Why in a patient already having permanent pacemaker implant having ventricular tachycardia
Reading File
Finding Sources
Finding Sources
Searching the Web
ventricular tachycardia in patients with permanent pacemaker causes mechanisms
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough, well-cited answer. Here it is:
Ventricular Tachycardia in a Patient with a Permanent Pacemaker
This is an important clinical scenario. VT occurring in a pacemaker patient has both pacemaker-related and non-pacemaker-related causes - and distinguishing them changes management entirely.
A. Pacemaker-Specific Causes of VT/Rapid Ventricular Pacing
1. Pacemaker-Mediated Tachycardia (PMT) / "Endless Loop Tachycardia"
This is the classic pacemaker-specific tachycardia. It occurs exclusively with dual-chamber (DDD/VDD) pacemakers.
Mechanism:
- A premature ventricular contraction (PVC) or paced ventricular beat conducts retrogradely back to the atrium via the AV node (or an accessory pathway)
- This retrograde atrial depolarization occurs after the Post-Ventricular Atrial Refractory Period (PVARP)
- The atrial lead senses this retrograde P wave and triggers a ventricular paced beat (after the set AV delay)
- This paced ventricular beat again conducts retrogradely - forming a closed reentrant loop between the ventricle, AV node, atrium, and pacemaker circuitry
- The tachycardia runs at the programmed upper rate limit of the pacemaker
The pacemaker essentially acts as the "antegrade limb" of the reentry circuit - this is why it is called pacemaker-mediated.
Key feature: Rate is fixed at the programmed upper rate limit (e.g., 120-180 bpm). The StatPearls PMT article notes that retrograde VA conduction - the prerequisite - is present in 30-80% of pacemaker patients.
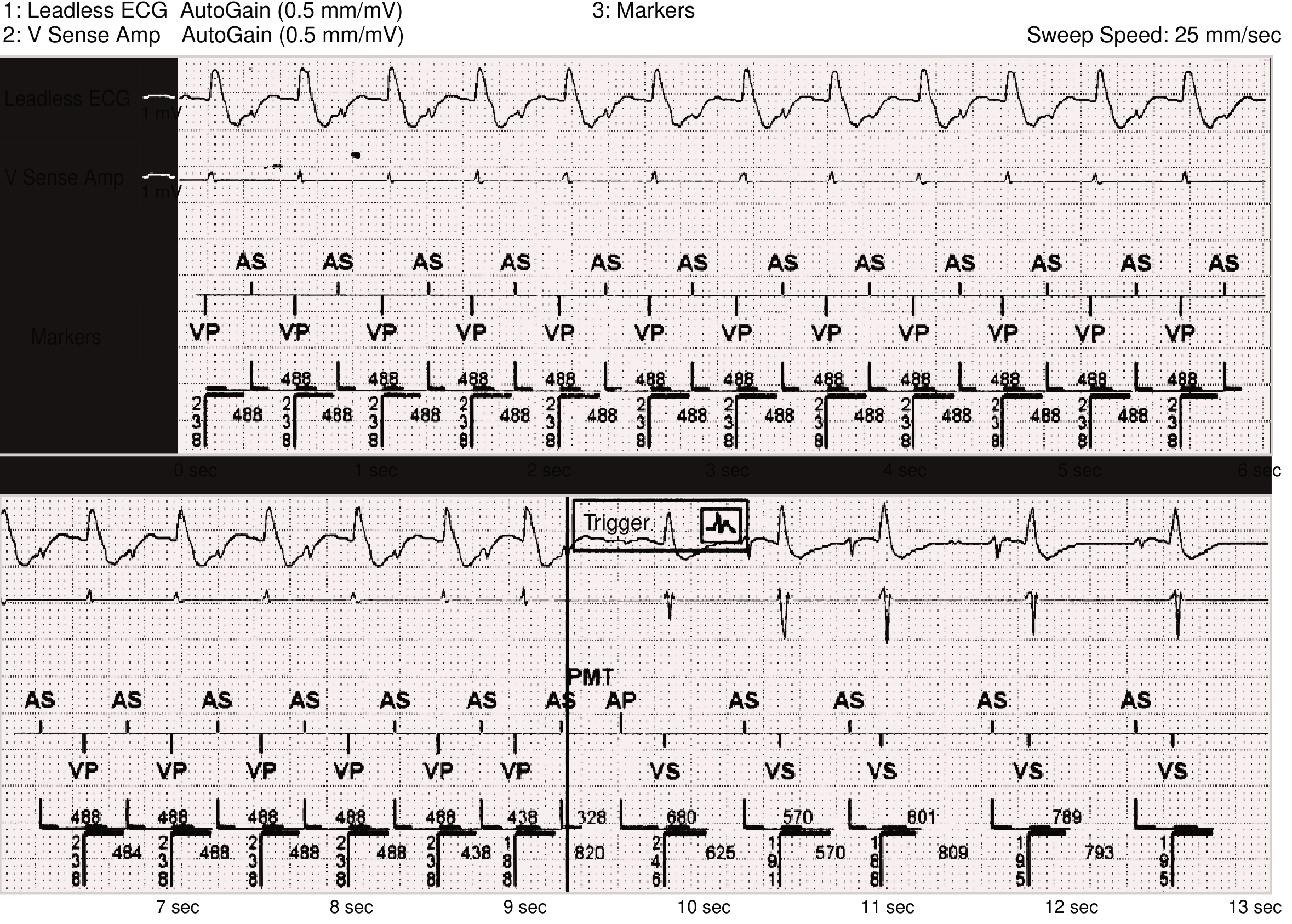
Pacemaker-Mediated Tachycardia (PMT) - Braunwald's Heart Disease. Top panel: regular AS (atrial sensed) → VP (ventricular paced) cycles at fixed interval = PMT. Bottom panel: algorithm extends PVARP at one beat, terminating the loop.
