Explain me 10 heart diseases common ecg change and ecg images
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common heart diseases ECG changes findings 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Searching the Web
ECG Wolff-Parkinson-White Brugada syndrome hyperkalemia complete heart block Torsades de pointes patterns
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive textbook content and key ECG images. Let me compose the full, detailed answer.
10 Common Heart Diseases and Their ECG Changes
Sources: Harrison's Principles of Internal Medicine 22E (2025), Rosen's Emergency Medicine, Tintinalli's Emergency Medicine
1. ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of an epicardial coronary artery causes transmural ischemia. Current of injury flows outward toward epicardial leads, producing ST elevation.
ECG Changes:
- Hyperacute T waves - the earliest sign: broad, tall T waves preceding ST changes
- ST elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Pathological Q waves - develop within hours to days (>40 ms wide, >25% of R wave height)
- T wave inversions - evolve as ST normalizes
- Reciprocal ST depression in opposite leads (increases specificity)
Localization:
- Anterior STEMI: V1-V4 (LAD)
- Inferior STEMI: II, III, aVF (RCA)
- Lateral STEMI: I, aVL, V5-V6
- Posterior MI: tall R wave + horizontal ST depression in V1-V2 (mirror image)
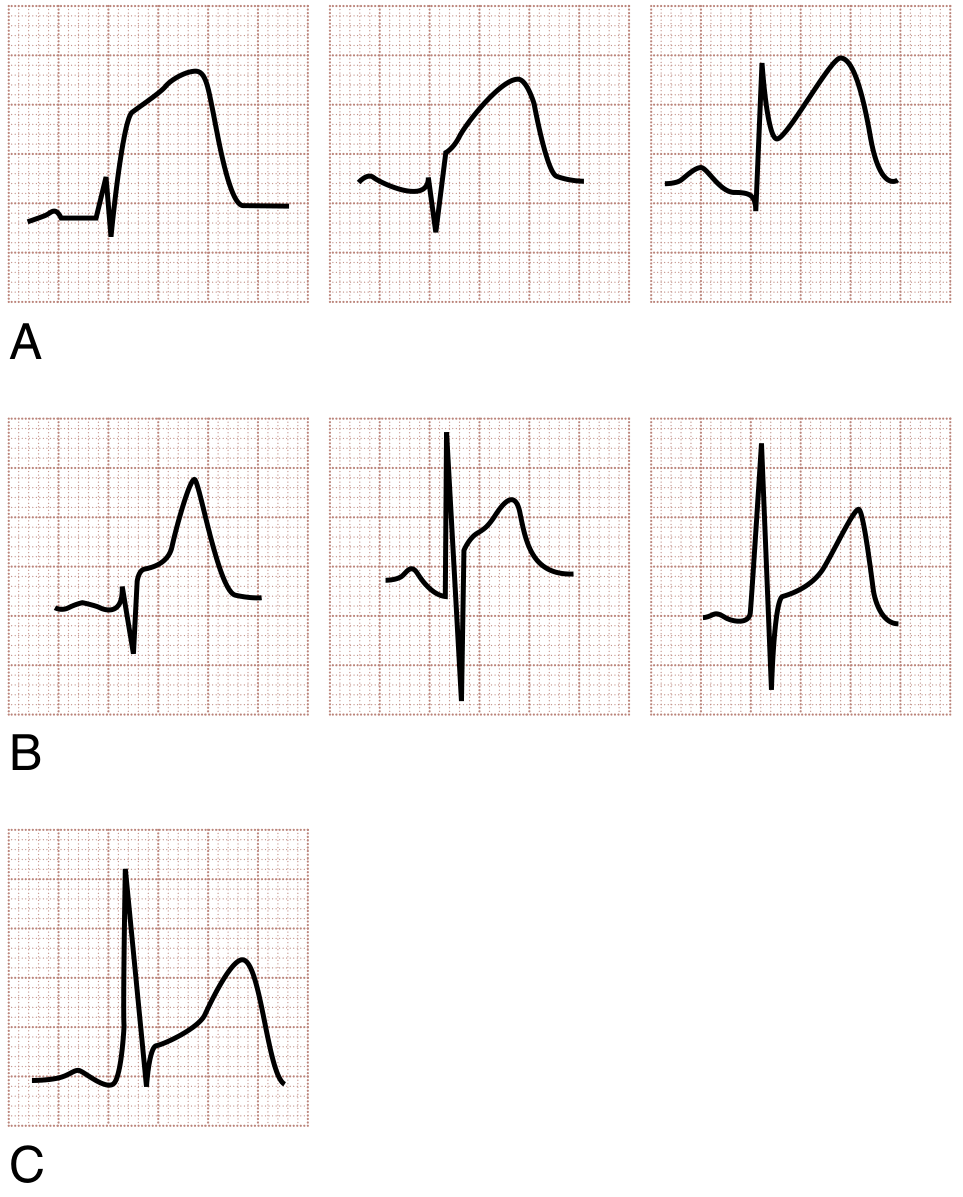
Fig 1. ST segment morphology comparison: (A) Flat/convex ST in STEMI; (B) Concave ST in benign early repolarization and pericarditis; (C) Concave pattern also seen in some STEMIs - serial ECGs help distinguish. (Rosen's Emergency Medicine)
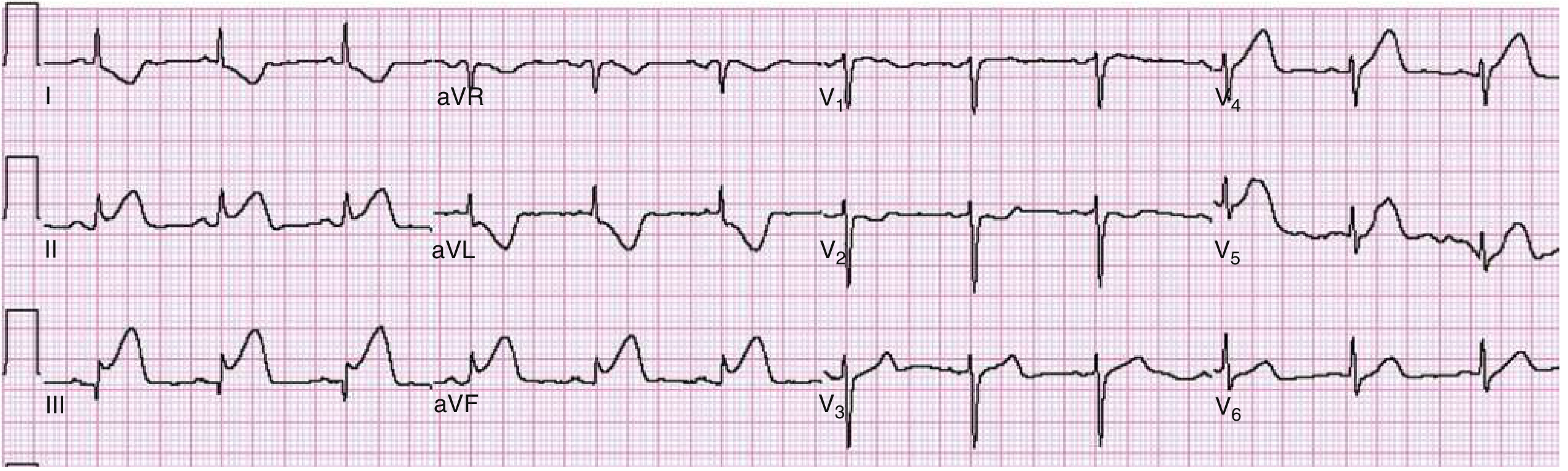
Fig 2. Inferior STEMI: Marked ST elevation in leads II, III, aVF; classic reciprocal ST depression in I and aVL. (Rosen's Emergency Medicine)
2. Non-ST Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Mechanism: Subendocardial ischemia. The ST vector shifts toward the subendocardium/ventricular cavity, causing overlying leads to show ST depression.
