Parkinson and parkinsonism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Parkinson's Disease and Parkinsonism
1. Parkinsonism: The Syndrome
Parkinsonism is a clinical syndrome defined by six cardinal features:
- Tremor at rest
- Bradykinesia (slowness of movement)
- Rigidity
- Loss of postural reflexes
- Flexed posture
- Freezing (motor blocks)
The four major features form the acronym TRAP: Tremor, Rigidity, Akinesia, Postural disturbances.
Parkinsonism is a syndrome, not a single disease. Parkinson's disease (PD) is merely the most common cause.
- Bradley and Daroff's Neurology in Clinical Practice
2. Parkinson's Disease (PD): Overview
Epidemiology
-
Second most common neurodegenerative disorder after Alzheimer's disease
-
Affects ~1 in 1000 in the general population; at least 1% of persons over 65
-
Slight male predominance (3:2 ratio)
-
Prevalence is rising with global aging; age-adjusted mortality increased 2.4% per year between 1999 and 2019
-
Goldman-Cecil Medicine
Pathobiology
Genetic factors (~10% of cases)
| Gene (PARK locus) | Inheritance | Protein | Notes |
|---|---|---|---|
| PARK-SNCA (PARK1) | AD | α-Synuclein | Missense mutations + duplications |
| PARK-Parkin (PARK2) | AR | Parkin | Up to 50% of early-onset PD |
| PARK-PINK1 (PARK6) | AR | PINK1 kinase | Early onset |
| PARK-DJ-1 (PARK7) | AR | DJ-1 | Early onset |
| PARK-LRRK2 (PARK8) | AD | LRRK2 (dardarin) | Most common AD form; common in N. Africans, Ashkenazi Jews |
| GBA1 | Risk allele | Glucocerebrosidase | Higher dementia risk, faster progression |
AR = autosomal recessive; AD = autosomal dominant
Environmental factors: Pesticides, heavy metals, and traumatic brain injury increase risk. The selective neurotoxin MPTP (oxidized to MPP+) causes acute parkinsonism by inhibiting mitochondrial complex I, directly implicating oxidative stress.
Other proposed mechanisms: Mitochondrial dysfunction, protein misfolding/aggregation, excitotoxicity, neuroinflammation, apoptosis, and loss of trophic support.
- Goldman-Cecil Medicine; Bradley and Daroff's Neurology
Pathology
The hallmark is loss of pigmented dopaminergic neurons in the substantia nigra pars compacta (SNpc) of the midbrain, with resultant dopamine depletion in the neostriatum (especially the putamen).
Key threshold: approximately 60% of dopaminergic neurons must degenerate before classic motor features appear.
The pathological signature is the Lewy body - a cytoplasmic inclusion composed primarily of aggregated α-synuclein, seen in surviving neurons of the SNpc and other areas.
