35yr women with heavy menstrual bleeding with clots and severe cramping, usg s/o large,irregularly shaped mass in uterus. Whats is Diagnosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"uterine fibroids" AND "heavy menstrual bleeding"
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
uterine fibroid leiomyoma ultrasound
Reading File
I now have comprehensive information. Let me compile the full clinical answer.
Diagnosis: Uterine Leiomyoma (Fibroid)
This is the most likely diagnosis based on the classic triad:
- 35-year-old premenopausal woman
- Heavy menstrual bleeding (menorrhagia) with clots + severe dysmenorrhea
- Ultrasound showing a large, irregularly shaped uterine mass
What Are Uterine Fibroids?
Uterine leiomyomas are benign monoclonal tumors arising from smooth muscle cells of the myometrium, stimulated by estrogen and progesterone. They are the most common pelvic tumor in women, occurring in up to 70–80% of women by age 50, though most are asymptomatic.
Why This Presentation Fits
| Feature | Significance |
|---|---|
| Age 35, premenopausal | Peak symptomatic age; estrogen-driven growth |
| Heavy bleeding with clots | Submucosal/intramural fibroids distort endometrial vasculature, impairing hemostasis |
| Severe cramping | Uterine attempts to expel submucosal fibroids; prostaglandin excess |
| Irregularly enlarged uterus on USG | Multiple fibroids create a lobulated, asymmetric contour — classic "lumpy-bumpy" uterus |
As stated in Berek & Novak's Gynecology: "Clinically significant subserosal and intramural fibroids can usually be diagnosed by pelvic examination based on findings of an enlarged, irregularly shaped, firm, and nontender uterus."
FIGO Classification of Fibroid Location
Fibroids most likely to cause heavy bleeding are submucosal (Types 0–2):
- Type 0 — Pedunculated, entirely within the cavity
- Type 1 — <50% intramural
- Type 2 — ≥50% intramural
- Types 3–4 — Intramural (cause bulk symptoms + bleeding)
- Types 5–7 — Subserosal (mainly bulk/pressure symptoms)
Pathophysiology of Bleeding
- Increased endometrial surface area due to cavity distortion
- Impaired myometrial contractility around fibroid — uterus can't compress spiral arteries effectively
- Increased vascularity and angiogenesis around fibroids
- Prostaglandin imbalance → uterine cramping and heavy flow
Ultrasound Findings (Classic)
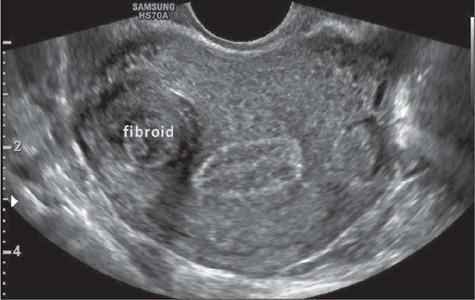

Typical USG findings:
- Heterogeneous, hypoechoic solid mass with well-defined margins
- May show posterior acoustic shadowing (dense fibrous tissue)
- Enlarged, lobulated uterine contour
- Multiple lesions possible
Differential Diagnosis to Consider
| Condition | Distinguishing Features |
|---|---|
| Adenomyosis | Diffuse uterine enlargement, globular shape, heterogeneous myometrium; no discrete mass |
| Endometrial polyp | Focal intracavitary lesion; smaller; best seen on SIS/hysteroscopy |
| Uterine sarcoma (LMS) | Rare at 35; more common postmenopausal; rapid growth, heterogeneous; requires MRI/biopsy |
| Ovarian mass | Separate from uterus on USG; different origin |
⚠️ Note: The textbook emphasizes that "rapid growth almost never indicates uterine sarcoma in premenopausal women" — sarcoma mean age is 55–68 years. However, if imaging shows atypical features, MRI is warranted.
Investigations
- Transvaginal USG — first-line; confirms size, location, number
- Saline infusion sonography (SIS) or hysteroscopy — for submucosal fibroids
- MRI pelvis — gold standard for mapping multiple fibroids pre-operatively; distinguishes fibroid from sarcoma
- CBC — assess anemia from chronic blood loss
- Serum ferritin — iron deficiency
- TFTs — rule out hypothyroidism as co-contributor to HMB
- Endometrial biopsy — if endometrial pathology suspected (age >40 or irregular bleeding)
Management Overview
Medical (preserve fertility/temporize):
- GnRH agonists/antagonists (e.g., leuprolide, relugolix) — reduce fibroid volume 30–50%; used preoperatively (recent 2025 Cochrane review [PMID: 40183418] supports preoperative GnRH therapy)
- Levonorgestrel IUS (Mirena) — reduces bleeding for smaller fibroids not distorting cavity
- Tranexamic acid / NSAIDs — symptomatic relief of bleeding and cramping
- Combined OCP — cycle regulation
Surgical:
- Hysteroscopic myomectomy — for submucosal fibroids (Types 0–2); fertility-preserving
- Laparoscopic/open myomectomy — for intramural/subserosal fibroids; fertility-preserving
- Hysterectomy — definitive cure; for completed family or failed conservative management
- Uterine artery embolization (UAE) — minimally invasive; good for multiple fibroids; reduces fertility potential
Key Points
- Most common pelvic tumor in women; peak symptoms in reproductive age (30s–40s)
- Driven by estrogen + progesterone → regress after menopause
- Submucosal location causes the heaviest bleeding
- Irregularly enlarged uterus on USG is the hallmark finding
- Treatment depends on symptom severity, fibroid location, size, and fertility wishes
— Berek & Novak's Gynecology; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.