all common heart ecg
Reading File
Finding Sources
Searching the Web
common ECG patterns heart arrhythmias guide 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and images. Let me compile the complete ECG guide.
Common Heart ECG Patterns - Complete Guide
Source: Harrison's Principles of Internal Medicine 22E (2025), Braunwald's Heart Disease, Fuster and Hurst's The Heart
The Cardiac Conduction System

The normal beat originates in the sinoatrial (SA) node → spreads through both atria → reaches the AV node → travels down the His bundle → splits into right and left bundle branches → activates ventricles via Purkinje fibers.
Basic ECG Waveforms and Intervals
| Waveform | Represents | Normal Duration |
|---|---|---|
| P wave | Atrial depolarization | < 120 ms; amplitude < 2.5 mm |
| PR interval | AV conduction time | 120-200 ms |
| QRS complex | Ventricular depolarization | 60-100 ms (< 120 ms) |
| ST segment | Ventricular plateau phase | Isoelectric |
| T wave | Ventricular repolarization | Same polarity as QRS |
| QT interval | Total ventricular repolarization | QTc < 440 ms (men), < 460 ms (women) |
| U wave | Purkinje repolarization | Small, same polarity as T |
Normal 12-Lead ECG (sinus rhythm, HR 75 bpm, PR 160 ms, QRS 80 ms)
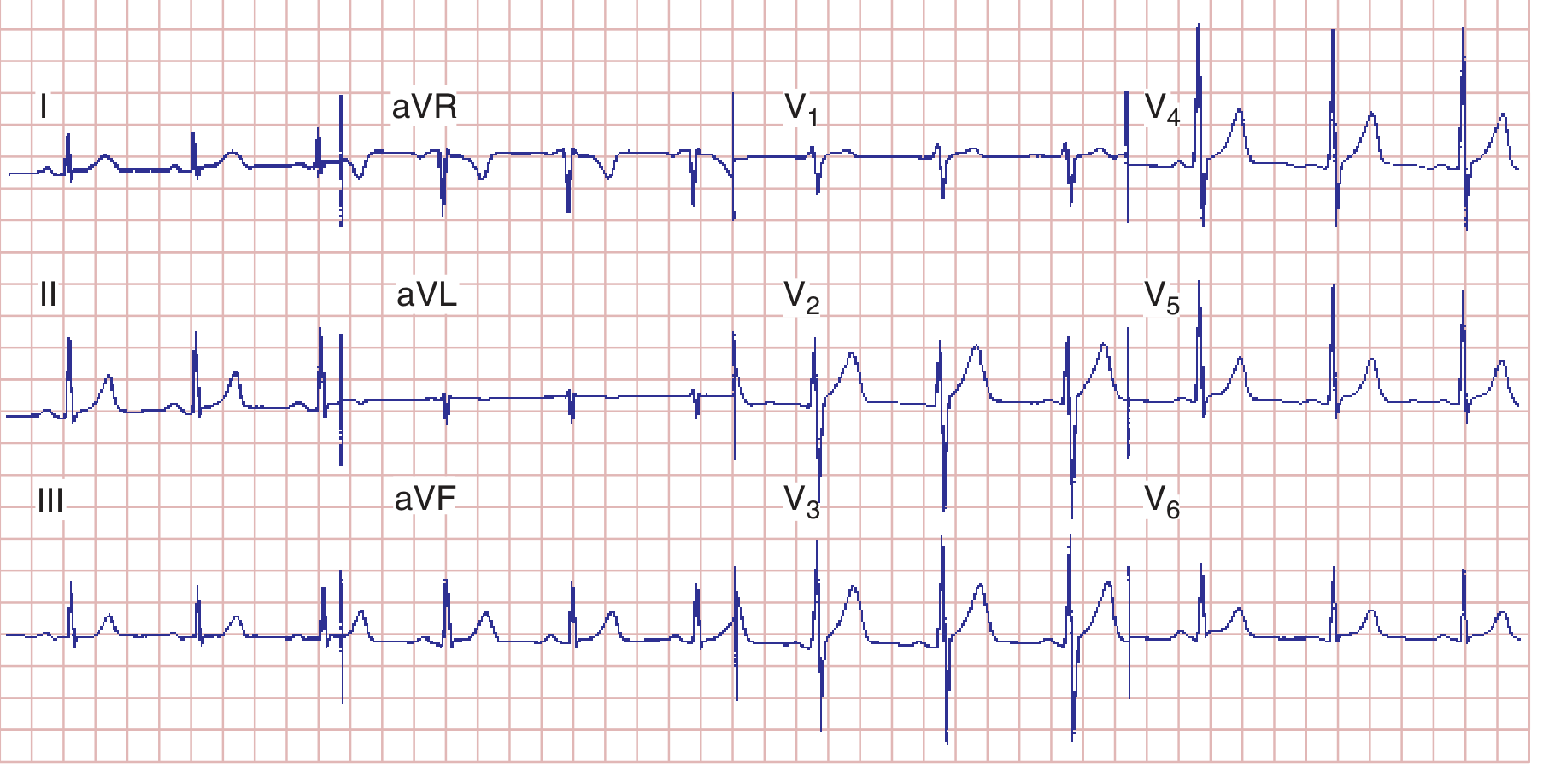
A systematic approach: (1) rate, (2) rhythm, (3) PR interval, (4) QRS duration, (5) QT/QTc, (6) axis, (7) P waves, (8) QRS voltages, (9) R-wave progression, (10) Q waves, (11) ST segments, (12) T waves, (13) U waves.
1. Sinus Rhythms
Normal Sinus Rhythm (NSR)
- Rate: 60-100 bpm
- Upright P wave before every QRS in leads I, II, aVF
- Regular P-P and R-R intervals
- PR interval 120-200 ms
Sinus Tachycardia
- Rate: > 100 bpm; identical to NSR otherwise
- Causes: fever, pain, anxiety, anemia, hypovolemia, PE, heart failure, drugs (atropine, sympathomimetics)
Sinus Bradycardia
- Rate: < 60 bpm; otherwise normal morphology
- Causes: athletes, vagal tone, inferior MI, hypothyroidism, beta-blockers, calcium channel blockers
Sinus Arrhythmia
- P-P interval varies with respiration (> 120 ms variation)
- Normal variant, especially in young people
2. Atrial Arrhythmias
Premature Atrial Complexes (PACs)
- Early, abnormally shaped P wave followed by narrow QRS
- May be non-conducted (blocked PAC) or conducted with aberrancy
Atrial Fibrillation (AF)
- No distinct P waves - replaced by irregular fibrillatory baseline (best seen in V1)
