Crohn’s disease
Reading File
Finding Sources
Searching PubMed
"Crohn's disease"[MeSH Terms] AND management
Searching the Web
Crohn's disease 2025 2026 updated guidelines treatment
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"Crohn disease"[MeSH Terms] AND "biological therapy"[MeSH Terms]
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have enough content for a comprehensive answer. Let me compile it.
Crohn's Disease
Definition and Overview
Crohn's disease (CD) is a chronic, relapsing inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal tract from mouth to anus. It is characterized by transmural (full-thickness), discontinuous ("skip lesion") inflammation. The terminal ileum is the most commonly affected site. Unlike ulcerative colitis (UC), which is confined to the colon and has continuous, more superficial involvement, CD may produce strictures and fistulas as a consequence of its deep, transmural nature.
Epidemiology
- Bimodal age of onset: peak in young adults (15-25 years) with a second smaller peak in the 50s-60s
- Affects approximately 1 million people in the United States
- Incidence is rising globally, particularly in industrializing countries and those adopting Westernized diets
- Previously concentrated in Western Europe and North America; now increasingly seen in Asia and Latin America
Etiology and Pathogenesis
CD results from a combination of:
- Genetic susceptibility - Hundreds of loci are associated with IBD. Key genes include NOD2 (innate immunity), IL-23R (interleukin receptor), and ATG16L1 (autophagy). No single gene variant is diagnostically useful on its own.
- Dysregulated immune response - Abnormal immune activation in response to luminal antigens or gut microbiota
- Microbiome dysbiosis - Altered gut bacterial composition
- Environmental factors - Westernized diet, air pollution, industrialization, smoking (smoking increases risk of CD, in contrast to UC where it is protective)
Pathology
Gross Features
- Transmural inflammation - penetrates the full thickness of the bowel wall
- Skip lesions - diseased segments alternating with normal mucosa (distinguishes CD from UC)
- Cobblestone appearance - mucosal islands separated by deep linear fissuring ulcers
- Strictures - from fibrotic healing of transmural inflammation
- Fistulas - abnormal tracts between bowel loops, bladder, skin, or vagina due to fistulizing penetration
- Mesenteric fat wrapping ("creeping fat") - fat extends over the serosal surface of the bowel
Microscopic Features
- Transmural chronic inflammation
- Non-caseating granulomas - present in ~50% of cases; highly specific when found
- Crypt architectural distortion
- Submucosal fibrosis
- In the stomach: focally enhanced gastritis; serpiginous or longitudinal ulcers