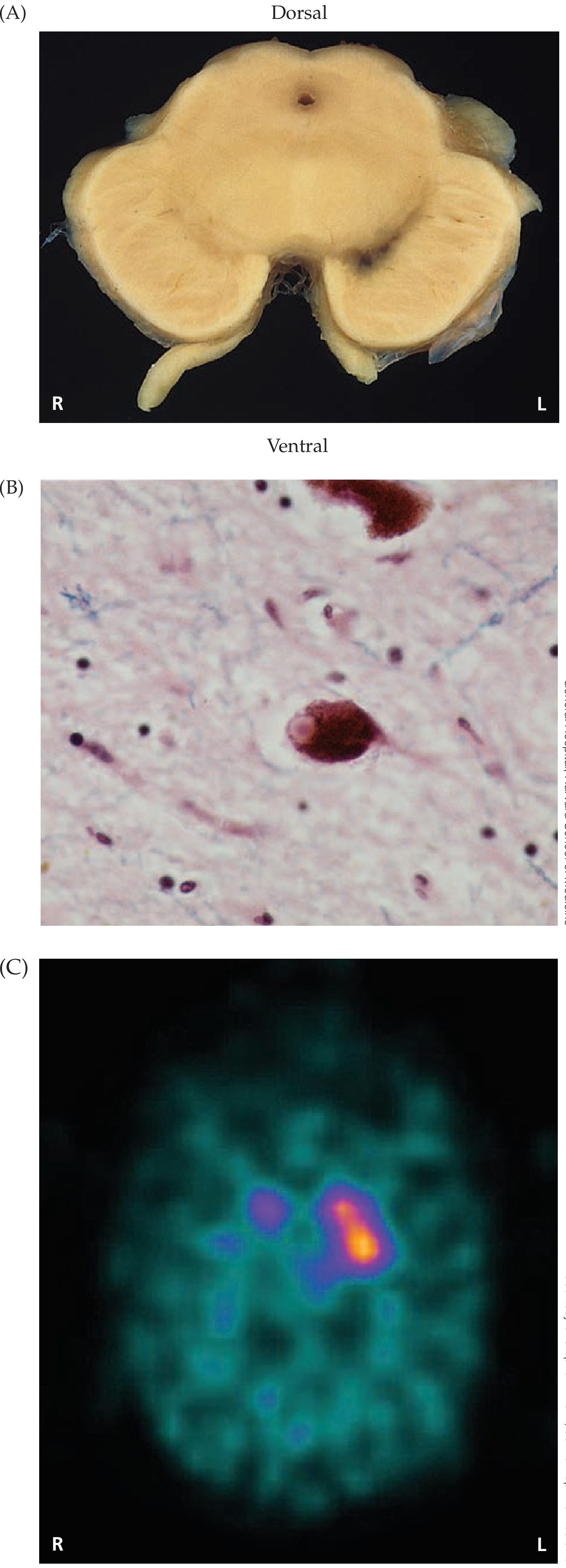
Fig. Parkinson's disease: (A) Gross depigmentation of substantia nigra, (B) Lewy body in dopaminergic neuron, (C) Asymmetric DAT-SPECT scan showing unilateral striatal dopamine transporter loss.
Pathology spreads beyond the SNpc to involve brainstem nuclei, cortical regions, olfactory system, and peripheral autonomic neurons - explaining the many non-motor features. Disease may begin in the olfactory bulb and lower brainstem (Braak staging hypothesis), only later involving the SNpc.
- Goldman-Cecil Medicine; Neuroanatomy through Clinical Cases 3e
Clinical Manifestations
Prodromal / Premotor Phase
The disease begins years before motor symptoms. Early premotor markers include:
- Hyposmia/anosmia (olfactory degeneration - often the earliest sign)
- REM sleep behavior disorder (RBD)
- Constipation (autonomic/gut involvement)
- Depression and anxiety
- Restless leg syndrome
Motor Symptoms
Tremor:
- Classic 4-6 Hz pill-rolling resting tremor (suppressed with voluntary movement)
- Occurs in only ~80% of patients; up to 30% never develop tremor
- Typically begins asymmetrically (one limb/side), with asymmetry persisting throughout the disease
Bradykinesia/Akinesia:
- Reduced facial expression = masked facies (hypomimia)
- Hypophonia (soft voice) with hurried, muttering speech
- Micrographia (small handwriting)
- Slow saccades, broken smooth pursuit eye movements
- Decreased spontaneous blink rate
- Positive Myerson's sign (failure to suppress blinking when glabella is tapped)
Rigidity:
- Cogwheel rigidity (ratchet-like resistance to passive movement, due to tremor superimposed on "lead-pipe" rigidity)
- Stooped posture
Postural instability and gait:
- Festinating gait: shuffling, small steps, with tendency to fall forward (anteropulsion) or backward (retropulsion)
- Freezing (inability to initiate gait, especially in doorways)
- En bloc turning (without normal torso rotation)
- Inability to rise from a chair without using hands
Non-Motor Symptoms
| System | Features |
|---|---|
| Cognitive | Mild executive dysfunction early; dementia (15-40%) late; bradyphrenia |
| Psychiatric | Depression, anxiety, hallucinations (especially with dopaminergic drugs), impulse control disorders |
| Autonomic | Orthostatic hypotension, urinary urgency/frequency, constipation, erectile dysfunction, seborrhea, hypersalivation |
| Sleep | RBD, excessive daytime sleepiness |
| Sensory | Pain, anosmia |
- Neuroanatomy through Clinical Cases 3e; Goldman-Cecil Medicine
Diagnosis
Diagnosis is clinical, based on the presence of parkinsonism with typical features (asymmetric onset, rest tremor, levodopa responsiveness).
