Tuberculosis
Reading File
Finding Sources
Searching PubMed
"tuberculosis"[MeSH Terms] AND "treatment"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-based overview of Tuberculosis.
Tuberculosis (TB)
Definition and Etiology
Tuberculosis is a chronic communicable granulomatous disease caused by Mycobacterium tuberculosis, a rod-shaped, non-spore-forming, obligate aerobe measuring ~0.5 x 3 μm. In 2023, after being displaced by COVID-19 for three years, TB likely returned as the leading infectious cause of death from a single pathogen. The WHO estimated 1.3 million TB deaths and 5.8 million new cases in 2021.
Key microbiologic features:
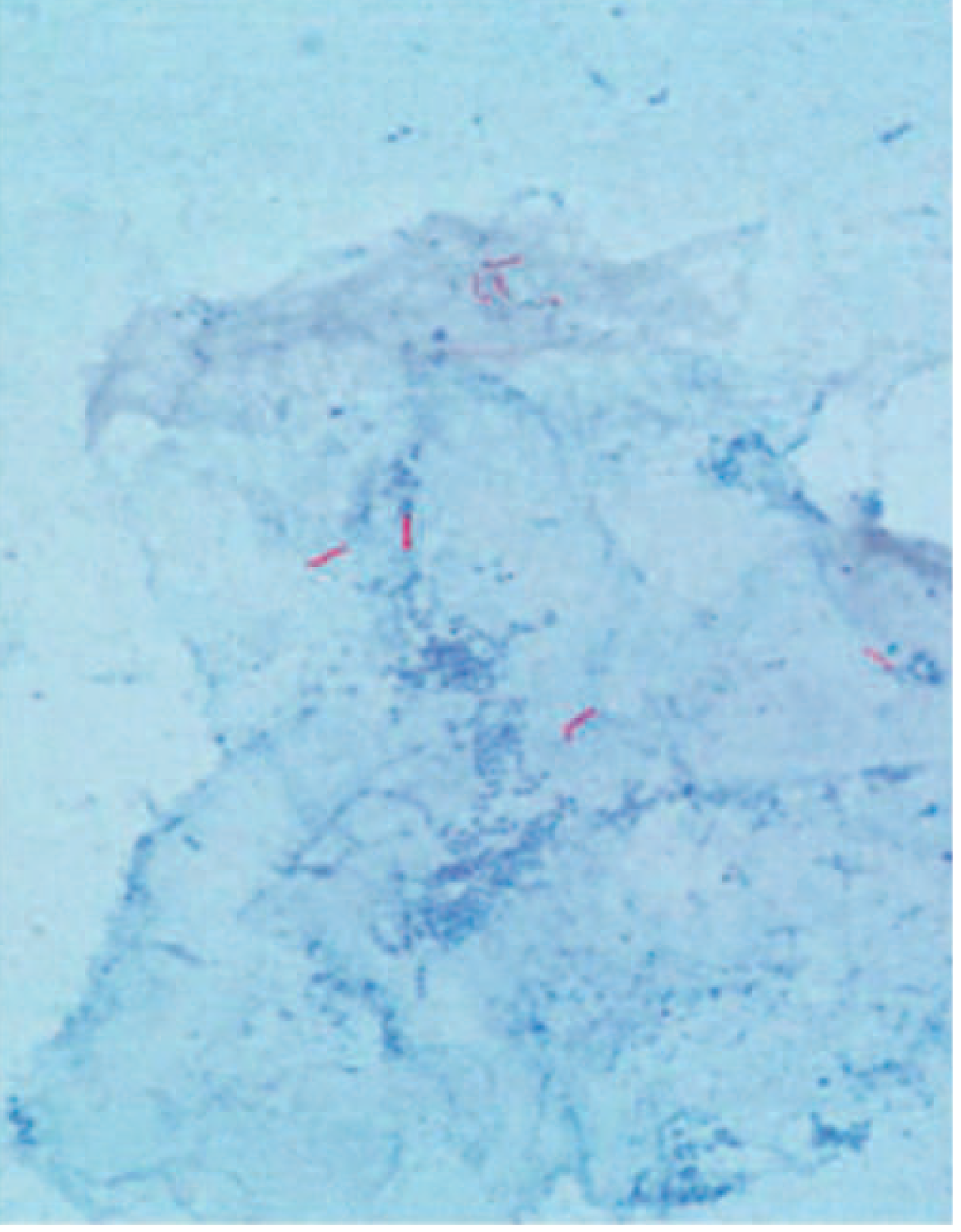
- Gram-stain neutral, but acid-fast - the hallmark characteristic. High mycolic acid content in the cell wall prevents decolorization by acid-alcohol after carbol fuchsin staining
- Extremely slow growth: doubles every 18-24 hours; cultures may take up to 10 weeks
- The complex, waxy cell envelope (mycolic acids, arabinogalactan, peptidoglycan, unique lipids like phthioceral dimycocerosate and trehalose dimycolates) creates a formidable barrier to antibiotic penetration
- Facultative anaerobe that can replicate intracellularly within macrophages
M. tuberculosis acid-fast bacilli under Ziehl-Neelsen stain (red rods on blue background):
The M. tuberculosis complex includes related species:
- M. africanum - causes TB in West/Central/East Africa
- M. bovis - transmitted via unpasteurized dairy; intrinsically pyrazinamide-resistant
- M. caprae, M. pinnipedii, M. microti - zoonotic members
Epidemiology and Risk Factors
TB flourishes in poverty, crowding, and chronic debilitating illness. High-risk groups include:
- HIV/AIDS patients (dominant risk factor in HIV-endemic regions; CD4 <200/μL carries greatest risk)
- The urban poor, elderly, foreign-born
- Patients with diabetes, Hodgkin lymphoma, silicosis, CRF, malnutrition, alcohol use disorder, immunosuppression
- Approximately 13 million people have latent TB in the United States (2019)
- ~80% of populations in some Asian and African countries are tuberculin-positive
Pathogenesis and Immunity
Transmission is via airborne droplet nuclei from a person with active pulmonary TB. Droplet nuclei are generated when infected individuals cough, sneeze, or speak - they are small enough to remain suspended in air and reach the alveoli.