ECG Changes:
- ST depression (horizontal or downsloping) - most typical; upsloping is less specific
- T wave inversions - narrow, symmetrical; isoelectric or slightly upward-bowed ST preceding them
- Wellens syndrome - deep symmetrical T wave inversions (Type I) or biphasic T waves (Type II) in V1-V4, indicating critical LAD stenosis; may be present even when pain-free
- May have a normal ECG - does NOT exclude NSTEMI
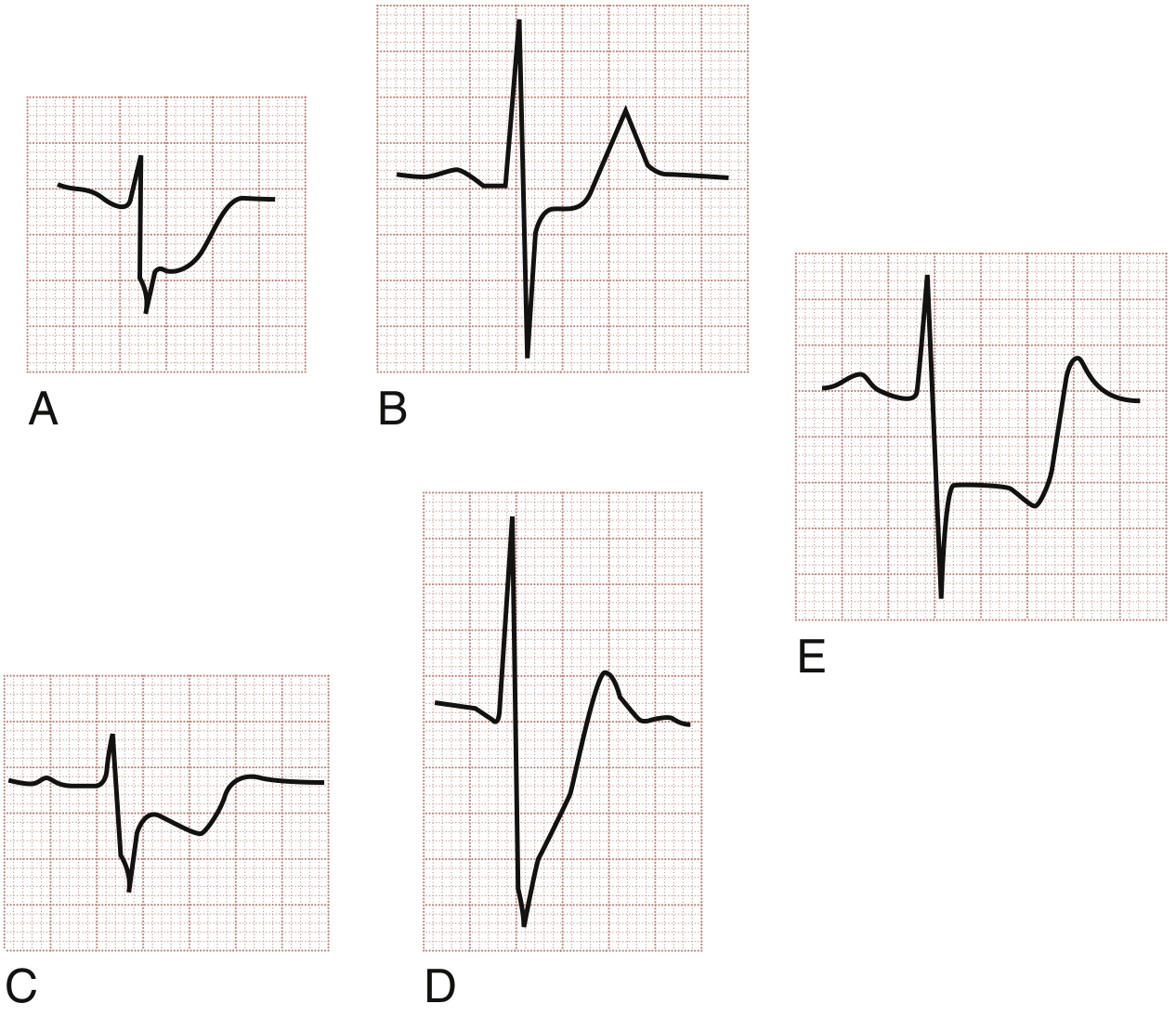
Fig 3. ST segment depression in ACS: (A) flat/horizontal pattern, (B) upsloping (less ischemic), (C) horizontal in posterior MI (right precordials), (D) marked downsloping, (E) biphasic Wellens T waves. (Rosen's Emergency Medicine)

Fig 4. Wellens T wave sign - deep symmetric T wave inversions in precordial leads V1-V6 with severe LAD stenosis. (Harrison's Principles of Internal Medicine 22E)
3. Atrial Fibrillation (AF)
Mechanism: Chaotic, disorganized atrial electrical activity from multiple micro-reentrant circuits. Associated with ischemic heart disease, valvular disease, cardiomyopathy, thyrotoxicosis, and "holiday heart" (alcohol binge).
