Parkinson disease
"Parkinson disease"[MeSH Terms] AND management
Parkinson disease 2025 guidelines treatment pathophysiology
Parkinson Disease - Comprehensive Overview
Definition & Epidemiology
- Guyton and Hall Textbook of Medical Physiology, p. 712
- Robbins & Kumar Basic Pathology, p. 854
Pathology & Morphology
Gross Findings
- Pallor of the substantia nigra (SN) and locus coeruleus - the result of loss of melanin-containing pigmented neurons.
Microscopic Hallmark: Lewy Bodies
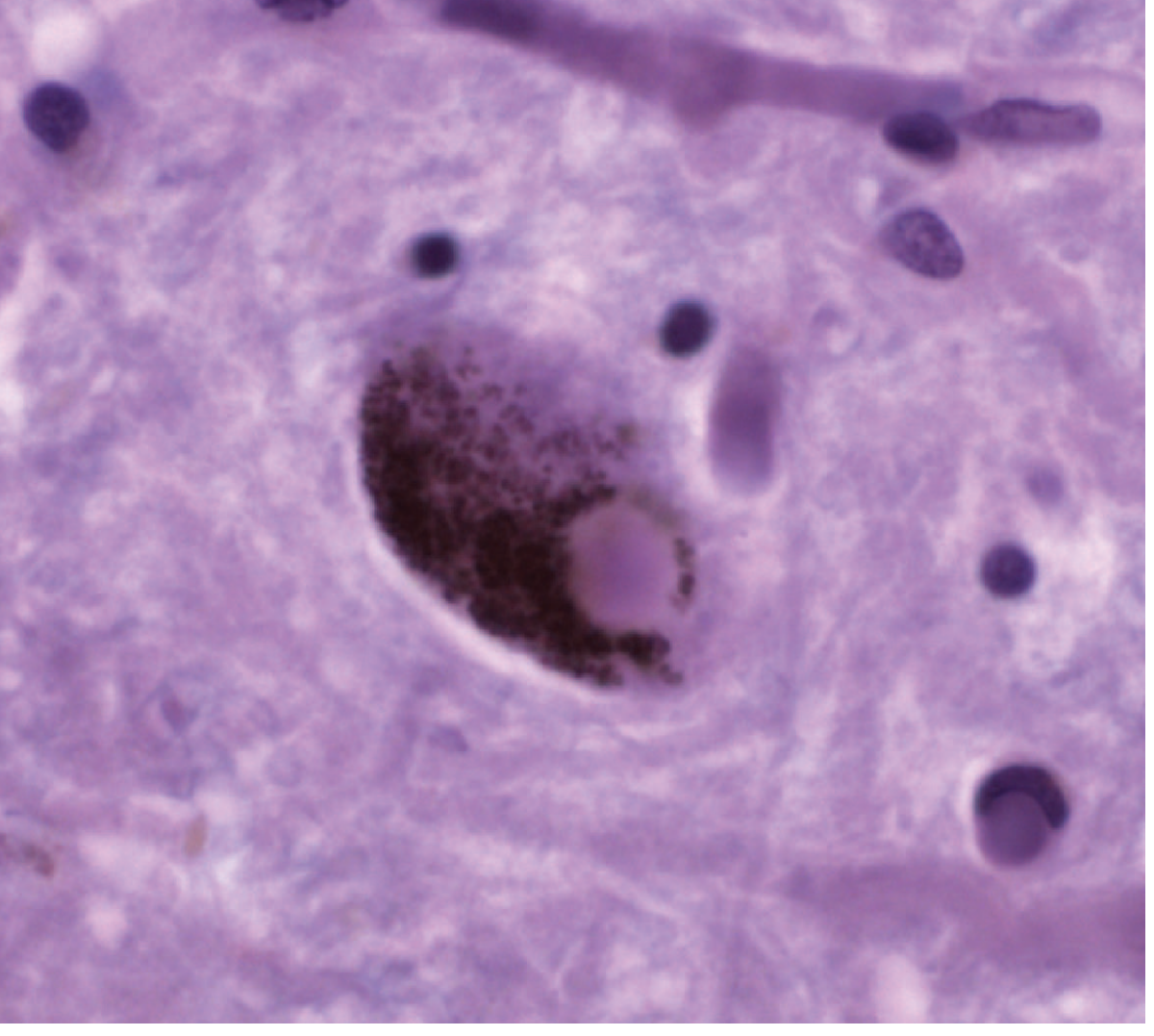
- Fine filaments of alpha-synuclein (α-syn) (main component)
- Neurofilaments and ubiquitin
- Robbins & Kumar Basic Pathology, p. 854
Pathogenesis
The Alpha-Synuclein / Prion Hypothesis
- It misfolds and forms β-sheet-rich toxic oligomers
- These polymerize into amyloid aggregates (Lewy bodies)
- The aggregates spread in a prion-like manner to connected neurons
- Injection of purified α-syn fibrils into rodent striatum produces Lewy pathology, neurodegeneration, and spread to anatomically connected sites
The Braak Hypothesis
- Harrison's Principles of Internal Medicine 22E, p. 3542
The GBA1 / Lysosomal Pathway
- GBA1 variants (encoding glucocerebrosidase) are the most important genetic risk factor for PD
- Reduced GCase activity impairs lysosomal clearance of α-syn
- Accumulating α-syn inhibits lysosomal function further → a vicious cycle
- This pathway is disrupted even in sporadic PD without GBA1 mutations
Other Genetic Factors
| Gene | Mutation type | Effect |
|---|---|---|
| SNCA (α-synuclein) | Point mutations, duplications | Autosomal dominant PD |
| LRRK2 (leucine-rich repeat kinase 2) | Gain-of-function | Most common cause of autosomal dominant PD |
| Parkin, PINK1 | Loss-of-function | Autosomal recessive, early-onset PD |
| GBA1 | Heterozygous variants | Risk factor; faster progression |
- Harrison's Principles of Internal Medicine 22E; Robbins & Kumar Basic Pathology
Basal Ganglia Circuit Disruption
- Overly activates the subthalamic nucleus (STN)
- Increases inhibitory output from the globus pallidus interna (GPi)
- Suppresses thalamic activity → reduced motor cortex activation → bradykinesia and rigidity
- Guyton and Hall Textbook of Medical Physiology, p. 712
Clinical Features
Cardinal Motor Signs (TRAP)
