Meaning of GVA GSA GSE GVE SSA SVA SVE
Searching the Web
GVA GSA GSE GVE SSA SVA SVE abbreviations meaning
These are cranial nerve fiber classifications used in neuroanatomy. They describe the functional components of cranial nerve fibers using two dimensions:
- G = General | S = Special
- V = Visceral | S = Somatic
- A = Afferent (sensory, toward brain) | E = Efferent (motor, away from brain)
The 7 Functional Components
| Code | Full Name | Meaning |
|---|---|---|
| GSA | General Somatic Afferent | Sensory from skin, muscles, joints (touch, pain, temp, proprioception) — general body sense |
| GSE | General Somatic Efferent | Motor to skeletal muscles derived from somites (tongue muscles, extraocular muscles) |
| GVA | General Visceral Afferent | Sensory from internal organs, glands, blood vessels (visceral pain, stretch, chemical signals) |
| GVE | General Visceral Efferent | Autonomic (parasympathetic) motor to smooth muscle, cardiac muscle, glands |
| SSA | Special Somatic Afferent | Special senses from somatic structures: vision (CN II) and hearing/balance (CN VIII) |
| SVA | Special Visceral Afferent | Special senses from visceral structures: taste (CN VII, IX, X) and smell (CN I) |
| SVE | Special Visceral Efferent | Motor to muscles derived from pharyngeal (branchial) arches — jaw, facial, pharyngeal, laryngeal muscles |
Quick Memory Aid
- "Somatic" = body wall / skeletal; "Visceral" = organs / gut
- "General" = widespread distribution; "Special" = specific specialized organs
- "Afferent" = incoming (sensory); "Efferent" = outgoing (motor)
Which Cranial Nerves Carry Which Fibers
| Fiber Type | Cranial Nerves |
|---|---|
| GSA | V, VII, IX, X |
| GSE | III, IV, VI, XII |
| GVA | IX, X |
| GVE | III, VII, IX, X |
| SSA | II, VIII |
| SVA | I, VII, IX, X |
| SVE | V, VII, IX, X, XI |
Vertical and horizontal gaze palsy
Reading File
Finding Sources
Searching the Web
vertical horizontal gaze palsy neuroanatomy lesion site mechanism
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
horizontal gaze palsy PPRF pontine lesion diagram
Here is a comprehensive overview of gaze palsies:
Gaze Palsies: Horizontal & Vertical
A gaze palsy is an impairment of conjugate (both eyes moving together symmetrically) excursions, limited to either the horizontal or vertical plane. The key distinction from individual nerve palsies is that both eyes are equally affected.
Anatomy of Gaze Control
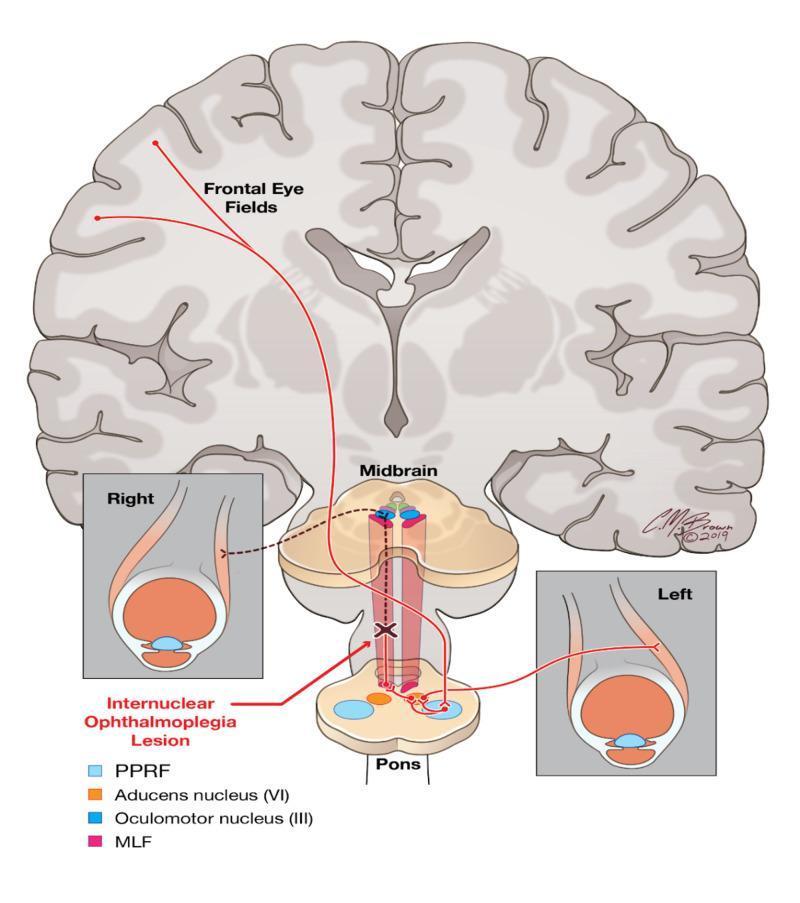
Horizontal Gaze
The Paramedian Pontine Reticular Formation (PPRF) — also called the horizontal gaze centre — is located in the pons. When activated:
- Signals travel directly to the ipsilateral CN VI nucleus → lateral rectus of the same side
- Internuclear neurons cross the midline and ascend via the contralateral Medial Longitudinal Fasciculus (MLF) → CN III nucleus → medial rectus of the opposite eye
- Result: conjugate gaze toward the same side as the stimulated PPRF
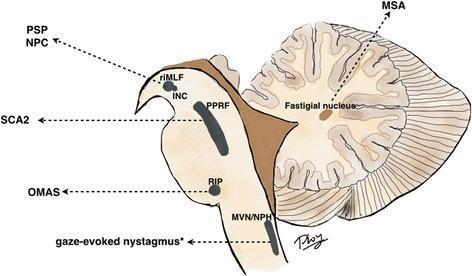
Vertical Gaze
- Controlled by the rostral interstitial nucleus of the MLF (riMLF) in the midbrain
- Upgaze fibers decussate through the posterior commissure (near the pretectum)
- Downgaze fibers project directly (no decussation) to oculomotor nuclei
- The Interstitial Nucleus of Cajal (INC) serves as the neural integrator for vertical gaze holding
Horizontal Gaze Palsy
Mechanism & Lesion Sites