Sequence of events after inhalation:
- Bacilli inhaled, reach alveolar spaces - phagocytosed by alveolar macrophages
- Mycobacteria evade phagolysosomal killing (via lipoarabinomannan inhibiting phagosome maturation)
- Local replication triggers cytokine release (TNF, IL-1, IL-12); Th1 CD4+ T-cell response develops
- Cell-mediated immunity (CMI) develops over 2-8 weeks, controlled by IFN-γ-activated macrophages
- Characteristic caseating granulomas form - epithelioid macrophages, Langhans giant cells, central caseous necrosis, surrounded by lymphocytes and fibroblasts
- In ~95% of immunocompetent individuals, the primary infection is controlled and becomes latent
Primary vs. Secondary (Reactivation) TB
Primary TB
- Develops in the previously unexposed, unsensitized host
- About 5% of newly infected immunocompetent individuals develop significant disease
- Lesion typically forms in the lower part of the upper lobe or upper part of the lower lobe (areas receiving the most inspired air)
- Forms a Ghon focus: 1-1.5 cm gray-white area of consolidation with central caseous necrosis
- Regional lymph node involvement (caseous) + Ghon focus = Ghon complex
- On healing, fibrosis and calcification form the Ranke complex (visible on X-ray)
- Lymphatic/hematogenous dissemination occurs in early weeks, seeding distant organs
CXR showing right hilar lymphadenopathy with infiltration in primary TB in a child:

Secondary (Reactivation) TB
- Arises in a previously sensitized host - either from reactivation of dormant foci (decades later) or reinfection
- Less than 5% of patients with primary TB develop secondary TB
- Classically localizes to the apex of one or both upper lobes (possibly due to high oxygen tension)
- Prompt tissue response walls off the focus; regional lymph nodes are less prominently involved
- Cavitation is common: central caseous material liquefies and drains into bronchi, forming cavities (which are a major source of infectivity)
- Hallmark: productive chronic cough, hemoptysis, fever, night sweats, weight loss
Clinical Manifestations
Pulmonary TB (most common)
| Symptom | Notes |
|---|---|
| Cough | Initially dry, then productive and purulent |
| Hemoptysis | Present in ~50% of pulmonary cases |
| Fever | Low-grade, remittent; classically appears late afternoon |
| Night sweats | Classic constitutional feature |
| Weight loss, anorexia, malaise | Mediated by TNF and IL-1 from activated macrophages |
| Pleuritic chest pain | Extension of infection to pleural surfaces |
Extrapulmonary TB
Occurs in 10-40% of all TB patients; up to two-thirds of HIV-infected TB patients may have extrapulmonary involvement. Sites include:
| Site | Manifestation |
|---|---|
| Lymph nodes | Scrofula - cervical lymphadenitis (most common extrapulmonary form) |
| Pleura | Pleural effusion with exudative, lymphocyte-predominant fluid |
| CNS | Tuberculous meningitis: headache, neurologic deficits, high CSF protein, low glucose |
| Spine | Pott disease - vertebral collapse, back pain, paraplegia |
| Kidney | Hematuria, sterile pyuria, "putty kidney" calcification |
| Female genital tract | Salpingitis presenting as infertility |
| Pericardium | Constrictive pericarditis |
| Adrenal glands | Addison's disease |
| Disseminated | Miliary TB - hematogenous spread creating millet-seed size lesions in multiple organs |
Diagnosis
Tests for TB Infection (Latent TB)
-
Tuberculin Skin Test (TST / Mantoux / PPD)
- Intradermal injection of purified protein derivative
- Induration read at 48-72 hours
- Positive if ≥10 mm (≥5 mm in HIV+ patients/close contacts/immunosuppressed)
- Limitations: false-negative with anergy (HIV, malnutrition, overwhelming TB, sarcoidosis, Hodgkin's); false-positive from BCG vaccination and atypical mycobacteria
-
Interferon-Gamma Release Assays (IGRAs) (QuantiFERON-TB Gold, T-SPOT.TB)
- In vitro: patient T cells stimulated with M. tuberculosis antigens; IFN-γ production measured
- More specific than TST; not affected by BCG vaccination