Red flags suggesting alternative diagnoses:
- Early postural instability and falls
- Rapid progression
- Symmetrical onset
- No response to levodopa
- Prominent early dementia or hallucinations
- Supranuclear gaze palsy
- Early autonomic failure
Investigations:
- DaT-SPECT (dopamine transporter scintigraphy): shows asymmetric reduced striatal uptake in PD (see image above); normal in drug-induced parkinsonism
- Genetic testing: considered in early-onset disease or strong family history
- MRI: usually normal in PD but helps exclude structural causes
Treatment
Symptomatic Pharmacotherapy
1. Levodopa + Carbidopa (most effective)
- Carbidopa is a peripheral DOPA decarboxylase inhibitor that prevents peripheral conversion of levodopa, reducing side effects and increasing CNS availability
- Gold standard; no benefit in delaying initiation
- Motor complications develop in up to 50% within 2-5 years:
- Wearing off (end-of-dose akinesia, morning akinesia)
- On-off fluctuations
- Peak-dose dyskinesia (chorea/athetosis at maximum drug levels)
- Diphasic dyskinesia (at beginning and end of dose)
- Off-period dystonia (foot/leg cramps, typically in morning)
- Even after 20+ years of disease, most classic motor features continue to respond to levodopa
2. Dopamine Agonists (e.g., pramipexole, ropinirole, rotigotine patch)
- Preferred as initial monotherapy in patients under 65 who are cognitively intact
- Delays onset of motor complications vs levodopa, but less efficacious
- Higher risk of hallucinations, impulse control disorders (hypersexuality, gambling), edema
- All patients eventually need levodopa
3. MAO-B Inhibitors (selegiline, rasagiline, safinamide)
- Inhibit dopamine breakdown; used as add-on therapy to reduce wearing-off
4. COMT Inhibitors (entacapone, opicapone)
- Block catechol-O-methyltransferase, extending levodopa effect; used in wearing-off
5. Anticholinergics (trihexyphenidyl, benztropine)
- Useful mainly for tremor in younger patients; avoided in elderly (confusion, urinary retention)
6. Amantadine
- NMDA antagonist; modestly reduces motor symptoms; useful for levodopa-induced dyskinesias
Surgical Treatment: Deep Brain Stimulation (DBS)
Indicated when motor complications cannot be adequately controlled medically.
Targets:
| Target | Key Benefits | Relative Disadvantages |
|---|---|---|
| Subthalamic nucleus (STN) | Larger benefit in "off" state; allows greater levodopa reduction | Higher risk of neuropsychiatric effects |
| Globus pallidus internus (GPi) | Better dyskinesia suppression; more flexible long-term; safer neuropsychiatric profile; better for "brittle dyskinesia" | Less medication reduction |
Both STN and GPi DBS have shown similar overall motor outcomes in randomized trials.
Focused ultrasound (FUS) thalamotomy/subthalamotomy is a newer non-invasive ablative option.