- Irregularly irregular ventricular rhythm
- Rate: ventricular rate 100-160 bpm (uncontrolled); variable QRS morphology possible if aberrant conduction
- Most common sustained arrhythmia; major risk factor for stroke
Atrial Flutter
- Sawtooth flutter waves at ~300 bpm (best in II, III, aVF)
- Regular ventricular rate, typically at 2:1, 3:1, or 4:1 block (150, 100, or 75 bpm)
- Flutter waves may be buried in QRS; carotid sinus massage unmasks them
Supraventricular Tachycardia (SVT / AVNRT)
- Narrow-complex tachycardia, regular, rate 150-250 bpm
- P waves hidden within or just after QRS (retrograde conduction)
- Abrupt onset and termination
Multifocal Atrial Tachycardia (MAT)
- Rate > 100 bpm
- At least 3 different P-wave morphologies
- Irregular rhythm
- Associated with COPD, severe illness
3. AV Block
First-Degree AV Block
- PR interval > 200 ms
- Every P wave conducts to ventricles
- Benign; may reflect increased vagal tone or digitalis effect
Second-Degree AV Block - Mobitz Type I (Wenckebach)
- Progressive PR prolongation until a P wave is not conducted (dropped QRS)
- Grouped beating; RR interval shortens before the drop
- Usually due to AV node disease; often benign
Second-Degree AV Block - Mobitz Type II
- Constant PR interval, then sudden non-conducted P wave (dropped QRS without warning)
- Indicates infranodal (His-Purkinje) disease
- Higher risk of progression to complete heart block; requires pacing consideration
Third-Degree (Complete) AV Block
- Complete dissociation of P waves and QRS complexes
- Atrial rate > ventricular rate
- Escape rhythm: junctional (narrow QRS, rate 40-60) or ventricular (wide QRS, rate 20-40)
- Causes: inferior MI, Lyme disease, digoxin toxicity, fibrosis of conduction system
4. Bundle Branch Blocks
Right Bundle Branch Block (RBBB)
- QRS ≥ 120 ms
- rSR' ("rabbit ears") in V1
- Wide, slurred S wave in I, aVL, V5-V6
- Secondary T-wave inversion in V1-V3 (normal with RBBB)
- Can be normal variant or seen with RVH, PE, ASD, ischemia
Left Bundle Branch Block (LBBB)
- QRS ≥ 120 ms
- Broad, notched R wave in I, aVL, V5-V6 (no septal q waves)
- QS or rS pattern in V1
- T-wave inversion in leads with broad R wave (discordant)
- Almost always pathological; associated with CAD, cardiomyopathy, hypertensive heart disease
- Makes ST analysis unreliable - new LBBB with symptoms = treat as STEMI equivalent
Left Anterior Fascicular Block (LAFB)
- QRS < 120 ms (fascicular blocks don't widen QRS significantly)
