Abg
Hey! It looks like your message got cut off. Did you mean to ask about ABG (Arterial Blood Gas)? Or something else?
Let me know what you'd like to know - for example:
- ABG interpretation
- Normal ABG values
- A specific ABG result you want analyzed
- Something else entirely
Abg interpretation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a complete, systematic guide to ABG interpretation drawn from Current Surgical Therapy 14e and Barash's Clinical Anesthesia 9e:
ABG Interpretation: Step-by-Step
Normal Values
| Parameter | Normal Value | Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO2 | 40 mmHg | 38 - 42 mmHg |
| HCO3- | 24 mEq/L | 22 - 26 mEq/L |
| PaO2 | 100 mmHg | 75 - 100 mmHg |
| SaO2 | - | >95% |
Step 1 - Check pH
| pH | Interpretation |
|---|---|
| < 7.35 | Acidemia |
| 7.35 - 7.45 | Normal |
| > 7.45 | Alkalemia |
Step 2 - Identify Primary Process
Look at PaCO2 and HCO3- direction:
| pH | PaCO2 | HCO3- | Primary Disorder |
|---|---|---|---|
| pH ↓ | ↑ | normal/slightly ↑ | Respiratory acidosis |
| pH ↓ | normal/slightly ↓ | ↓ | Metabolic acidosis |
| pH ↑ | ↓ | normal/slightly ↓ | Respiratory alkalosis |
| pH ↑ | normal/slightly ↑ | ↑ | Metabolic alkalosis |
Key rule: In respiratory disorders, PaCO2 moves opposite to pH. In metabolic disorders, PaCO2 and pH move in the same direction.
Step 3 - Assess Compensation
Check if the body has appropriately compensated. If compensation is beyond expected, a mixed disorder is present.
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO2 = 1.5 × [HCO3-] + 8 ± 2 (Winter's Formula) |
| Metabolic alkalosis | PaCO2 = 0.7 × [HCO3-] + 20 ± 5 |
| Acute respiratory acidosis | ↑ HCO3- = ΔPaCO2 / 10 |
