Lumbar plexus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Let me compile it.
Lumbar Plexus
Formation and Location
The lumbar plexus is formed within (or posterior to) the substance of the psoas major muscle by the anterior rami of L1, L2, L3, and most of L4, with a variable contribution from T12 (subcostal nerve). It lies anterior to the transverse processes of the lumbar vertebrae.
The remaining part of L4 (the "pre-fixed" portion) joins with L5 to form the lumbosacral trunk, which descends over the ala of the sacrum to connect with the sacral plexus.
(Gray's Anatomy for Students, p. 462)
Schematic Diagram (Gray's Anatomy)
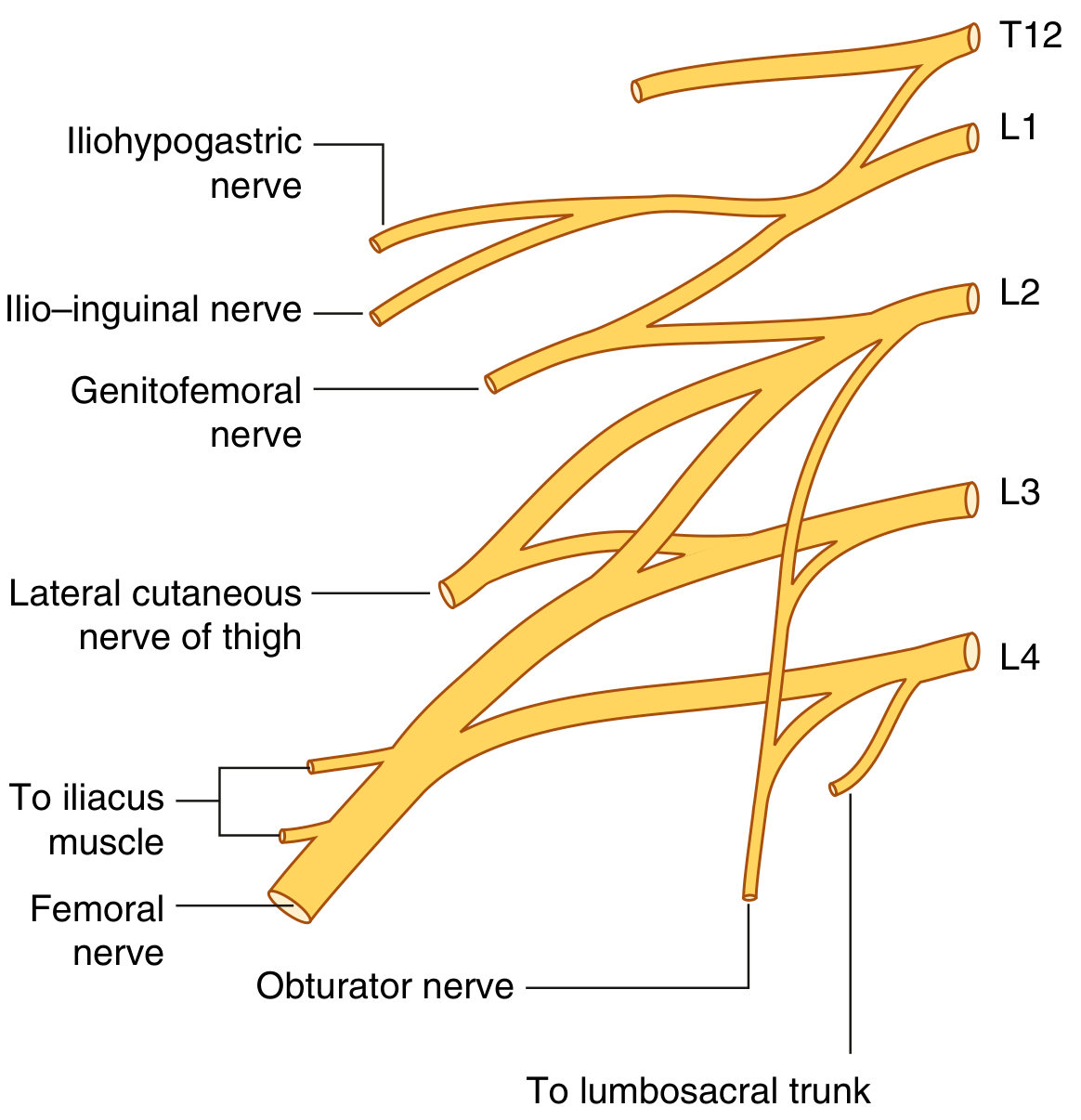
Fig. 4.177 - Lumbar Plexus (Gray's Anatomy for Students)
Branches - Summary Table
| Branch | Root | Motor | Sensory |
|---|---|---|---|
| Iliohypogastric | L1 | Internal oblique, transversus abdominis | Posterolateral gluteal skin; skin over pubic region |
| Ilio-inguinal | L1 | Internal oblique, transversus abdominis | Upper medial thigh; anterior scrotum/labium majus |
| Genitofemoral | L1, L2 | Cremaster muscle (genital branch) | Anterior scrotum or mons pubis/labium majus (genital); upper anterior thigh (femoral) |
| Lateral cutaneous nerve of thigh | L2, L3 | None (purely sensory) | Anterior and lateral thigh to the knee |