Treatment:
- Apply a magnet over the pacemaker - converts to asynchronous mode, breaks the loop
- Reprogram PVARP to extend it beyond VA conduction time
- Modern pacemakers have automated PMT detection and termination algorithms
2. Tracking of Rapid Atrial Arrhythmias
In DDD mode (without mode switch), when the patient develops atrial flutter or atrial fibrillation, the pacemaker tracks the atrial rate and drives the ventricles at the upper rate limit. This produces a rapid, regular paced wide-complex rhythm that looks like VT on the surface ECG.
- Tintinalli's Emergency Medicine notes: "Unless preprogrammed to mode switch, pacemakers detect rapid atrial rhythms and track them, resulting in pacing at the upper rate limit."
- Solution: mode-switch programming (DDI or DDIR fallback)
3. Runaway Pacemaker
A rare but dangerous failure where the pulse generator discharges at a rate above its preset upper limit, typically >200 bpm. Caused by:
- Battery failure / depletion
- Circuit damage from external electromagnetic interference or radiation
- Component failure
This can degenerate into true VT or VF. A magnet may help temporarily, but the device must be replaced - Tintinalli's Emergency Medicine.
4. Pacemaker Stimulus Triggering True VT
The pacemaker lead tip sits in the RV apex, and if it fires during the vulnerable period (R-on-T), it can trigger VT or VF. This was a significant problem with old asynchronous (VOO) pacemakers - fixed-rate pacing without sensing. Roberts & Hedges' Clinical Procedures notes: "Asynchronous pacing frequently resulted in the pacemaker firing during the vulnerable period... occasionally caused ventricular tachycardia or fibrillation."
Modern demand pacemakers (sense-inhibit mode) essentially eliminated this risk.
5. Lead-Related Issues Causing VT
- Fractured or displaced lead producing erratic stimuli at multiple ventricular sites
- Oversensing of noise (electromagnetic interference, myopotentials, T-wave oversensing) causing inappropriate pacing outputs that fall on vulnerable repolarization periods - Braunwald's Heart Disease
B. Non-Pacemaker Causes of VT in a Pacemaker Patient
These are at least as common and must not be overlooked. The underlying reason the patient received a pacemaker (structural heart disease) is often itself the substrate for VT.
| Cause | Mechanism |
|---|---|
| Ischemic cardiomyopathy / prior MI | Scar-related reentry (most common cause of sustained monomorphic VT) |
| Dilated cardiomyopathy | Diffuse fibrosis creating multiple reentry circuits |
| Hypertrophic cardiomyopathy | Disorganized myocyte architecture |
| Electrolyte disturbances | Hypokalemia, hypomagnesemia, hypocalcemia - alter membrane excitability |
| Drug effects | Antiarrhythmics (pro-arrhythmia), digoxin toxicity, QT-prolonging drugs |
| Acute myocardial ischemia | Altered conduction in peri-ischemic zone |
| Worsening heart failure | Increased wall stress, catecholamine surge |
Roberts & Hedges specifically states: "Although ventricular tachycardia and ventricular fibrillation have been reported to result from pacemakers, these dysrhythmias are rare. Therefore patients with such dysrhythmias should be evaluated for a non-pacemaker-induced cause."
C. Non-Reentrant VA Synchrony (RNRVAS)
A subtler pacemaker-related rhythm where a PVC conducts retrogradely but falls within the PVARP, so the atrial channel is not triggered. However, atrial pacing occurs at the lower rate limit but fails to capture (functional refractoriness). The sequence repeats, producing a pseudo-tachycardia that is distinct from true PMT - Braunwald's Heart Disease.
Summary: How to Approach This Clinically
- Is it truly wide complex VT or rapid paced rhythm? - pacemaker artifacts (spikes), fixed rate at upper limit, and mode should all be checked
- What pacemaker mode? - DDD/VDD enables PMT; VVI/AAI does not
- Magnet test - applying a magnet temporarily converts to asynchronous mode; if the tachycardia terminates, it was PMT
- Device interrogation - essential to review intracardiac electrograms (EGMs), stored episodes, and lead parameters
- Rule out ischemia, electrolyte abnormality, and drug effects - even in pacemaker patients
Key distinction: PMT = regular rate at upper rate limit with pacemaker spikes, breakable with magnet. True VT = irregular/variable, not at upper rate limit, will NOT break with magnet, requires cardioversion/ICD therapy.
Sources: Tintinalli's Emergency Medicine, p.263 | Braunwald's Heart Disease, p.607 | Roberts & Hedges' Clinical Procedures in Emergency Medicine | StatPearls - PMT | PMC - Pacemaker-Mediated Arrhythmias
This is a shared conversation. Sign in to Orris to start your own chat.