Distribution and Classification
| Location | Approximate Frequency |
|---|---|
| Ileocolitis (terminal ileum + colon) | ~40-50% (most common) |
| Ileum only | ~30% |
| Colon only | ~20% |
| Upper GI (stomach/duodenum) | ~5% (almost always with lower GI involvement) |
The Montreal Classification describes CD by:
- Location: L1 (ileal), L2 (colonic), L3 (ileocolonic), L4 (upper GI modifier)
- Behavior: B1 (inflammatory), B2 (stricturing), B3 (penetrating)
- Perianal modifier: "p" added if perianal disease is present
Clinical Features
Intestinal Symptoms
- Chronic or intermittent abdominal pain (often right lower quadrant)
- Non-bloody diarrhea (blood may occur if colonic involvement)
- Weight loss and malnutrition
- Fever during flares
- Perianal disease: skin tags, fissures, abscesses, fistulas (highly characteristic of CD)
Complications
- Obstruction - from fibrotic strictures (chronic) or active inflammation (acute)
- Abscesses - intra-abdominal or perianal
- Fistulas - enteroenteric, enterovesical, enterocutaneous, rectovaginal
- Malabsorption - from reduced absorptive surface area, terminal ileal disease (B12 deficiency, bile salt malabsorption), small intestinal bacterial overgrowth (SIBO)
- Short bowel syndrome - after repeated resections
- Colorectal cancer - increased risk with longstanding colonic involvement
Extraintestinal Manifestations (EIMs)
- Joints: peripheral arthritis, ankylosing spondylitis, sacroiliitis
- Skin: erythema nodosum, pyoderma gangrenosum
- Eyes: episcleritis, uveitis
- Liver/biliary: primary sclerosing cholangitis (more common in UC but occurs in CD)
- Other: aphthous mouth ulcers, thromboembolic disease
Diagnosis
Laboratory
- Elevated CRP and ESR - correlate with disease activity; high CRP suggests active disease or infectious complication
- Fecal calprotectin and lactoferrin - sensitive markers of intestinal inflammation; useful for monitoring relapse and response to biologics
- Anemia (iron deficiency, B12 deficiency, anemia of chronic disease)
- Hypoalbuminemia
Endoscopy
- Colonoscopy with ileoscopy: aphthous ulcers, deep linear/serpiginous ulcers, cobblestoning, skip lesions
- Mucosal biopsies showing granulomas are highly supportive
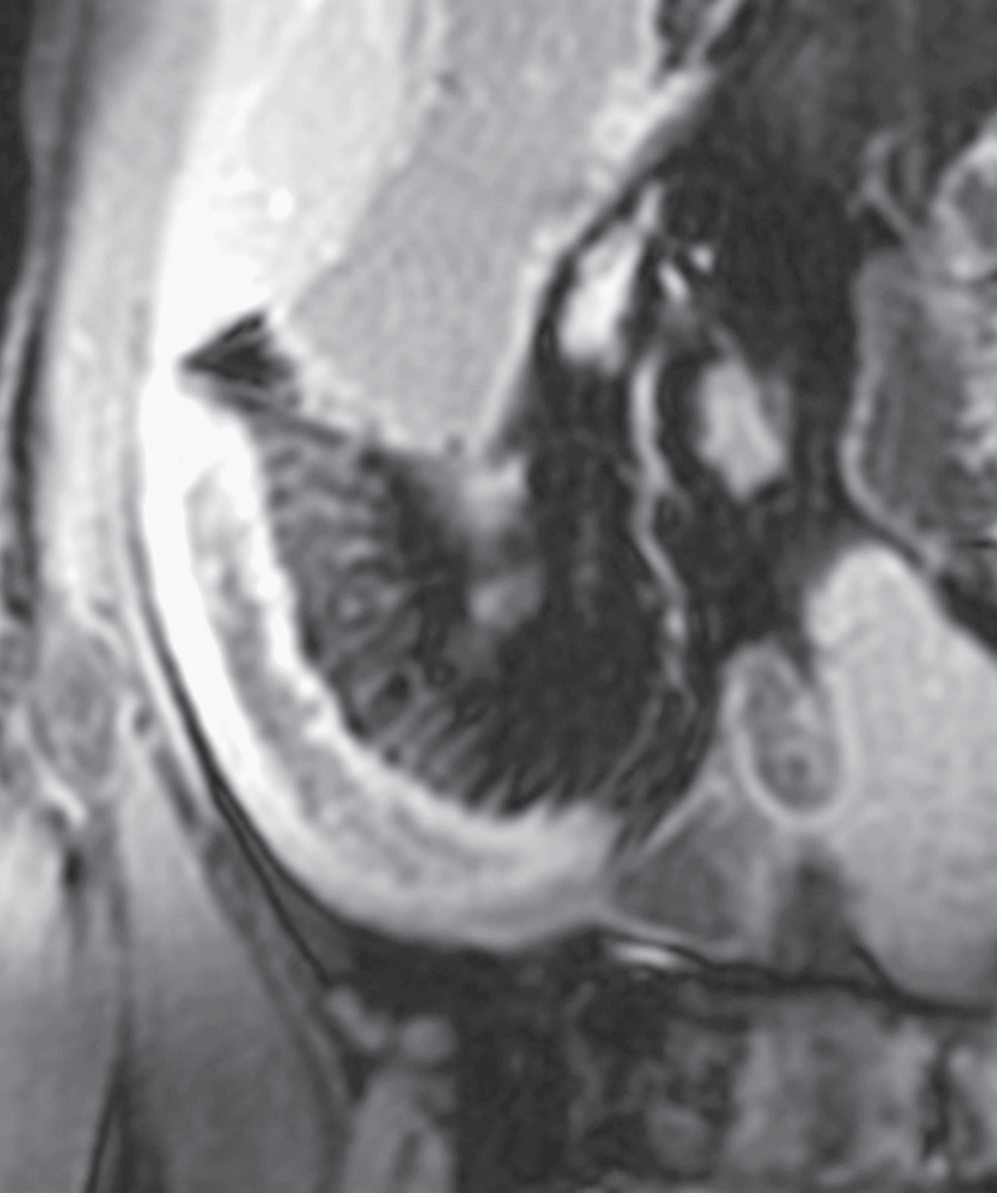
Imaging
- MR enterography (MRE): modality of choice for small bowel assessment; shows mural thickening, mural hyperenhancement, and the "comb sign" (engorged peri-enteric vasculature resembling comb teeth - see image below)
- CT enterography: alternative when MRI is unavailable
- Ultrasound: useful bedside tool for bowel wall thickening
Disease Activity Scoring
- Crohn's Disease Activity Index (CDAI): remission = CDAI <150; clinical response = decrease ≥100 points. Used in clinical trials.