| Obturator | L2-L4 | Obturator externus, pectineus, adductors (longus, brevis, magnus), gracilis | Medial thigh |
| Femoral | L2-L4 | Iliacus, pectineus, sartorius, rectus femoris, vasti | Anterior thigh; medial leg (via saphenous nerve) |
(Gray's Anatomy for Students, p. 462; Imaging Anatomy - Bones, Joints, Vessels and Nerves, p. 398)
Relation to Psoas Major - Exit Points
The branches of the lumbar plexus emerge from the psoas in a predictable pattern:
- Anterior - Genitofemoral nerve (pierces the muscle to appear on its anterior surface)
- Lateral - Iliohypogastric, ilio-inguinal, lateral cutaneous nerve of thigh, and femoral nerve (the largest branch - exits from the lower lateral border)
- Medial - Obturator nerve and lumbosacral trunk
Lumbar Plexus in the Posterior Abdomen
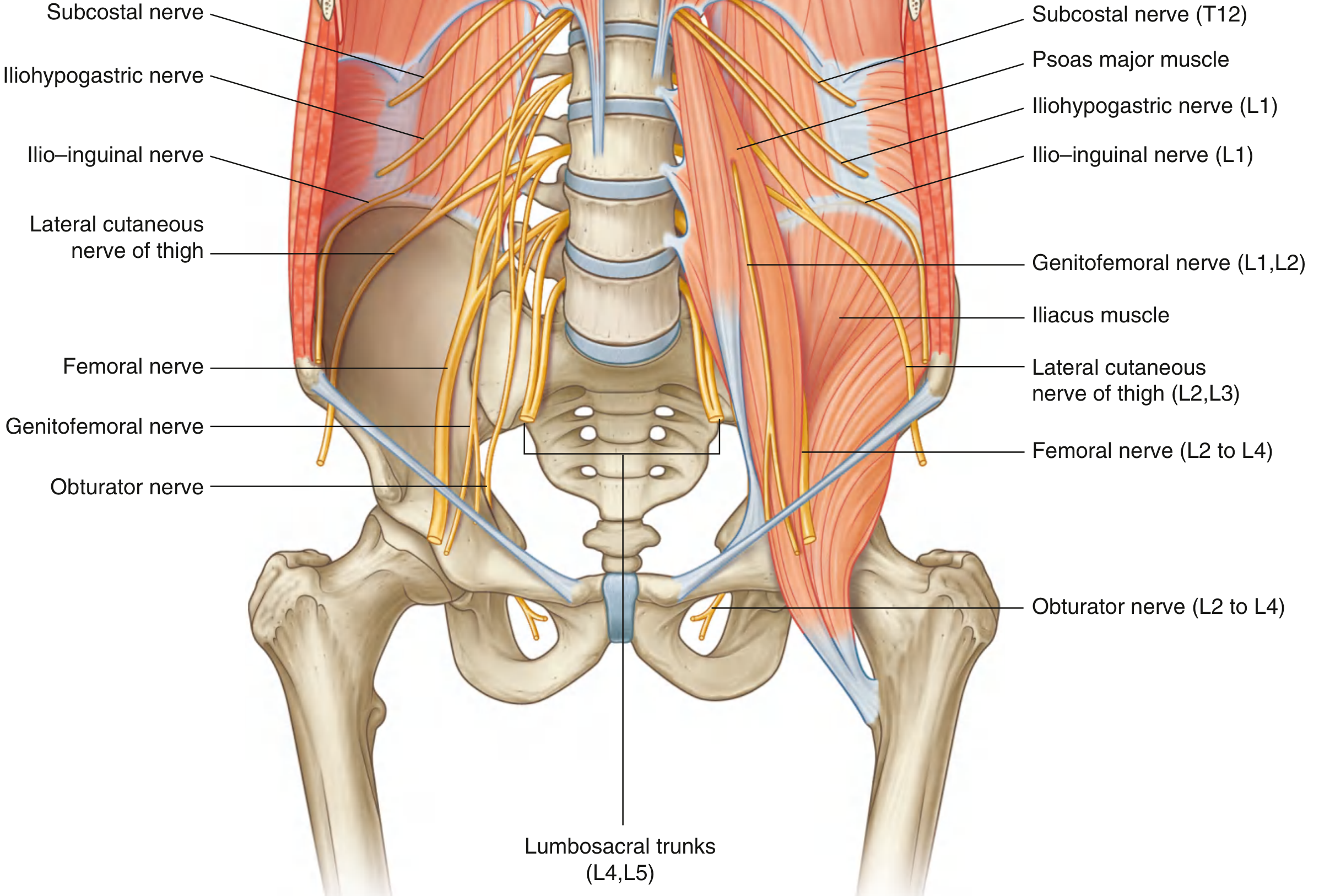
Fig. 4.178 - Lumbar Plexus in the Posterior Abdominal Region (Gray's Anatomy for Students)
Individual Branches in Detail
1. Iliohypogastric Nerve (L1)
Emerges from the lateral border of psoas, crosses quadratus lumborum (posterior to the kidney), and pierces transversus abdominis. Gives a lateral cutaneous branch to the posterolateral gluteal skin above the iliac crest, and an anterior cutaneous branch that pierces external oblique aponeurosis just above the superficial inguinal ring to supply the pubic skin.
2. Ilio-inguinal Nerve (L1)
Smaller than and inferior to the iliohypogastric. Runs a more oblique course across iliacus, pierces transversus abdominis and internal oblique, and enters the inguinal canal. Exits through the superficial inguinal ring alongside the spermatic cord - supplies the upper medial thigh, the root of the penis and anterior scrotum (male) or mons pubis and labium majus (female).
3. Genitofemoral Nerve (L1, L2)
Passes downward through psoas substance, emerges on its anterior surface, descends retroperitoneally posterior to the ureter. Divides into:
- Genital branch - enters inguinal canal via deep ring; supplies cremasteric muscle and scrotal/labial skin
- Femoral branch - passes posterior to inguinal ligament lateral to femoral artery; supplies skin of upper anterior thigh
4. Lateral Cutaneous Nerve of Thigh (L2, L3)
Purely sensory. Emerges from the lateral border of psoas, crosses iliacus obliquely toward the anterior superior iliac spine (ASIS), then passes posterior to the inguinal ligament to enter the thigh. Supplies the anterior and lateral thigh down to the knee. Entrapment near the ASIS causes meralgia paraesthetica.