- Left axis deviation (more negative than -45°)
- Small q in I, aVL; small r in II, III, aVF
- Most common cause of marked LAD in adults
Left Posterior Fascicular Block (LPFB)
- Right axis deviation (> +110°)
- Small r in I; small q in III
- Rare; must exclude other causes of RAD (RVH, PE, lateral MI)
5. Ventricular Arrhythmias
Premature Ventricular Complexes (PVCs)
- Wide QRS (> 120 ms), bizarre morphology, no preceding P wave
- Full compensatory pause
- Isolated PVCs common and often benign; frequent PVCs (> 10,000/day) may cause cardiomyopathy
Ventricular Tachycardia (VT)
- Wide-complex tachycardia, rate 100-250 bpm, ≥ 3 consecutive beats
- AV dissociation (P waves marching through QRS) = diagnostic of VT
- Fusion beats and capture beats also diagnostic
- Sustained VT: lasts > 30 seconds or causes hemodynamic compromise
- Monomorphic vs. polymorphic (includes Torsades de Pointes)
Torsades de Pointes
- Polymorphic VT with twisting QRS axis around the baseline
- Associated with prolonged QT interval
- Triggers: hypokalemia, hypomagnesemia, class IA/III antiarrhythmics, tricyclics, certain antibiotics
Ventricular Fibrillation (VF)
- Chaotic, irregular waveforms, no organized QRS complexes
- Causes cardiac arrest; requires immediate defibrillation
6. Ventricular Hypertrophy

Left Ventricular Hypertrophy (LVH)
- Tall R waves in left leads (V5, V6, I, aVL) + deep S in V1-V2
- Sokolow-Lyon criterion: S(V1) + R(V5 or V6) > 35 mm
- Cornell criterion: R(aVL) + S(V3) > 28 mm (men) or > 20 mm (women)
- Associated ST depression and T-wave inversion in V5-V6 ("strain pattern")
- Causes: hypertension, aortic stenosis, hypertrophic cardiomyopathy
Right Ventricular Hypertrophy (RVH)
- Tall R wave in V1 (R > S in V1)
- Right axis deviation (QRS axis > +100°)
- ST depression and T-wave inversion in V1-V3 ("RV strain")
- Causes: pulmonary hypertension, severe pulmonic stenosis, congenital heart disease
Atrial Enlargement
Right atrial (RA) enlargement ("P pulmonale"):
- Tall, peaked P waves > 2.5 mm in II, III, aVF
Left atrial (LA) abnormality ("P mitrale"):
- Broad, notched P waves in limb leads (> 120 ms)
- Biphasic P wave in V1 with prominent negative terminal component
- Seen with mitral valve disease, LV dysfunction
7. Myocardial Ischemia and Infarction
Ischemia creates "currents of injury" that shift the ST segment. The location of changes identifies the affected territory.
