Precocious puberty
Reading File
Finding Sources
Searching PubMed
"precocious puberty"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Harrison's 22e (2025), Goldman-Cecil, and Textbook of Family Medicine. Let me compile the full answer.
Precocious Puberty
Definition
Precocious puberty is the onset of secondary sexual characteristics before age 8 in girls and age 9 in boys. Some guidelines (Lawson Wilkins Pediatric Endocrine Society) further specify that breast development or pubic hair in white girls before age 7 and black girls before age 6 warrants evaluation. For boys, the threshold is testicular enlargement >4 mL before age 9, associated with acceleration of linear growth and advancement of bone age.
Note: Over the past century, the mean age of pubertal onset has fallen by ~3 years, partly due to improved nutrition and rising obesity rates. This secular trend continues, making the diagnostic threshold somewhat debated.
Classification
Precocious puberty is broadly divided into two major types:
1. Central (GnRH-Dependent / True) Precocious Puberty (CPP)
- Caused by early activation of the hypothalamic-pituitary-gonadal (HPG) axis with premature GnRH pulsatility
- Leads to elevated LH, FSH, and sex steroids
- Isosexual (consistent with phenotypic sex)
2. Peripheral (GnRH-Independent / Pseudo-Precocious Puberty)
- Sex steroid secretion independent of LH/FSH stimulation
- Characterized by elevated sex steroids with suppressed gonadotropins
- Can be isosexual or heterosexual (contrasexual - e.g., virilization of a girl)
Incomplete (Partial / Benign Variants)
These do not require treatment in most cases:
- Isolated precocious thelarche - breast development without other signs, typically in girls <2 years; usually self-limited and resolves spontaneously
- Isolated precocious pubarche - pubic hair due to early adrenarche; usually self-limited
- Isolated premature menarche
- Adolescent gynecomastia in boys - social concern; self-limited
The majority (>75%) of children investigated for precocious puberty have benign diagnoses requiring no treatment. - Textbook of Family Medicine 9e
Causes
Central (GnRH-Dependent) - Boys
| Category | Causes |
|---|---|
| Idiopathic | No identifiable cause (less common in boys than girls) |
| CNS lesions | Hypothalamic hamartoma, optic glioma, arachnoid cysts, astrocytoma, ependymoma, tuberous sclerosis, inflammatory/infectious lesions |
| Genetic | Activating mutations in KISS1 (kisspeptin), KISS1R, or MKRN3 (makorin ring finger protein 3) |