- Both TST and IGRA cannot differentiate infection from active disease
Tests for Active TB
| Method | Details |
|---|---|
| Sputum AFB smear | Acid-fast staining (Ziehl-Neelsen or fluorescent auramine-rhodamine); most common first-line method |
| Culture | Gold standard; liquid media (radiometric assay) gives result in ~2 weeks vs. 10 weeks for solid media; required for drug-susceptibility testing |
| PCR / NAAT (e.g., Xpert MTB/RIF) | Rapid; can be done on sputum or tissue; detects M. tuberculosis and rifampin resistance simultaneously |
| CXR | Upper lobe infiltrates, cavitation in secondary TB; hilar adenopathy in primary TB |
| Bronchoscopy/BAL | When sputum cannot be obtained |
Treatment
Drug-Susceptible TB - Standard Regimen
Treatment uses two phases with directly observed therapy (DOT):
Intensive Phase (2 months): HRZE
- H - Isoniazid (INH)
- R - Rifampicin (Rifampin)
- Z - Pyrazinamide
- E - Ethambutol
Continuation Phase (4 months): HR (or HRE)
- Isoniazid + Rifampicin (+/- Ethambutol)
- Total duration: 6 months for most drug-susceptible pulmonary TB
- Extension by 12-24 weeks for CNS TB, skeletal TB, and disseminated TB
Key Drug Properties and Side Effects
| Drug | Mechanism | Key Adverse Effects |
|---|---|---|
| Isoniazid (H) | Inhibits mycolic acid synthesis (InhA) | Hepatotoxicity, peripheral neuropathy (prevent with pyridoxine/B6), drug-induced lupus |
| Rifampicin (R) | Inhibits RNA polymerase (beta subunit) | Hepatotoxicity, orange body fluids, potent CYP450 inducer (numerous drug interactions) |
| Pyrazinamide (Z) | Disrupts membrane energy metabolism (in acidic environment) | Hepatotoxicity, hyperuricemia/gout, arthralgias |
| Ethambutol (E) | Inhibits arabinosyltransferase (arabinogalactan synthesis) | Optic neuritis (monthly visual acuity/color vision monitoring required) |
Monitoring During Treatment
- Baseline: LFTs (ALT, bilirubin), creatinine, platelets, hepatitis serology
- Monthly: assessment for hepatotoxicity symptoms (nausea, vomiting, jaundice)
- Stop hepatotoxic drugs if ALT >5x ULN (or >3x ULN with symptoms)
- Monthly sputum cultures until clearance confirmed
- Monthly dispensing allows essential clinical monitoring
Latent TB Infection (LTBI) Treatment
Options include:
- 9H: 9 months of daily isoniazid (most widely used)
- 4R: 4 months of daily rifampicin
- 3HP: 3 months of weekly isoniazid + rifapentine (directly observed)
- 1HP: 1 month of daily isoniazid + rifapentine (newer regimen)
Drug-Resistant TB
- MDR-TB: Resistance to at least isoniazid AND rifampicin - the two most potent first-line drugs
- XDR-TB: MDR-TB + resistance to fluoroquinolones AND at least one injectable agent (bedaquiline, linezolid)
- WHO estimated 465,000 MDR-TB cases in 2019 (~3% of new cases, ~20% of previously treated cases)
- Epicenter: Eastern Europe, Russia, parts of Africa and Asia
- MDR-TB treatment requires 18-24+ months with second-line drugs (bedaquiline, delamanid, linezolid, fluoroquinolones); treatment is more toxic and less effective
Prevention and Control
- BCG vaccination: Effective against miliary TB and TB meningitis in children; provides variable protection against pulmonary TB in adults
- LTBI treatment: Prevents progression from infection to active disease
- Infection control: Airborne isolation of active cases; N95 respirators for healthcare workers; negative-pressure rooms; UV germicidal irradiation
- Contact tracing and DOT: Systematic identification and treatment of close contacts
- HIV treatment: ART markedly reduces TB risk in HIV-infected individuals
Prognosis
- Drug-susceptible TB properly treated: >95% cure rate
- Untreated active TB: fatal in >70% of cases
- MDR-TB: significantly worse outcomes, prolonged treatment, higher toxicity
- HIV co-infection: substantially increases morbidity and mortality
Sources: Harrison's Principles of Internal Medicine 22E (2025), Robbins & Kumar Basic Pathology, Goldman-Cecil Medicine, Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.