5. Obturator Nerve (L2-L4)
Descends in psoas and emerges from its medial border near the pelvic brim. Passes posterior to the common iliac vessels, along the lateral pelvic wall, then through the obturator canal into the medial compartment of the thigh. Divides into anterior and posterior branches:
- Supplies all adductor muscles (adductor longus, brevis, magnus, gracilis, obturator externus, ± pectineus)
- Articular branches to the hip and knee joints
- Cutaneous supply to the medial thigh
6. Femoral Nerve (L2-L4) - Largest Branch
Descends through psoas and exits its lower lateral border, running in the groove between psoas and iliacus (deep to iliacus fascia). Passes posterior to the inguinal ligament (lateral to the femoral artery) to enter the femoral triangle. Immediately divides into multiple branches:
- Motor - iliacus, pectineus, sartorius, and all four quadriceps muscles
- Cutaneous - medial and intermediate cutaneous nerves to anterior thigh; saphenous nerve (longest branch) to medial leg and foot
- Articular - hip and knee joints
(Gray's Anatomy for Students, pp. 463-465)
Lumbosacral Plexus Overview (THIEME Atlas)
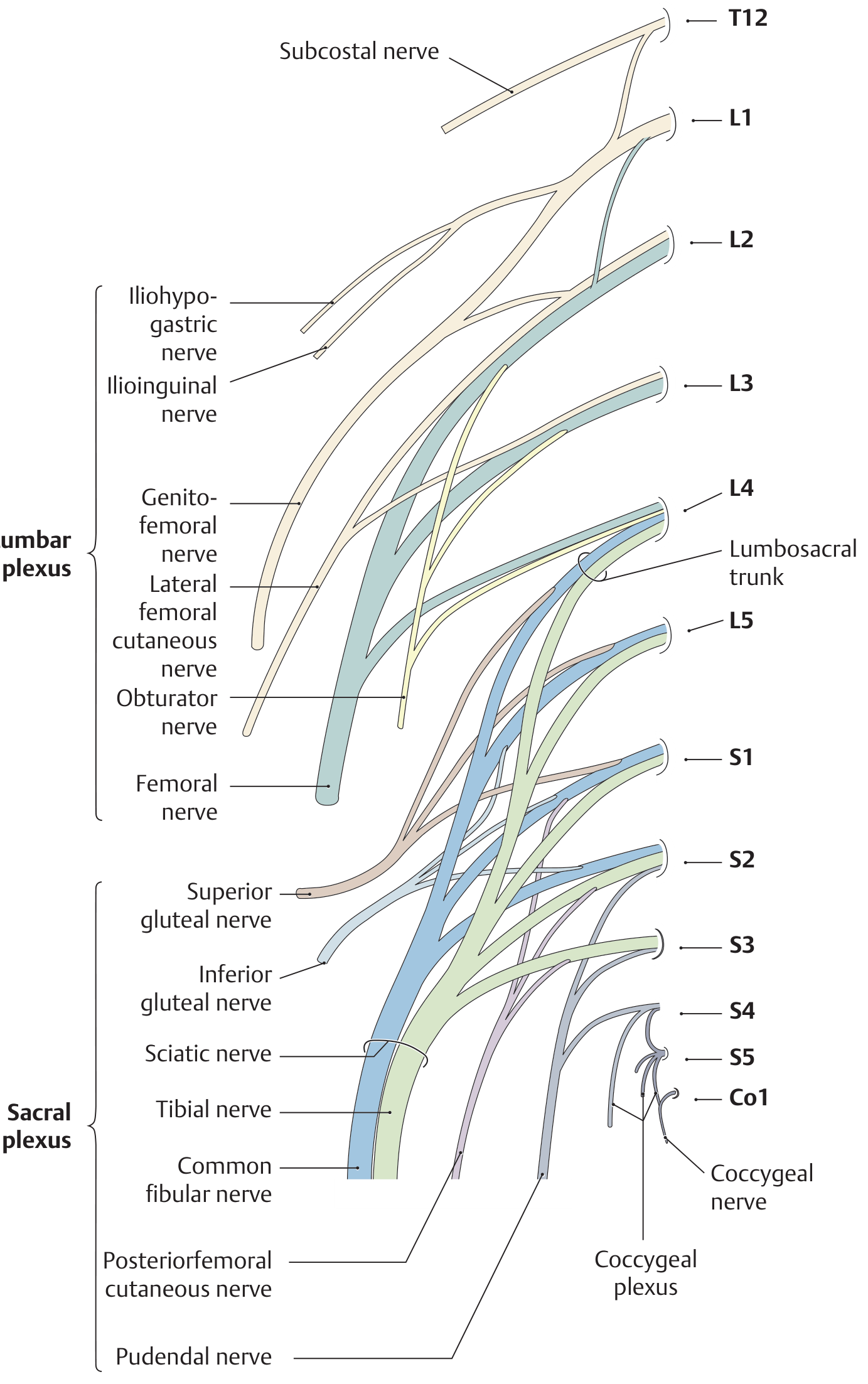
THIEME Atlas of Anatomy - Structure of the Lumbosacral Plexus