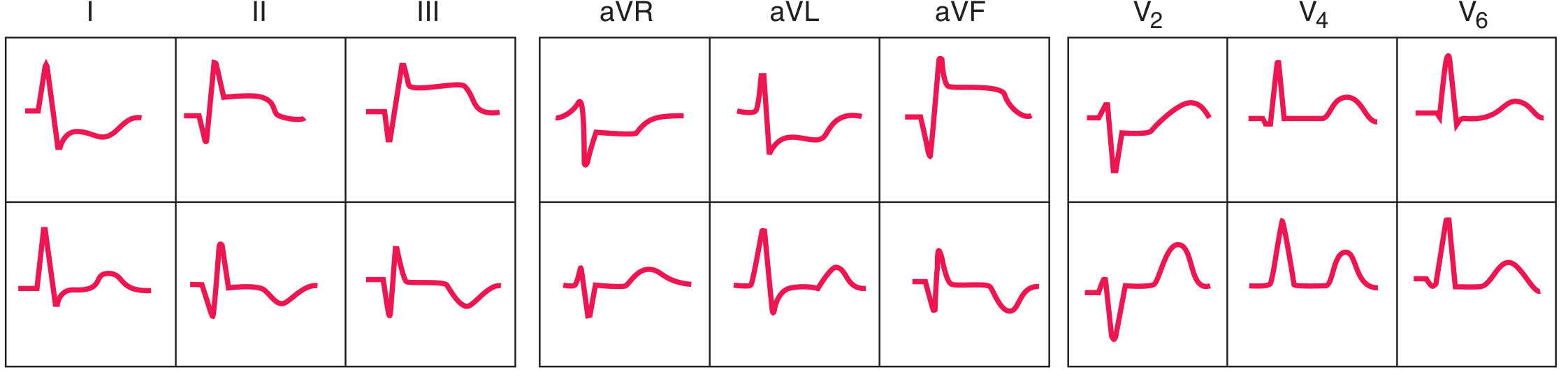
ST-Elevation MI (STEMI)
- ST elevation (≥ 1 mm in ≥ 2 contiguous limb leads; ≥ 2 mm in ≥ 2 contiguous precordial leads)
- Followed by T-wave inversion, then pathological Q waves (> 40 ms wide, > 25% of R-wave amplitude)
- Reciprocal ST depression in opposite leads
| Territory | Leads with ST elevation | Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Lateral | I, aVL, V5-V6 | LCx or LAD diagonal |
| Inferior | II, III, aVF | RCA (or LCx) |
| Posterior | Tall R in V1-V2, ST depression V1-V3 (reciprocal) | RCA/LCx |
| RV infarct | ST elevation in V4R | RCA proximal |
Anterior vs. Inferior STEMI ECG sequence
NSTEMI / Unstable Angina
- ST depression (horizontal or downsloping) ± T-wave inversion, without ST elevation
- No Q waves develop
- Subendocardial ischemia pattern
Wellens' Syndrome
- Characteristic T-wave changes in V2-V3 (deep symmetric inversions or biphasic) in a pain-free period
- Indicates critical LAD stenosis; high risk for massive anterior MI
8. Specific ECG Syndromes
Wolff-Parkinson-White (WPW)
- Short PR (< 120 ms)
- Delta wave (slurred upstroke of QRS)
- Wide QRS (> 120 ms)
- Pseudoinfarct Q waves possible
- Risk: pre-excited AF can cause VF if AV nodal blockers given
Brugada Syndrome
- Right bundle branch block morphology with ST elevation in V1-V3 (coved or saddle-back pattern)
- Structurally normal heart
- Risk of sudden cardiac death via VF
- Unmasked by sodium channel blockers, fever, cocaine
Long QT Syndrome (LQTS)
- QTc > 450-460 ms