ECG Changes (from Tintinalli's Table 18-8):
- Absent P waves - replaced by a chaotic, fibrillatory baseline (f waves, 350-600/min)
- Irregularly irregular RR intervals - the hallmark
- Narrow QRS unless pre-existing bundle branch block or pre-excitation (WPW)
- Ventricular rate typically 100-160/min if uncontrolled
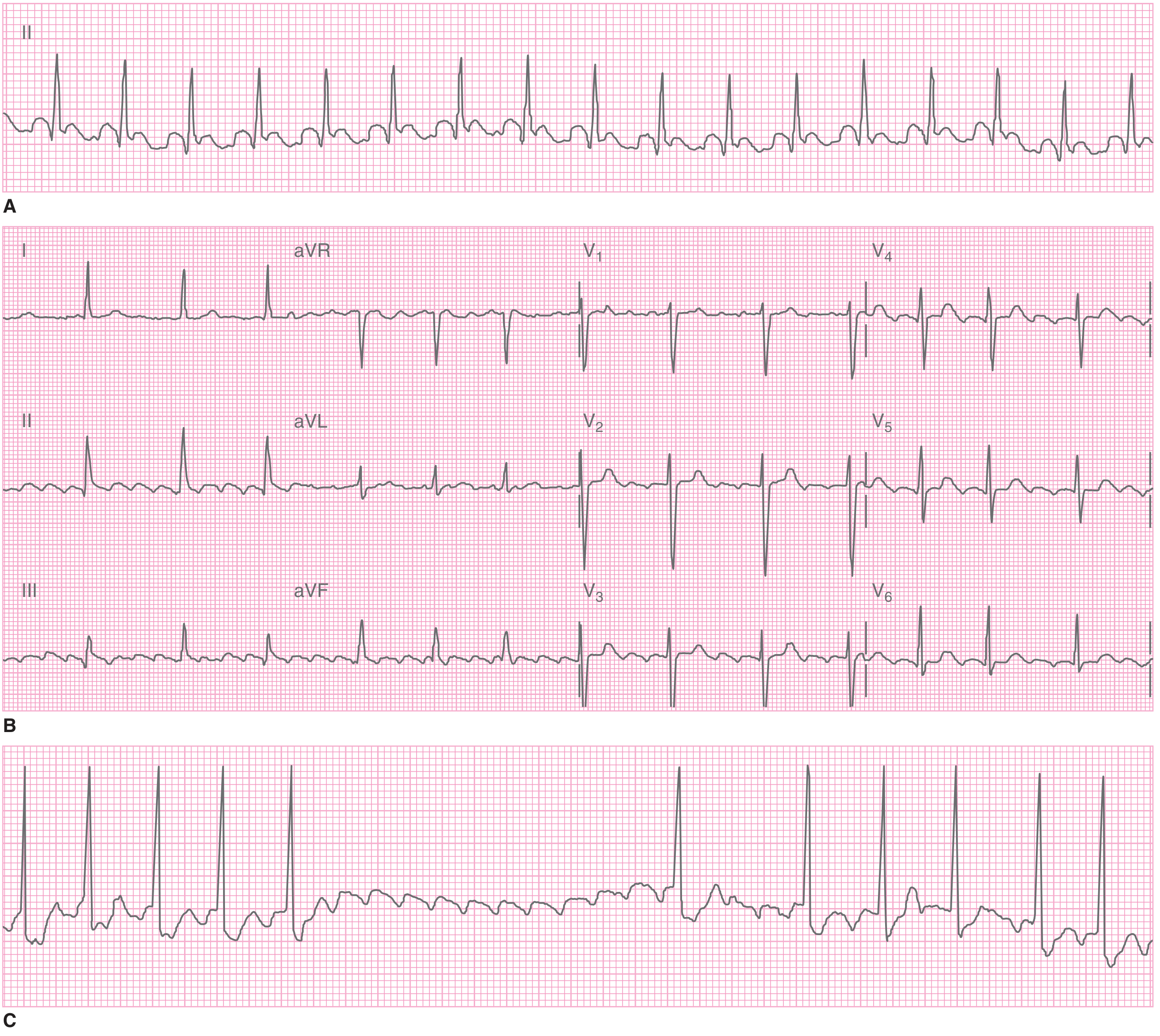
Fig 5. (A) Tachycardia with irregular baseline - atrial fibrillation; (B) Regular narrow-complex tachycardia with flutter waves (sawtooth) in leads II, III, aVF - atrial flutter with 2:1 block; (C) Atrial flutter response to carotid sinus massage unmasking flutter waves. (Tintinalli's Emergency Medicine)
4. Complete Heart Block (Third-Degree AV Block)
Mechanism: Complete dissociation between atrial and ventricular conduction. No impulses pass through the AV node. The ventricles are driven by a slow escape rhythm (junctional or ventricular).
ECG Changes:
- P waves present but bear no fixed relationship to QRS complexes (AV dissociation)
- PP intervals regular, RR intervals regular, but PR intervals vary completely
- Bradycardia - escape rate 20-40/min if ventricular, 40-60/min if junctional
- Wide QRS (>120 ms) if ventricular escape; narrow QRS if junctional escape
- Ventricular rate is slower than atrial rate
