adrenal glands
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compose a thorough answer.
Adrenal Glands
Overview
The paired adrenal (suprarenal) glands sit atop the superior pole of each kidney in the retroperitoneal space. Each weighs approximately 4 g. Despite their small size, they receive one of the highest rates of blood flow per gram of any organ in the body. Each gland is functionally two distinct organs - an outer cortex and an inner medulla - with different embryological origins, structures, and hormonal products.
- Medical Physiology (Barrett), p. 50-1
Embryology
| Region | Embryological Origin | Key Point |
|---|---|---|
| Cortex | Mesoderm (coelomic epithelium) | Differentiates by gestational week 8; fetal cortex involutes after birth |
| Medulla | Neural crest cells | Migrate into developing cortex; differentiate into chromaffin cells |
The fetal adrenal cortex is distinct from the adult cortex and is responsible for steroid production throughout intrauterine life. It involutes soon after birth and is replaced by the three-layered adult cortex.
- Langman's Medical Embryology; Costanzo Physiology 7e, p. 431
Gross Anatomy & Blood Supply
The adrenal gland has no hilum. Blood enters via three suprarenal arteries arising from larger abdominal vessels, which penetrate the capsule independently and immediately branch into a subcapsular arterial plexus. From there, separate arterioles supply the cortex and medulla. Notably, the medulla receives a dual blood supply:
- Direct arterial blood from medullary arterioles
- Venous blood draining from cortical capillaries (meaning medullary chromaffin cells are exposed to high concentrations of cortical steroids)
Venous drainage is via the suprarenal veins.
- Junqueira's Basic Histology 17e, p. 1020
Adrenal Cortex (80% of gland mass)
The cortex has three concentric zones, each producing distinct hormones:
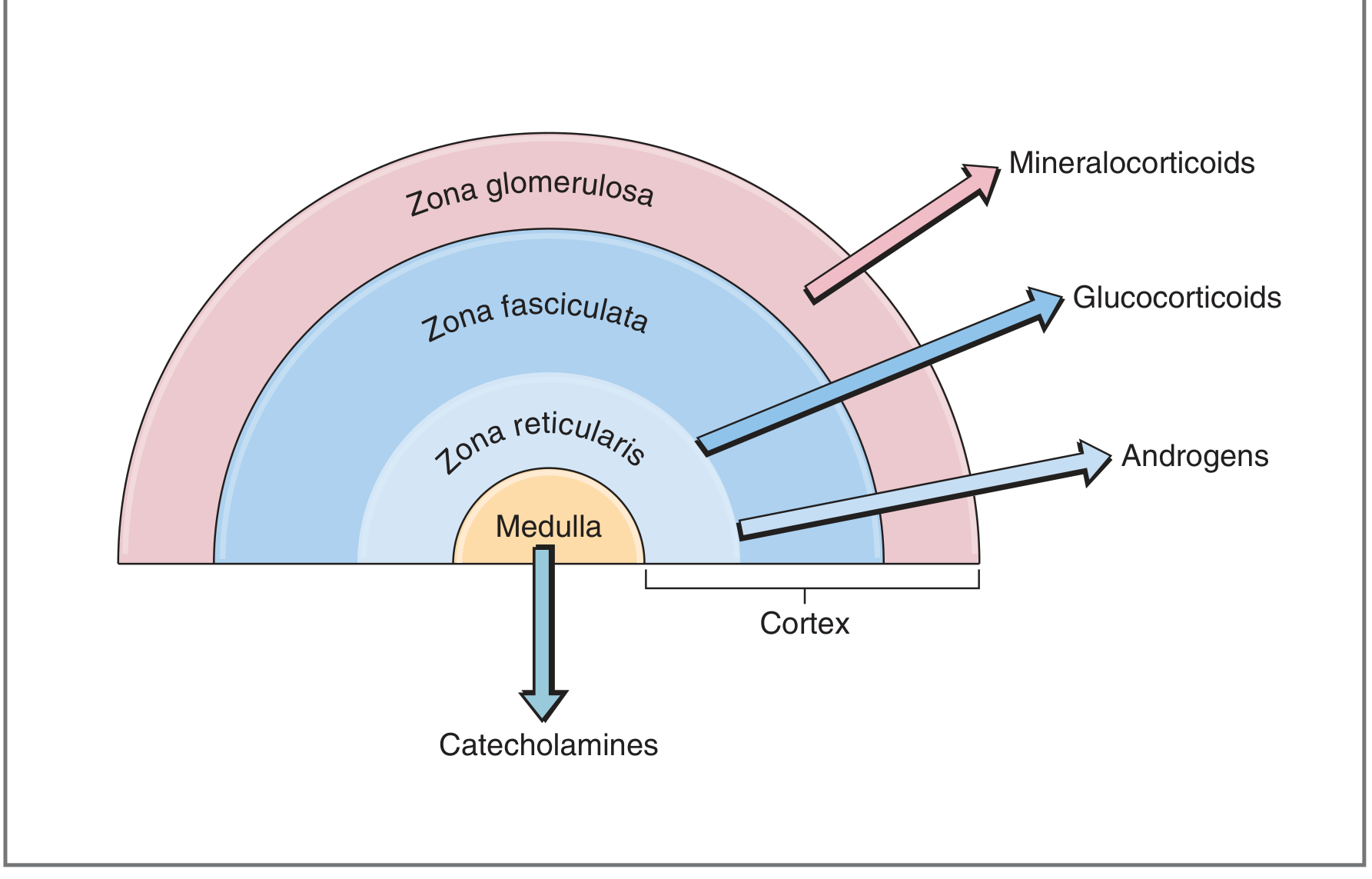
The Three Zones (GFR mnemonic - outside to inside)
| Zone | Location | Hormone | Class |
|---|---|---|---|
| Zona Glomerulosa | Outermost | Aldosterone | Mineralocorticoid |