Cutaneous Distribution
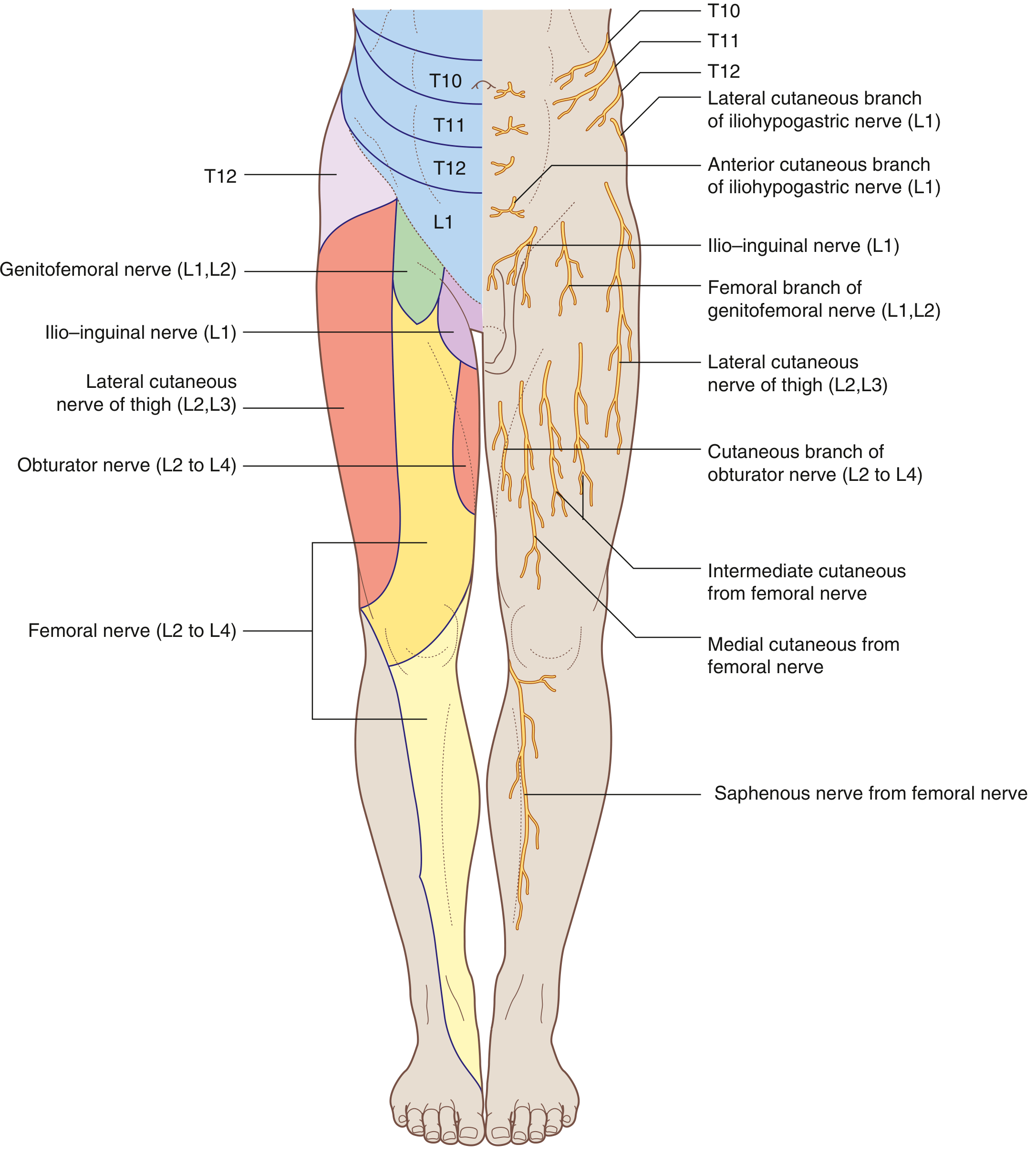
Fig. 4.179 - Cutaneous Distribution of Lumbar Plexus Nerves (Gray's Anatomy for Students)
Imaging of the Lumbar Plexus
On CT or MRI, the lumbar roots can be traced as they exit their neural foramina. Once the ventral rami enter the psoas, the plexus itself is difficult to visualize. Occasionally the femoral nerve is seen as a fascicular structure surrounded by fat along the posterior margin of psoas. The obturator nerve is usually the easiest branch to identify on imaging, seen medial to the psoas at the pelvic brim. (Imaging Anatomy - Bones, Joints, Vessels and Nerves, p. 398)
Clinical Points
Lumbar Plexopathy
Damage to the lumbar plexus (L2-L4) produces a characteristic combination of:
- Weakness of hip flexion (iliopsoas via femoral nerve), knee extension (quadriceps), and hip adduction (adductors via obturator)
- Sensory loss over the anteromedial thigh
- Absent or depressed knee jerk
- The co-occurrence of femoral and obturator territory deficits distinguishes plexopathy from a single nerve or single root lesion
Common Causes of Lumbar Plexus Injury
- Retroperitoneal hematoma (e.g., anticoagulated patients, iliopsoas hemorrhage)