| Site | Effect | Key Feature |
|---|---|---|
| PPRF (pons) | Ipsilateral gaze palsy — cannot look toward lesion side | NOT overcome by doll's-head maneuver or calorics |
| CN VI nucleus (pons) | Ipsilateral gaze palsy + ipsilateral esotropia | Slow saccades in contralateral hemifield |
| Frontal Eye Field (FEF) cortex | Contralateral gaze palsy — eyes deviate toward lesion acutely | Overcome by doll's-head / calorics (supranuclear) |
Rule: Frontal lobe lesion → eyes look toward the lesion (away from the hemiplegia). Pontine lesion → eyes look away from the lesion (toward the hemiplegia).
Clinical pearl
In the most severe pontine form, neither eye can cross the midline into the opposite field. Milder forms show slow saccades or gaze-evoked nystagmus contralaterally.
Vertical Gaze Palsy
Mechanism & Lesion Sites
| Site | Effect |
|---|---|
| Pretectum / posterior commissure (midbrain) | Upgaze palsy (most common) — upgaze fibers cross here and are vulnerable |
| riMLF bilateral | Both upgaze and downgaze deficits |
| riMLF unilateral | Slowing of downward saccades; torsional nystagmus |
| Thalamus | Supranuclear vertical gaze palsies (upgaze) |
Why upgaze > downgaze palsy?
Upgaze fibers decussate in the dorsal midbrain near the posterior commissure → vulnerable to compression/infarction there. Downgaze fibers project directly from riMLF without crossing → spared with dorsal midbrain lesions.
Parinaud (Dorsal Midbrain) Syndrome
Classic upgaze palsy caused by compression of the dorsal midbrain (pretectal region):
| Sign | Details |
|---|---|
| Supranuclear upgaze palsy | Saccades impaired; VOR (doll's-head) preserved |
| Convergence-retraction nystagmus | On attempted upgaze |
| Light-near dissociation | Pupils react to accommodation but not light |
| Collier sign | Bilateral lid retraction |
| Defective convergence |
Causes by age:
- Children: pinealoma/pinealoblastoma, aqueduct stenosis, meningitis
- Young adults: demyelination, AVM, trauma
- Elderly: midbrain infarct, mass lesions, posterior fossa aneurysm
Progressive Supranuclear Palsy (PSP / Steele-Richardson-Olszewski)
A neurodegenerative disease that specifically impairs downward gaze first, then upgaze, then horizontal — eventually global gaze palsy. Associated with pseudobulbar palsy, extrapyramidal rigidity, and dementia.
- Key differentiator from Parkinson's disease: downgaze palsy does NOT occur in PD; its presence strongly suggests PSP.
Related Syndromes
| Syndrome | Lesion | Deficit |
|---|---|---|
| INO (internuclear ophthalmoplegia) | MLF | Ipsilateral adduction failure + contralateral abduction nystagmus |
| One-and-a-half syndrome | PPRF + ipsilateral MLF | Ipsilateral gaze palsy + INO → only movement: contralateral abduction |
| WEBINO | Bilateral rostral MLF | Bilateral INO + exotropia ("wall-eyed") |
Diseases Causing Vertical/Upgaze Palsy (Summary)
- Midbrain infarction/hemorrhage
- Pinealoma or dorsal midbrain tumor
- Hydrocephalus (3rd ventricle enlargement)
- Progressive supranuclear palsy
- Parkinson's disease, Lewy body disease
- Niemann-Pick type C, Gaucher disease, Tay-Sachs (metabolic)
- Whipple disease of the brain
- Bilateral INO (e.g., multiple sclerosis)
(Adams & Victor's Principles of Neurology, 12th Ed.; Kanski's Clinical Ophthalmology, 10th Ed.; Localization in Clinical Neurology, 8th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.