- Congenital (LQTS1, LQTS2, LQTS3) or acquired
- Risk of Torsades de Pointes and sudden death
Short QT Syndrome
- QTc < 340 ms; tall, peaked T waves
- Risk of AF and VF
Hypertrophic Cardiomyopathy (HCM)
- LVH pattern with deeply inverted T waves in lateral leads
- Prominent septal Q waves in I, aVL, V5-V6
- "Dagger-like" Q waves
9. Metabolic and Drug-Induced Changes
Hyperkalemia ECG Progression
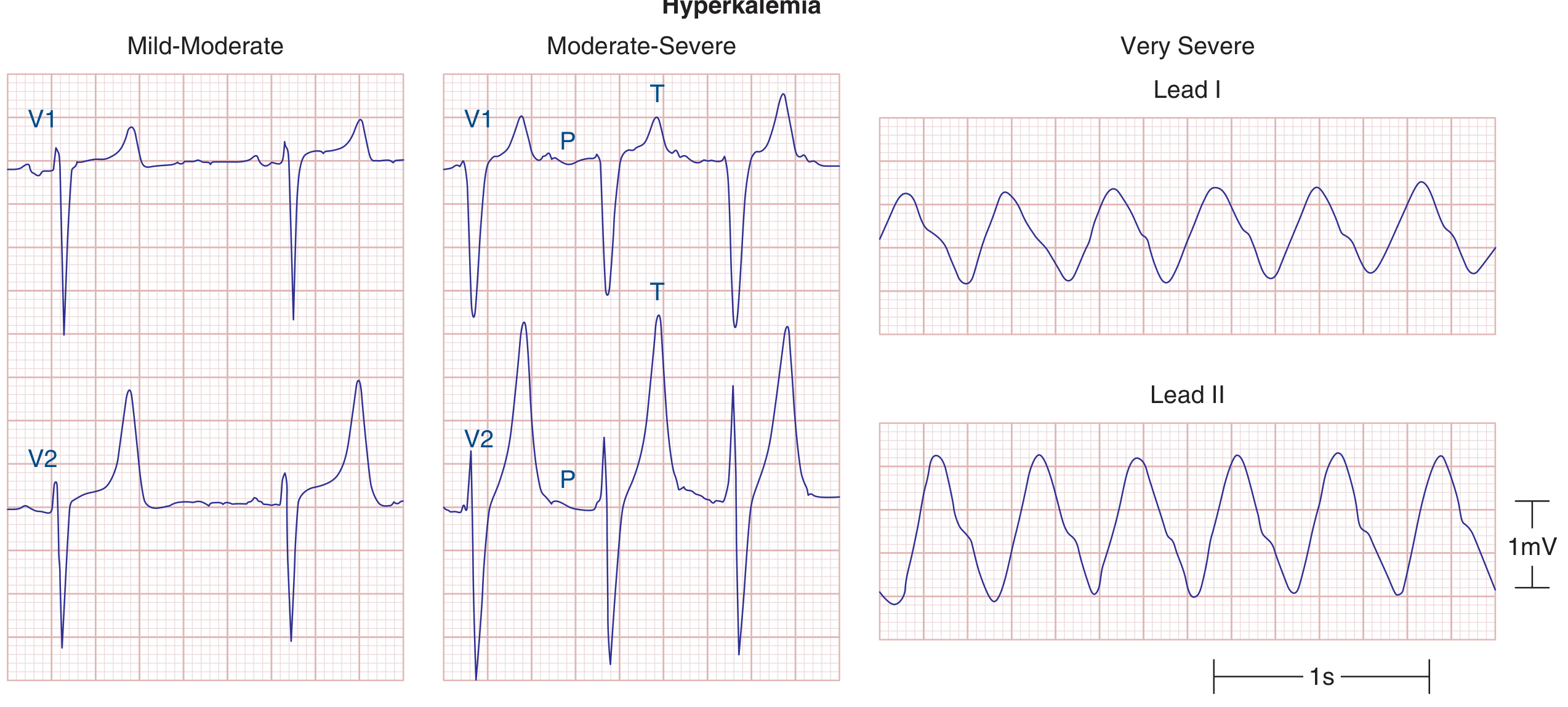
- Mild-moderate: Narrow, peaked ("tented") T waves
- Moderate-severe: PR prolongation, P-wave flattening, QRS widening
- Severe: Sine-wave pattern → asystole
Hypokalemia
- Prominent U waves (often taller than T waves)
- ST depression, T-wave flattening
- Prolonged QU interval (mimics long QT)
Hypocalcemia
- Prolonged QT interval (prolonged ST segment)
Hypercalcemia
- Shortened QT interval
Digitalis Effect
- "Scooped" ST-T complex (reverse tick appearance)
- Shortened QT interval
- Toxicity: PAT with block, junctional rhythms, VT, AV block
Hypothermia
- Osborn (J) wave: positive deflection at J point, best in V4-V6
- Bradycardia; prolonged all intervals
Pericarditis (Acute)
- Diffuse, concave ST elevation in multiple leads (saddle-shaped)
- PR depression (best seen in II, aVF)
- Unlike MI: no reciprocal ST changes (except aVR), no Q waves
- Evolves through 4 stages (ST elevation → normalization → T inversion → resolution)
Pulmonary Embolism (Acute)
- Most common: sinus tachycardia
- Classic (uncommon): S1Q3T3 - S wave in I, Q wave and T inversion in III
- Right axis deviation, new RBBB, T inversion V1-V4