In boys, a CNS lesion is found in ~2/3 of cases - always image!
Central (GnRH-Dependent) - Girls
- Idiopathic in the vast majority (~90%)
- CNS lesions less frequently found than in boys
Peripheral (GnRH-Independent)
| Cause | Notes |
|---|---|
| Congenital adrenal hyperplasia (CAH) | 21-hydroxylase or 11-beta-hydroxylase deficiency; elevated 17-OHP |
| hCG-secreting tumors | Germinomas (hypothalamic or pineal); stimulate Leydig cells in boys |
| McCune-Albright syndrome | Activating Gs-alpha mutations; polyostotic fibrous dysplasia + cafe-au-lait spots |
| Familial male-limited precocious puberty (testotoxicosis) | Activating LH receptor mutations; uncontrolled testosterone secretion |
| Adrenal tumors | Elevated testosterone + DHEAS |
| Leydig cell tumor of testis | Unilateral testicular enlargement |
| Exogenous sex steroids | Estrogen creams, anabolic steroids |
Tanner Staging (Reference)
The Tanner stages are used to assess pubertal progression:
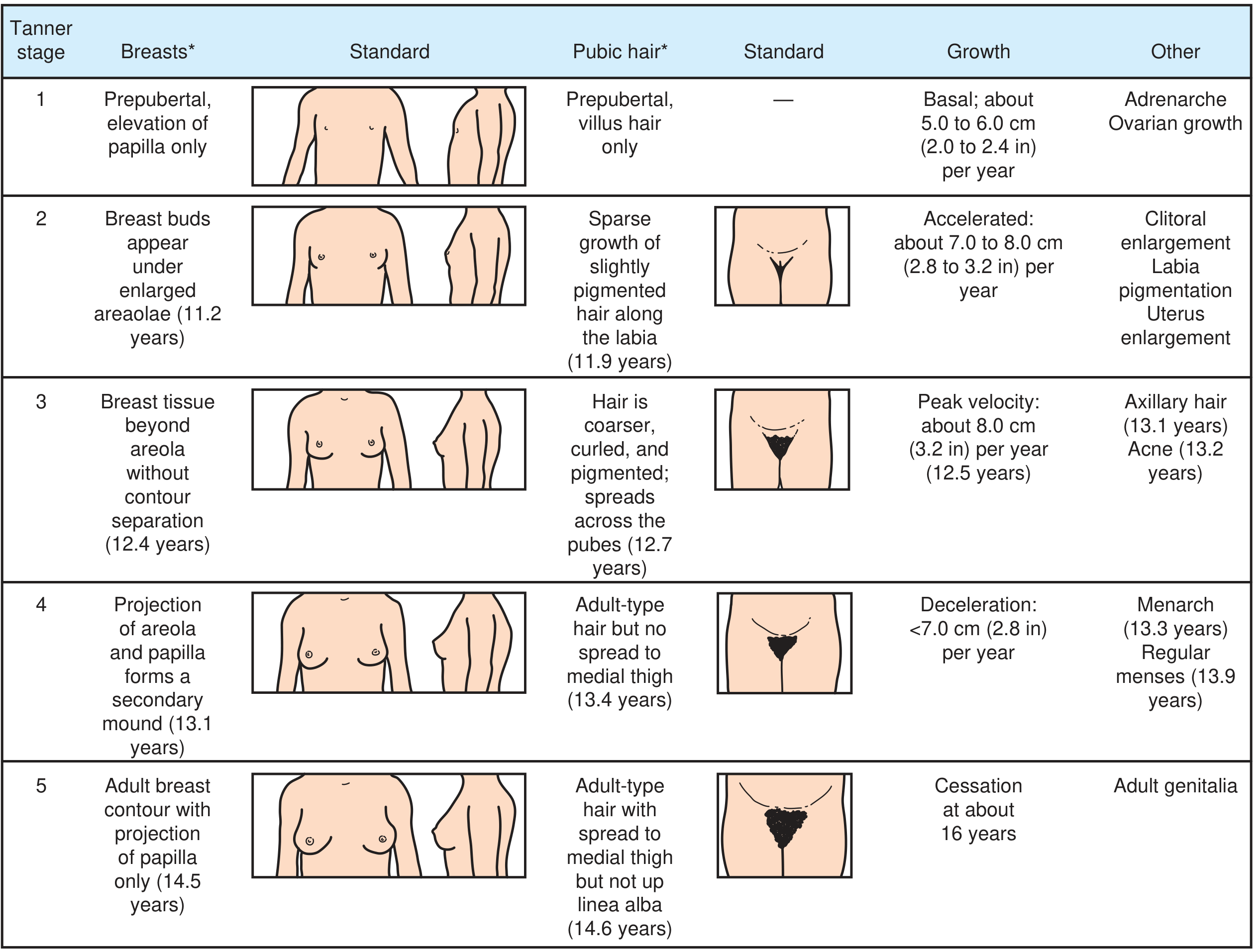
Tanner stages of puberty in girls based on breast size/shape and pubic hair distribution - Textbook of Family Medicine 9e
Clinical Features
- Accelerated linear growth (growth velocity above expected for age)
- Advanced bone age (leading to premature epiphyseal closure and reduced final adult height)
- Development of secondary sexual characteristics appropriate to sex (isosexual) or discordant (heterosexual)
- Psychosocial consequences: behavioral changes, early sexual awareness, peer difficulties
- Long-term risks of early puberty: increased risk of breast cancer, endometrial cancer, cardiovascular disease, hypertension, type 2 diabetes, and shorter lifespan
Diagnosis / Workup
Step 1 - History and Examination
- Age of onset, tempo (progressive vs. non-progressive)
- Family history (constitutional early puberty, CAH)
- Medications/topical exposures (estrogen creams)
- Growth chart review
- Tanner staging
Step 2 - Initial Labs
- Serum LH, FSH, testosterone/estradiol - distinguish central (elevated gonadotropins) from peripheral (suppressed gonadotropins)
- Bone age (wrist X-ray) - advanced bone age supports true precocity
- Morning testosterone in boys
Step 3 - Central PP confirmed (high LH + sex steroids)
- GnRH stimulation test (especially in girls): LH surge >5-8 IU/L after GnRH confirms CPP
- Brain MRI to exclude CNS lesions - mandatory in boys, strongly recommended in girls especially <6 years
Step 4 - Peripheral PP confirmed (high sex steroids, suppressed LH/FSH)
- 17-alpha-hydroxyprogesterone - elevated in CAH (21-OH deficiency)