5. Left/Right Bundle Branch Block (LBBB / RBBB)
Mechanism: Impaired conduction in one bundle system prolongs QRS and shifts its vector toward the side of delayed depolarization.
ECG Changes:
| Feature | RBBB | LBBB |
|---|---|---|
| QRS duration | ≥120 ms | ≥120 ms |
| V1 morphology | rSR' ("rabbit ears") | QS or rS (negative) |
| V6 morphology | qRS with terminal S | Broad monophasic R, no Q |
| T wave | Opposite to last QRS deflection | Opposite to last QRS deflection |
| Axis | Right or normal | Left |
- LBBB is a marker of underlying CAD, hypertensive heart disease, aortic valve disease, or cardiomyopathy - and can mask STEMI
- RBBB can be normal or associated with atrial septal defect, pulmonary hypertension
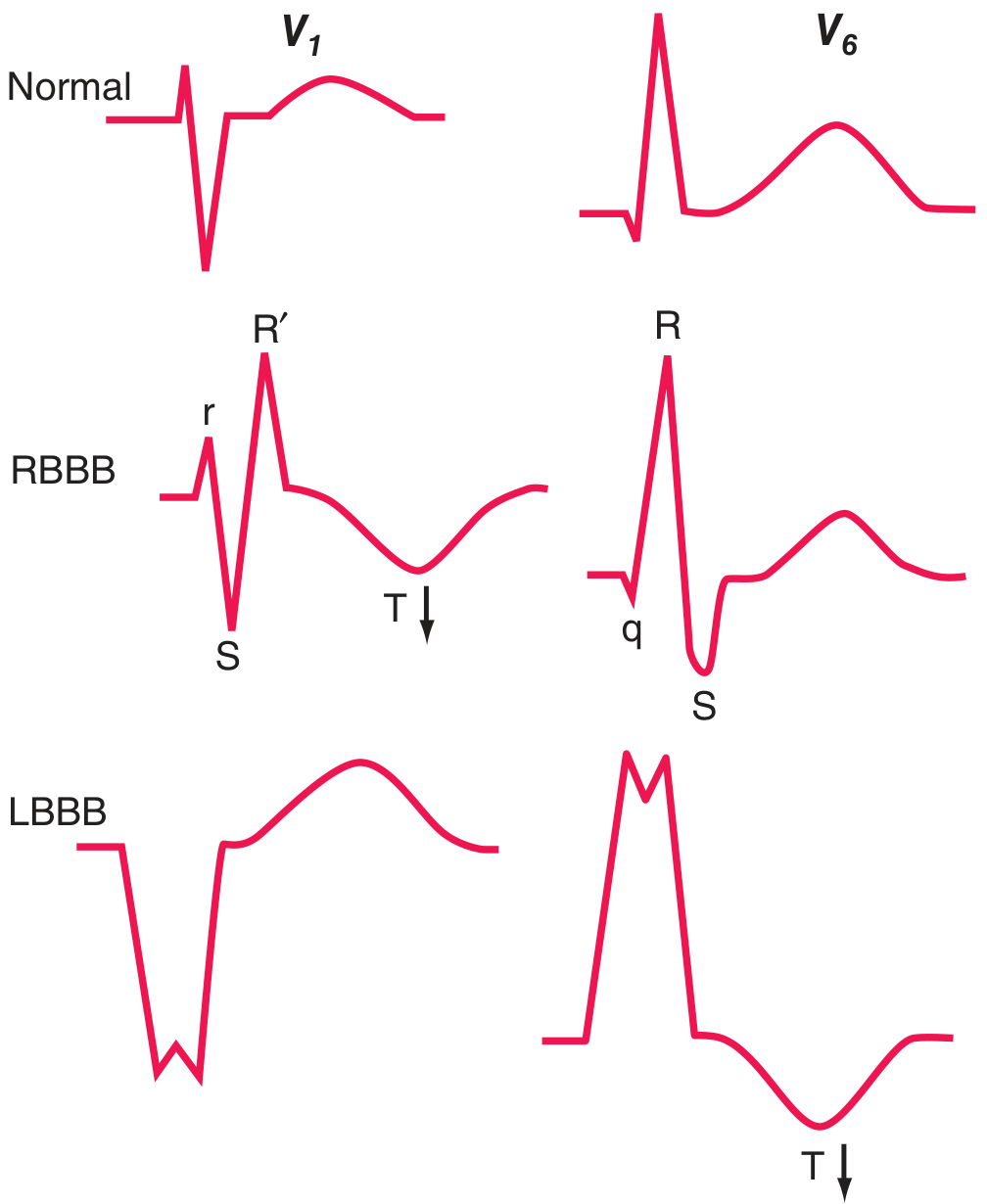
Fig 6. RBBB vs LBBB comparison. RBBB: rSR' in V1, qRS in V6, T wave inverted (arrow). LBBB: QS in V1, broad R in V6, T inverted (arrow). (Harrison's Principles of Internal Medicine 22E)
6. Left Ventricular Hypertrophy (LVH)
Mechanism: Increased muscle mass from pressure overload (hypertension, aortic stenosis) generates larger electrical potentials directed leftward and posteriorly.
ECG Changes (Sokolow-Lyon criteria and others):
- Increased voltage: SV1 + RV5 or RV6 ≥35 mm; RaVL >20 mm (women) or >28 mm (men)
- Left axis deviation