10. Quick Reference Summary Table
| Pattern | Key ECG Finding | Clinical Significance |
|---|---|---|
| NSR | Regular P-QRS, rate 60-100 | Normal |
| Sinus tachycardia | Rate > 100, normal P waves | Physiologic/pathologic cause |
| AF | No P waves, irregular QRS | Stroke risk, rate control |
| Atrial flutter | Sawtooth at 300, 2:1 block | Cardioversion or rate control |
| 1st-degree AVB | PR > 200 ms | Usually benign |
| Wenckebach | Progressive PR then dropped beat | Usually benign |
| Mobitz II | Constant PR then dropped beat | Risk of complete block |
| Complete heart block | P-QRS dissociation | Pacing required |
| RBBB | rSR' in V1, wide S in V6 | May be normal variant |
| LBBB | Broad R in V6, QS in V1 | Usually pathological |
| LVH | Sokolow > 35 mm + strain | Hypertension, AS, HCM |
| STEMI anterior | ST↑ V1-V4 | LAD occlusion, emergent PCI |
| STEMI inferior | ST↑ II, III, aVF | RCA occlusion |
| WPW | Short PR + delta wave | Risk of pre-excited AF |
| Brugada | Coved ST↑ V1-V3, RBBB-like | SCD risk |
| Hyperkalemia | Peaked T → sine wave | Emergent treatment |
| Long QT | QTc > 450 ms | Torsades risk |
| Pericarditis | Diffuse concave ST↑, PR↓ | NSAIDs, colchicine |
| PE | S1Q3T3, sinus tach | Anticoagulation |
| Digitalis effect | Scooped ST-T | Drug effect vs. toxicity |
Sources: Harrison's Principles of Internal Medicine 22E (2025) - Ch. 247 (Goldberger); Braunwald's Heart Disease 12E; Fuster and Hurst's The Heart 15E
This is a shared conversation. Sign in to Orris to start your own chat.