| Feature | Description |
|---|---|
| Tremor | Resting tremor, 3-6 Hz ("pill-rolling"), asymmetric, disappears with movement |
| Rigidity | "Lead-pipe" or "cogwheel" rigidity throughout range of motion |
| Akinesia/Bradykinesia | Slowness, reduced amplitude of movements - most disabling feature |
| Postural instability | Impaired postural reflexes → falls (appears later in disease) |
Other Motor Features
- Micrographia (small, cramped writing)
- Hypomimia (masked facies)
- Hypophonia (soft, monotone speech)
- Festinating gait (short, shuffling steps with forward lean)
- Freezing of gait (feet feel glued to floor)
- Dysphagia - present objectively in up to 82% of patients, associated with risk of aspiration pneumonia
Non-Motor Features (often precede motor symptoms)
-
Hyposmia/Anosmia - may antedate diagnosis by years
-
REM sleep behavior disorder (RBD) - acting out dreams; 40% develop PD or related synucleinopathy within 10 years
-
Constipation - due to involvement of enteric neurons
-
Depression and anxiety
-
Autonomic dysfunction - orthostatic hypotension, urinary dysfunction, sexual dysfunction
-
Cognitive impairment - from mild deficits to frank dementia in advanced disease
-
Drooling - due to reduced swallowing, not excessive production
-
Guyton and Hall Textbook of Medical Physiology; Adams and Victor's Principles of Neurology 12th Ed.
Diagnosis
- Early falls (PSP)
- Autonomic failure early (MSA)
- Poor/no levodopa response
- Rapid progression
- Symmetry from onset
Treatment
Pharmacological - Dopaminergic Therapy
- Still the most effective symptomatic agent; carbidopa inhibits peripheral DOPA decarboxylase, reducing nausea and increasing CNS availability
- Most effective for bradykinesia and rigidity; less effective for tremor and non-motor features
- Standard starting dose: carbidopa/levodopa 25/100 mg three times daily
- Limitations with long-term use: motor fluctuations
- Wearing-off: benefit shortens before next dose
- On-off fluctuations: unpredictable swings between mobile "on" and immobile "off" states
- Peak-dose dyskinesias: involuntary choreiform movements at maximal drug effect
- Diphasic dyskinesias: at rising and falling levodopa levels Risk factors: younger age, higher doses, female sex, more severe disease.