- ST depression + T wave inversion in leads I, aVL, V5-V6 ("strain pattern") - a secondary repolarization change
- Left atrial abnormality (P mitrale) - broad, notched P waves in lead II; biphasic P in V1
- May progress to LBBB
Note: Voltage criteria have low sensitivity, especially in obese patients and smokers.
7. Acute Pericarditis
Mechanism: Diffuse pericardial inflammation affects the subepicardial myocardium, causing widespread repolarization changes. There is also PR depression from atrial involvement.
ECG Changes (4 evolutionary stages):
- Stage 1 (acute): Diffuse ST elevation (concave/saddle-shaped) in almost all leads EXCEPT aVR and V1; PR segment depression (most specific finding)
- Stage 2: ST returns to baseline; T waves flatten
- Stage 3: T wave inversions develop diffusely
- Stage 4: Normalization
Key distinguishing features from STEMI:
- ST elevation is concave (not convex), diffuse (not regional)
- PR depression present
- No reciprocal ST depression (except aVR)
- No Q waves
- ST:T ratio in V6 >0.25 favors pericarditis
(Differential included in Table 64.3 from Rosen's - see Fig 1 above for ST morphology comparison)
8. Pulmonary Embolism (PE)
Mechanism: Acute right heart pressure overload from massive PE causes right ventricular dilation and strain, shifting the electrical axis rightward.