- Pelvic malignancy or retroperitoneal lymphadenopathy
- Diabetic amyotrophy (Bruns-Garland syndrome)
- Surgical positioning (lithotomy position) or direct surgical trauma
- Psoas abscess
Specific Nerve Syndromes
| Syndrome | Nerve | Key Feature |
|---|---|---|
| Meralgia paraesthetica | Lateral cutaneous nerve of thigh | Burning/numbness on lateral thigh; entrapment near ASIS |
| Obturator nerve palsy | Obturator nerve | Adductor weakness; medial thigh pain (obturator hernia) |
| Femoral nerve palsy | Femoral nerve | Quadriceps weakness, absent knee jerk, anterior thigh numbness |
| Inguinal/groin pain post-surgery | Ilio-inguinal or iliohypogastric | Entrapment during herniorrhaphy or appendectomy |
(Bradley and Daroff's Neurology in Clinical Practice; Campbell's Operative Orthopaedics 15e)
Sources:
- Gray's Anatomy for Students (pp. 461-465)
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System (p. 555-556)
- Imaging Anatomy - Bones, Joints, Vessels and Nerves, Vol. 3 (p. 398)
- Bradley and Daroff's Neurology in Clinical Practice (p. 2616)
- Campbell's Operative Orthopaedics, 15th Ed. (2026)
This is a shared conversation. Sign in to Orris to start your own chat.