| Zona Fasciculata | Middle (widest) | Cortisol | Glucocorticoid |
| Zona Reticularis | Innermost | DHEA, DHEAS, Androstenedione | Androgens |
All cortical steroids are synthesized from cholesterol as the precursor.
Histology of Cortical Cells
Cortical cells (adrenocortical cells) share features typical of all steroid-secreting cells:
-
Acidophilic cytoplasm rich in lipid droplets (cholesterol esters)
-
Abundant smooth ER (SER) - contains enzymes for cholesterol synthesis and steroid conversion
-
Mitochondria with tubular/vesicular cristae (not the usual shelf-like cristae) - contain enzymes for cholesterol → pregnenolone conversion and other steroidogenic steps
-
Steroids are not stored in granules - as lipid-soluble molecules, they diffuse freely across the plasma membrane
-
Junqueira's Basic Histology 17e, p. 1021
Cortisol (Glucocorticoid)
Synthesis: Zona fasciculata and (to a lesser degree) zona reticularis.
Key actions across body tissues:
- Liver: Activates gluconeogenesis; promotes glycogen synthesis
- Muscle/adipose: Mobilizes amino acids and fatty acids (catabolic)
- Immune system: Anti-inflammatory; suppresses lymphocyte and eosinophil activity; stabilizes mast cell membranes
- Bone: Inhibits osteoblasts; chronic excess causes osteoporosis
- CNS: Affects mood, cognition, appetite
- Cardiovascular: Supports vascular responsiveness to catecholamines
Regulation - HPA Axis:
Hypothalamus → CRH (41-amino acid peptide, from paraventricular nuclei) → Anterior pituitary corticotrophs → ACTH → Adrenal cortex → Cortisol
- Cortisol exerts negative feedback at three points: (1) directly inhibits hypothalamic CRH, (2) via hippocampal neurons that synapse on the hypothalamus, (3) inhibits CRH action on the anterior pituitary
Diurnal rhythm: Cortisol secretion is pulsatile (~10 bursts/day). Levels are lowest around midnight and peak just before awakening (~8 AM). The pre-awakening burst accounts for ~50% of total daily cortisol output. This pattern is driven by ACTH, which in turn is driven by CRH. The diurnal rhythm is abolished by coma, blindness, or constant light/dark exposure.