ECG Changes:
- Sinus tachycardia - the most common finding
- S1Q3T3 pattern - prominent S wave in lead I, Q wave in lead III, T wave inversion in lead III
- Right axis deviation
- New RBBB or incomplete RBBB (right ventricular conduction delay)
- ST-T changes in V1-V4 simulating anterior infarction (right ventricular strain)
- Right precordial T wave inversions (V1-V3)
- Atrial fibrillation or flutter may occur
- A normal ECG does NOT rule out PE
9. Wolff-Parkinson-White Syndrome (WPW)
Mechanism: An accessory bypass tract (Bundle of Kent) pre-excites the ventricles, bypassing the AV node delay. Ventricular activation begins earlier via the accessory pathway and the rest continues via the normal conduction system.
ECG Changes (the "WPW triad"):
- Short PR interval (<120 ms) - early ventricular activation bypassing AV node
- Delta wave - slurred upstroke at the beginning of the QRS (slow accessory pathway conduction through ventricular myocardium)
- Wide QRS (≥120 ms) - due to delta wave + fusion beat
- Secondary ST-T changes - discordant from QRS
- Risk of rapid conduction of AF down the bypass tract causing ventricular fibrillation
From Harrison's: "Prolongation of QRS duration...may be due to pre-excitation of the ventricles via a bypass tract, as in Wolff-Parkinson-White (WPW) patterns"
10. Brugada Syndrome
Mechanism: Autosomal dominant sodium channel mutation (SCN5A) causes abnormal early repolarization of right ventricular outflow tract. Associated with risk of sudden cardiac death from ventricular fibrillation.
ECG Changes:
- Type 1 (diagnostic - "coved" type): ST elevation ≥2 mm with coved (convex dome) morphology in V1-V2 (or V1-V3 in 2nd/3rd intercostal space), followed by a negative T wave - this is the ONLY diagnostic pattern
- Type 2 ("saddle-back"): ST elevation with saddle-back morphology - not diagnostic alone
- Pattern may be intermittent and provoked by fever, sodium channel blockers, or vagal tone
- Normal intervals otherwise; structurally normal heart
- Simulates RBBB morphology in right precordial leads
Harrison's: "A distinctive abnormality simulating right bundle branch block with ST-segment elevations in the right chest leads is seen with the Brugada pattern"
Summary Table
| # | Disease | Key ECG Finding | Leads Affected |
|---|---|---|---|
| 1 | STEMI | Convex ST elevation + Q waves + hyperacute T | Regional (I, V1-V4, II/III/aVF) |
| 2 | NSTEMI/UA | Horizontal/downsloping ST depression; Wellens T | V1-V4, diffuse |
| 3 | Atrial Fibrillation | Absent P waves; irregularly irregular RR | All leads |
| 4 | Complete Heart Block | AV dissociation; bradycardia; varying PR | All leads |
| 5 | LBBB / RBBB | Wide QRS ≥120 ms; rSR' (RBBB) vs QS (LBBB) | V1, V6 |
| 6 | LVH | Tall voltage; strain pattern (ST depression, T inversion) | Left precordial leads |
| 7 | Acute Pericarditis | Diffuse concave ST elevation; PR depression | Widespread (except aVR) |
| 8 | Pulmonary Embolism | S1Q3T3; new RBBB; sinus tachycardia | I, III, V1-V4 |
| 9 | WPW Syndrome | Short PR; delta wave; wide QRS | All leads |
| 10 | Brugada Syndrome | Coved ST elevation V1-V2; RBBB-like morphology | V1-V3 |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill) - Chap. 247
- Rosen's Emergency Medicine - Chap. 64
- Tintinalli's Emergency Medicine: A Comprehensive Study - Chap. 18
This is a shared conversation. Sign in to Orris to start your own chat.