- Goldman-Cecil Medicine; Bradley and Daroff's Neurology
3. Differential Diagnosis of Parkinsonism
A. Parkinson-Plus Syndromes (Atypical Parkinsonism)
These are neurodegenerative disorders that share parkinsonian features but have additional signs and poor levodopa response.
| Syndrome | Key Features | Pathology |
|---|---|---|
| Progressive Supranuclear Palsy (PSP) | Early falls (backward), supranuclear vertical gaze palsy (especially downgaze), axial rigidity, pseudobulbar palsy | 4-repeat tau (tauopathy) |
| Multiple System Atrophy (MSA) | Cerebellar ataxia and/or autonomic failure (severe orthostasis, urinary dysfunction) + parkinsonism; Pisa syndrome, antecollis | α-Synuclein (glial cytoplasmic inclusions) |
| Corticobasal Degeneration (CBD) | Asymmetric limb apraxia, alien limb phenomenon, cortical sensory loss, dystonia | 4-repeat tau |
| Dementia with Lewy Bodies (DLB) | Fluctuating cognition, visual hallucinations, RBD, sensitivity to neuroleptics; parkinsonism less severe | Cortical Lewy bodies (α-synuclein) |
B. Secondary (Acquired) Parkinsonism
| Cause | Examples / Notes |
|---|---|
| Drug-induced (most common secondary cause) | Neuroleptics, metoclopramide, prochlorperazine, tetrabenazine, reserpine, flunarizine, lithium - normal DaT-SPECT |
| Vascular parkinsonism | Second most common form in movement clinics (~8%); "lower body parkinsonism" - gait dominant, broad-based shuffling, pyramidal signs, dementia; structural MRI abnormal in 90-100% |
| Toxic | MPTP, manganese, carbon monoxide, mercury |
| Infectious | Encephalitis lethargica (post-influenza), HIV, CJD |
| Structural | Normal-pressure hydrocephalus, brain tumor, subdural hematoma |
| Metabolic | Wilson's disease (copper), Fahr disease (basal ganglia calcification) |
C. Genetic Causes mimicking PD
- Wilson disease
- Huntington disease (rigid variant)
- Spinocerebellar ataxias (SCA-2, SCA-3)
- Neuroacanthocytosis
- Pantothenate kinase-associated neurodegeneration (Hallervorden-Spatz)
- Dopa-responsive dystonia (treatable - important to identify)
4. Key Distinguishing Points: PD vs. Parkinsonism
| Feature | Parkinson's Disease | Atypical / Secondary Parkinsonism |
|---|---|---|
| Onset | Asymmetric | Often symmetric |
| Tremor | Prominent resting tremor | Less prominent or absent |
| Levodopa response | Good, sustained | Poor or absent |
| Progression | Gradual (5-15 years) | Often faster |
| Postural instability | Late feature | Early feature |
| DaT-SPECT | Abnormal (asymmetric) | Abnormal (degenerative) or normal (drug-induced, vascular) |
| Pathological hallmark | Lewy bodies (α-synuclein) | Variable (tau, TDP-43, etc.) |
Recent Evidence (2024-2026)
A 2025 systematic review in Movement Disorders (PMID: 39927608) characterized genotype-phenotype relationships of GBA1 variants - the most common genetic risk factor - highlighting their association with faster motor progression and higher dementia rates. A 2025 meta-analysis in Nature Communications (PMID: 40335465) using machine learning identified consistent gut microbiome alterations in PD, supporting the gut-brain axis hypothesis of early disease propagation.
Sources:
- Goldman-Cecil Medicine, International Edition, Chapter 378
- Bradley and Daroff's Neurology in Clinical Practice, Chapters 24 and 96
- Neuroanatomy through Clinical Cases, 3rd ed., Chapter 16
Ok thanks
You're welcome! Feel free to ask if you want to go deeper on any aspect — such as a specific drug mechanism, the basal ganglia circuitry in detail, a particular Parkinson-plus syndrome, or surgical options. Happy to help anytime.
This is a shared conversation. Sign in to Orris to start your own chat.