- Include pramipexole, ropinirole (oral), rotigotine (patch), apomorphine (injection/infusion)
- Preferred in younger patients to delay levodopa introduction and reduce dyskinesia risk
- Side effects: hallucinations, impulse control disorders, daytime somnolence, orthostatic hypotension
- Avoid in elderly patients due to neuropsychiatric side effects
- 2021 AAN guidelines allow early DA use as an alternative to levodopa in appropriate patients
- Inhibit monoamine oxidase B → reduce dopamine degradation
- Mild symptomatic benefit; may have neuroprotective properties (unproven)
- Can be used as monotherapy in early disease or as adjunct
- Inhibit catechol-O-methyltransferase → prolong levodopa effect
- Used as adjunct to reduce wearing-off
-
NMDA receptor antagonist
-
Used for dyskinesia management; also has mild antiparkinsonian effect
-
Harrison's Principles of Internal Medicine 22E; Guyton and Hall; Textbook of Family Medicine 9e
Surgical Treatment: Deep Brain Stimulation (DBS)
| Target | Advantages |
|---|---|
| STN (subthalamic nucleus) | Larger off-state motor benefit; allows larger medication reduction |
| GPi (globus pallidus interna) | Better dyskinesia suppression; safer neuropsychiatric profile; better long-term flexibility |
- Bradley and Daroff's Neurology in Clinical Practice, p. 652
Non-Pharmacological Treatment
- Exercise - strong evidence for motor benefit; network meta-analysis (2025, PMID 39880702) supports aerobic and resistance exercise as most effective
- Virtual reality training - evidence from 2025 meta-analysis (PMID 40142335) supports balance improvement
- Speech therapy - for hypophonia and dysphagia
- Physiotherapy - gait training, falls prevention
- Occupational therapy
- Dietitian input - aspiration risk, weight management
Emerging / Experimental Therapies
- α-Synuclein targeting: antibodies, small molecules, gene knockdown (multiple trials ongoing)
- GBA1-targeted therapy: GCase enhancers, substrate reduction therapy
- LRRK2 inhibitors: in clinical trials
- Focused ultrasound: thalamotomy for tremor, pallidotomy for dyskinesia
- Cell transplantation: dopaminergic neuron transplants (historical trials; renewed interest with iPSC-derived neurons)
Prognosis & Disease Course
Summary Table
| Domain | Key Points |
|---|---|
| Pathology | Loss of SNc dopaminergic neurons; Lewy bodies (α-synuclein + ubiquitin) |
| Pathogenesis | α-Syn misfolding, prion-like spread, Braak staging (gut→vagus→brain), GBA1/lysosomal dysfunction |
| Motor features | Resting tremor, rigidity, bradykinesia, postural instability (TRAP) |
| Non-motor | Anosmia, RBD, constipation, depression, autonomic dysfunction, dementia |
| 1st-line drug | Levodopa/carbidopa (most effective); DAs for younger patients |
| Complications | Wearing-off, on-off, peak-dose dyskinesia |
| Surgery | DBS (STN or GPi) for medically refractory motor complications |
| Key genetics | SNCA, LRRK2 (dominant); Parkin, PINK1 (recessive); GBA1 (risk factor) |
Recent evidence note (2025): A network meta-analysis (PMID 39880702) found that combined aerobic + resistance exercise provides the greatest motor benefit in PD. A meta-analysis on anxiety management in PD (PMID 40568748) highlights the importance of addressing non-motor psychiatric symptoms systematically.