- Symptoms alone should not guide therapy - objective assessment (endoscopy, CRP, fecal calprotectin, imaging) is required, as symptom scores don't always correlate with objective inflammation.
Treatment
2025 Paradigm Shift: Treat-to-Target / Early Advanced Therapy
Both the ACG (2025) and AGA (2025) guidelines represent a major shift: for moderate-to-severe CD, early initiation of advanced high-efficacy therapy is now preferred over the old "step-up" approach (failing aminosalicylates → thiopurines → biologics). The 2025 ACG guideline explicitly recommends against requiring patients to fail thiopurines or methotrexate before starting advanced therapies.
The treat-to-target goal is mucosal healing on endoscopy (not just symptom control).
Drug Classes
| Class | Agents | Role |
|---|---|---|
| Corticosteroids | Prednisone, budesonide | Induction of remission (NOT maintenance) |
| Immunomodulators | Azathioprine, 6-MP, methotrexate | Maintenance; combination with anti-TNF reduces immunogenicity |
| Anti-TNF | Infliximab, adalimumab, certolizumab, biosimilars | Induction + maintenance; first-line biologics |
| Anti-integrin | Vedolizumab (IV and SC) | Gut-selective; induction + maintenance |
| Anti-IL-12/23 | Ustekinumab (SC) | Induction + maintenance |
| Anti-IL-23 | Risankizumab, guselkumab, mirikuzumab | Newly incorporated in 2025 guidelines |
| JAK inhibitors | Upadacitinib | Incorporated in 2025 guidelines; moderate-to-severe CD |
| Dietary therapy | Mediterranean diet, Specific Carbohydrate Diet | Mild-to-moderate disease only (DINE-CD trial data) |
- Aminosalicylates (mesalazine) have minimal evidence in CD and are not generally recommended
- Antibiotics (metronidazole, ciprofloxacin) are used for perianal fistulas and abscesses, not as primary CD therapy
Perianal Fistulizing Disease
- Combined surgical drainage + anti-TNF (infliximab) is standard
- Emerging evidence: stem cell therapy (darvadstrocel/Alofisel) for complex perianal fistulas - a recent 2025 meta-analysis (PMID 40205247) confirms efficacy and safety
Surgery
Surgery is not curative but plays a major role:
- ~47% of patients require surgery within 10 years of diagnosis; rates have been declining with improved medical therapy
- ~30% require a second operation within 5 years of the first
- Guiding principle: preserve intestinal length - wide margins do not reduce recurrence
- Most common procedure: ileocecal resection (often laparoscopic)
- Strictureplasty: preferred over resection for scattered fibrotic strictures to preserve length
- Indications: intra-abdominal abscess, medically intractable fistula, fibrotic stricture with obstruction, growth failure in children, steroid-refractory/dependent disease, patient preference over immunosuppression
- The LIR:C trial showed that in limited (<40 cm) ileal CD failing steroids/immunomodulators, laparoscopic ileocecal resection vs. infliximab yielded equivalent quality of life at 12 months - surgery is a valid alternative for select patients
CD vs. Ulcerative Colitis: Key Distinctions
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Location | Any GI tract (mouth to anus) | Colon only |
| Pattern | Skip lesions, discontinuous | Continuous from rectum proximally |
| Depth | Transmural | Mucosal/submucosal |
| Granulomas | Yes (~50%) | No |
| Fistulas/strictures | Yes (common) | Rare |
| Smoking effect | Worsens CD | Protective in UC |
| Surgery | Not curative | Colectomy is curative |
Monitoring and Prognosis
- Mucosal healing (endoscopic remission) is the primary therapeutic target - biomarker and endoscopic monitoring is required even in asymptomatic patients
- Fecal calprotectin and CRP are useful non-invasive monitoring tools
- Patients on immunosuppressants/biologics require monitoring for infections (TB reactivation, hepatitis B reactivation), and regular skin/lymphoma surveillance
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapters 115, 116, 123
- Rheumatology (Elsevier, 2022), Chapter 38
- 2025 ACG Clinical Guideline: Management of Crohn's Disease in Adults
- AGA 2025 Living Guideline: Pharmacologic Management of Moderate-to-Severe CD
- PMID 40205247 - Stem cell therapy for anal fistulas (2025 meta-analysis)
This is a shared conversation. Sign in to Orris to start your own chat.