- DHEAS - elevated in adrenal source
- If testosterone + 17-OHP elevated: ACTH stimulation test for CAH
- If testosterone + DHEAS elevated: CT adrenal glands for tumor
- If testosterone elevated without 17-OHP or DHEAS rise: testicular ultrasound for Leydig cell tumor
- If all above negative: consider activating LH receptor mutation (testotoxicosis) or Gs-alpha mutation (McCune-Albright)
Treatment
Central (GnRH-Dependent) Precocious Puberty
GnRH analogues are the mainstay of treatment. They work by downregulating GnRH receptors, suppressing gonadotropins and sex steroids. Effects:
- Halt early pubertal development
- Delay accelerated bone maturation
- Prevent premature epiphyseal closure
- Improve final adult height (most effective if started before age 6)
- Mitigate psychosocial consequences
- Do not cause osteoporosis
Agents and doses (Goldman-Cecil):
- Leuprolide acetate 3-month depot: 11.25 mg or 30 mg IM every 3 months
- Triptorelin 6-month depot: 22.5 mg every 6 months
When to treat: Rapid pubertal progression, Tanner stage ≥3, rapid linear growth, significant bone age advancement, or psychological distress. Slowly progressive forms in older girls may be observed without treatment.
When to stop: Generally at 11-11.5 years of chronologic age. Puberty resumes after discontinuation.
Counseling is an essential component of management.
Peripheral (GnRH-Independent) Precocious Puberty
Treatment is directed at the underlying cause:
| Cause | Treatment |
|---|---|
| CAH | Glucocorticoids (hydrocortisone 15 mg/m²/day) |
| CNS lesion | Surgery, radiation, or medical management per lesion type |
| Adrenal/gonadal tumor | Surgical resection |
| McCune-Albright / testotoxicosis | Ketoconazole (10-20 mg/kg/day) to suppress steroidogenesis ± antiandrogen (spironolactone 5-7 mg/kg/day or bicalutamide 2 mg/kg/day); aromatase inhibitors (testolactone, letrozole) as adjuncts; abiraterone under investigation |
| Exogenous sex steroids | Remove the source |
Key Points Summary
| Feature | Central (CPP) | Peripheral |
|---|---|---|
| GnRH dependence | Yes | No |
| LH/FSH | Elevated (pubertal range) | Suppressed |
| Sex steroids | Elevated | Elevated |
| GnRH stimulation test | LH surge | No LH surge |
| Common in girls | Idiopathic (90%) | Less common |
| Common in boys | CNS lesion (2/3) | CAH, testotoxicosis |
| Treatment | GnRH analogues | Treat underlying cause |
Sources: Harrison's Principles of Internal Medicine 22e (2025), Goldman-Cecil Medicine, Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.