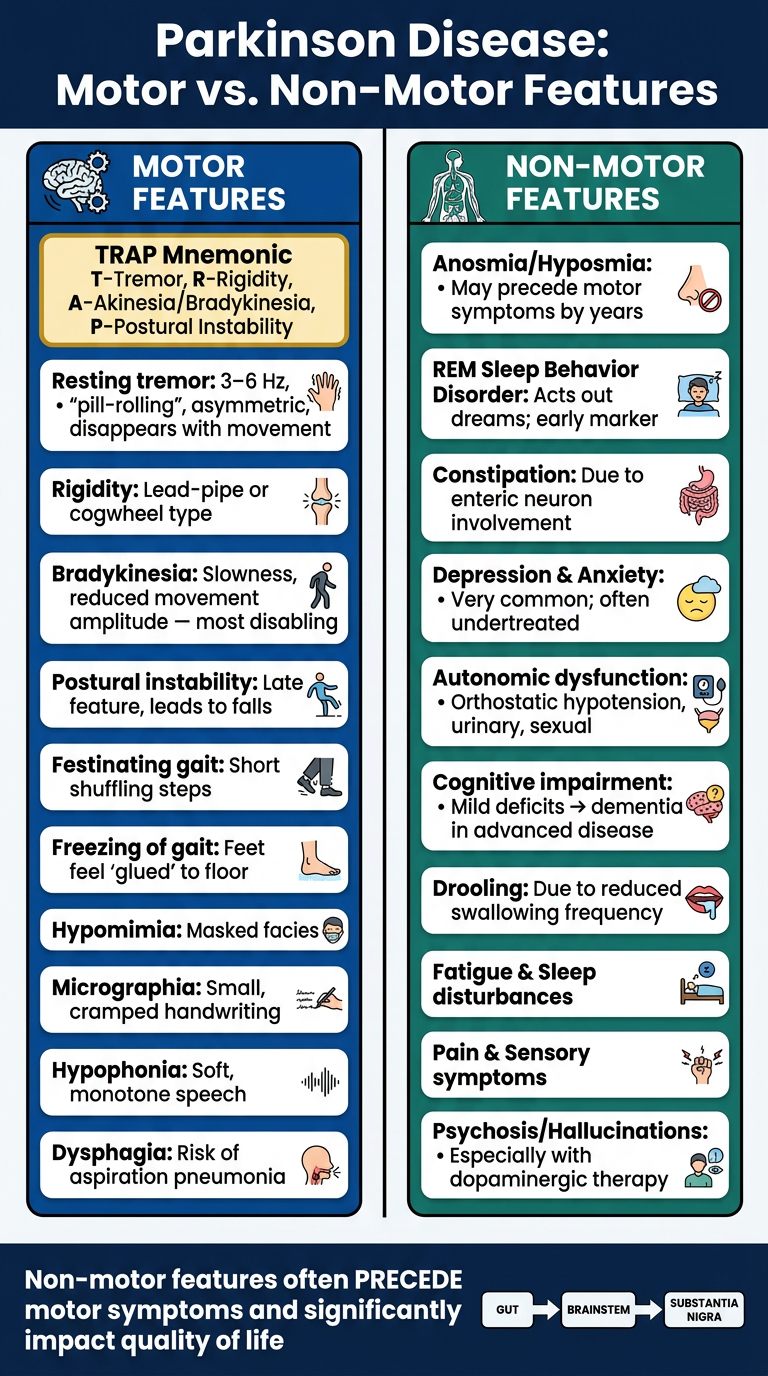
Create a visual summary poster comparing PD motor vs. non-motor features
A clean, professional medical education poster titled "Parkinson Disease: Motor vs. Non-Motor Features". Split into two bold vertical columns side by side. Left column has a dark blue header "MOTOR FEATURES" with a brain/movement icon. Right column has a dark teal/green header "NON-MOTOR FEATURES" with a nerve/body icon. Left column (Motor Features) lists in white cards on dark blue background: - TRAP Mnemonic highlighted in gold box: T-Tremor, R-Rigidity, A-Akinesia/Bradykinesia, P-Postural Instability - Resting tremor: 3–6 Hz, "pill-rolling", asymmetric, disappears with movement - Rigidity: Lead-pipe or cogwheel type - Bradykinesia: Slowness, reduced movement amplitude — most disabling - Postural instability: Late feature, leads to falls - Festinating gait: Short shuffling steps - Freezing of gait: Feet feel "glued" to floor - Hypomimia: Masked facies - Micrographia: Small, cramped handwriting - Hypophonia: Soft, monotone speech - Dysphagia: Risk of aspiration pneumonia Right column (Non-Motor Features) lists in white cards on dark teal background: - Anosmia/Hyposmia: May precede motor symptoms by years - REM Sleep Behavior Disorder: Acts out dreams; early marker - Constipation: Due to enteric neuron involvement - Depression & Anxiety: Very common; often undertreated - Autonomic dysfunction: Orthostatic hypotension, urinary, sexual - Cognitive impairment: Mild deficits → dementia in advanced disease - Drooling: Due to reduced swallowing frequency - Fatigue & Sleep disturbances - Pain & Sensory symptoms - Psychosis/Hallucinations: Especially with dopaminergic therapy At the bottom, a footer banner in dark navy: "Non-motor features often PRECEDE motor symptoms and significantly impact quality of life" with a small Braak staging arrow diagram showing gut → brainstem → substantia nigra. Clean, bold fonts, medical illustration style, high contrast, suitable for a hospital teaching wall.