- Costanzo Physiology 7e, pp. 435-436
Aldosterone (Mineralocorticoid)
Synthesis: Zona glomerulosa exclusively.
Actions: Promotes Na⁺ reabsorption and K⁺ excretion in the renal collecting tubule; increases water retention; raises blood pressure.
Regulation: Primarily by the renin-angiotensin-aldosterone system (RAAS) and plasma K⁺ levels. ACTH plays only a minor role (unlike with cortisol).
Structurally, aldosterone differs from cortisol by lacking the -OH at C17 and having an aldehyde group at C18 - a seemingly minor difference that completely eliminates glucocorticoid activity at physiological concentrations.
Adrenal Androgens
Synthesis: Zona reticularis.
Key hormones: Dehydroepiandrosterone (DHEA), DHEAS, and androstenedione - all weak androgens (far weaker than testosterone or DHT).
- DHEAS circulates at the highest concentration of any adrenal steroid and shows no diurnal variation
- Plasma DHEA follows the same diurnal pattern as cortisol
- In women, adrenal androgens are a significant source of androgen activity
Adrenal Medulla (20% of gland mass)
Origin: Neuroectoderm (neural crest). The medulla is essentially a modified sympathetic ganglion.
Cell type: Chromaffin cells (named for their staining with chromium salts), innervated by preganglionic sympathetic neurons.
Hormones: Catecholamines
- Epinephrine (adrenaline): ~80% of output; synthesized from norepinephrine via PNMT enzyme (induced by high local cortisol from cortical venous blood)
- Norepinephrine: ~20% of output; also produced at sympathetic nerve terminals elsewhere
Catecholamines are stored in granular complexes with chromogranins (49 kDa proteins), Ca²⁺, and ATP, and released by exocytosis in response to preganglionic stimulation.
Fight-or-flight effects:
-
Epinephrine: increases heart rate, dilates bronchioles, dilates skeletal/cardiac muscle arteries, elevates blood glucose (glycogenolysis)
-
Norepinephrine: constricts splanchnic and skin vessels, redirects blood to heart, muscles, and brain
-
Both: promote glycogenolysis and lipolysis
-
Junqueira's Basic Histology 17e, p. 1027
Clinical Summary: Major Disorders
| Disorder | Pathology | Key Features |
|---|---|---|
| Cushing's syndrome | Cortisol excess | Central obesity, moon face, striae, hypertension, hyperglycemia, osteoporosis |
| Addison's disease | Primary adrenocortical insufficiency | Fatigue, hypotension, hyponatremia, hyperkalemia, hyperpigmentation (↑ ACTH/MSH) |
| Primary hyperaldosteronism (Conn's) | Aldosterone excess | Hypertension, hypokalemia, metabolic alkalosis |
| Pheochromocytoma | Catecholamine-secreting medullary tumor | Paroxysmal hypertension, headache, sweating, palpitations; "10% tumor" |
| Congenital adrenal hyperplasia (CAH) | Enzyme defect in steroidogenesis (usually 21-hydroxylase) | Virilization, salt-wasting, ↑ ACTH driving adrenal hyperplasia |
Summary Table
| Feature | Cortex | Medulla |
|---|---|---|
| Origin | Mesoderm | Neural crest (neuroectoderm) |
| % of gland | ~80% | ~20% |
| Hormones | Cortisol, aldosterone, DHEA | Epinephrine, norepinephrine |
| Hormone class | Steroids | Catecholamines (amine) |
| Storage | Not stored; diffuse freely | Stored in chromaffin granules |
| Regulation | HPA axis (cortisol/androgens); RAAS + K⁺ (aldosterone) | Sympathetic innervation |
This is a shared conversation. Sign in to Orris to start your own chat.