| Chronic respiratory acidosis | ↑ HCO3- = 4 × (ΔPaCO2 / 10) |
| Acute respiratory alkalosis | ↓ HCO3- = 2 × (ΔPaCO2 / 10) |
| Chronic respiratory alkalosis | ↓ HCO3- = 5 × (ΔPaCO2 / 10) |
Step 4 - Calculate Anion Gap (AG)
Always calculate AG, even if metabolic acidosis isn't the primary diagnosis - a hidden AG metabolic acidosis can be masked in a mixed disorder.
AG = Na+ - (Cl- + HCO3-)
- Normal AG: < 12 mEq/L
- Correct for albumin: Add 2.5 × (4 - measured albumin) to the observed AG
High AG Metabolic Acidosis - MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia |
| D | Diabetic ketoacidosis |
| P | Propylene glycol / Paracetamol |
| I | Isoniazid / Iron |
| L | Lactic acidosis |
| E | Ethylene glycol |
| S | Salicylates |
Non-AG Metabolic Acidosis - HARDUPS / causes
- GI bicarbonate loss (diarrhea, fistulas)
- Renal tubular acidosis
- Normal saline infusion (hyperchloremic)
- Urine anion gap helps distinguish GI vs renal cause
Step 5 - Check the Delta-Delta Ratio (if AG elevated)
Δ/Δ = (AG - 12) / (24 - HCO3-)
| Ratio | Interpretation |
|---|---|
| < 1.0 | Pure AG acidosis + concurrent non-AG metabolic acidosis |
| 1.0 - 2.0 | Pure AG metabolic acidosis |
| > 2.0 | AG acidosis + concurrent metabolic alkalosis (or chronic respiratory acidosis) |
Step 6 - Assess Oxygenation
- PaO2 < 80 mmHg = Hypoxemia
- A-a gradient = PAO2 - PaO2 (normal < 15 mmHg on room air)
- PAO2 = FiO2 × (Patm - 47) - PaCO2/0.8
- Elevated A-a gradient suggests V/Q mismatch, diffusion defect, or shunt
Step 7 - Calculate Base Deficit (surgical/ICU context)
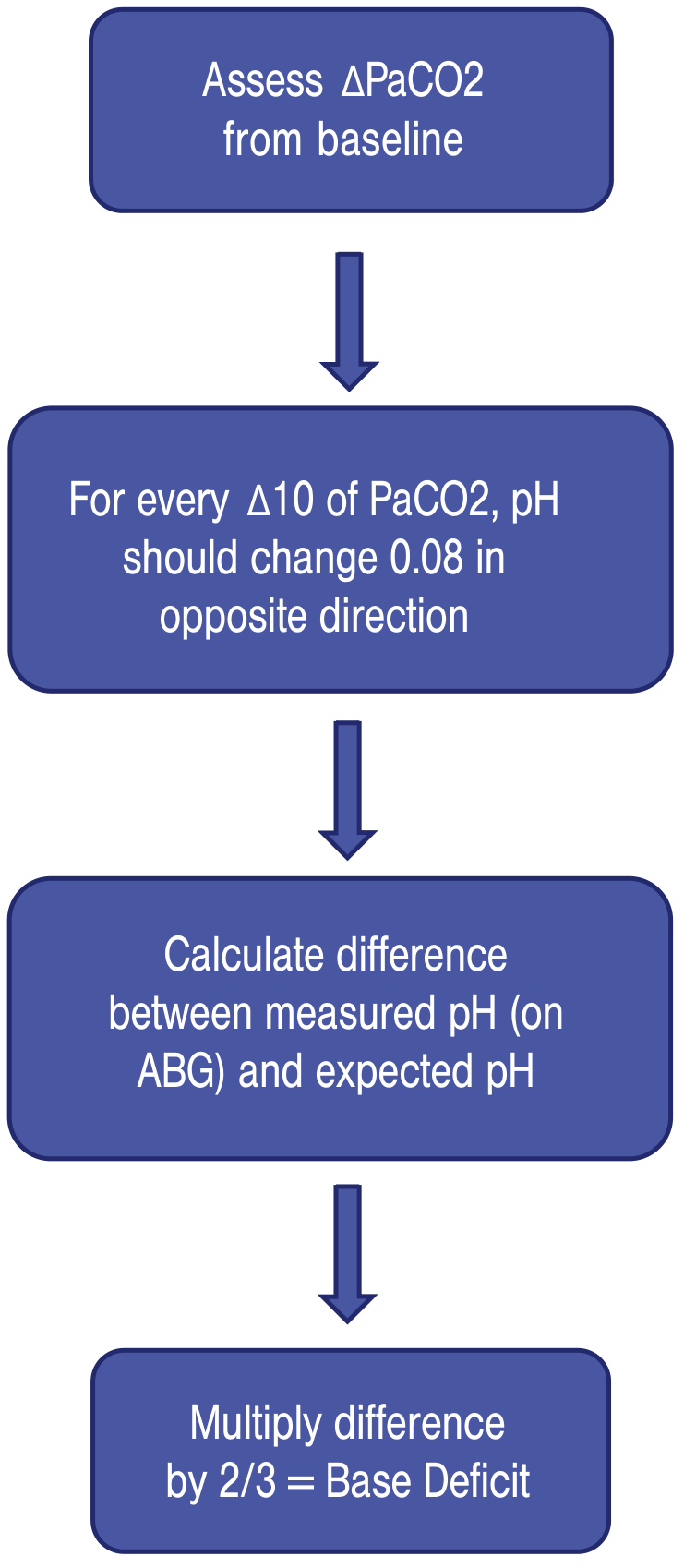
- For every 10 mmHg change in PaCO2, pH changes 0.08 in the opposite direction
- Base deficit = (measured pH - expected pH) × 2/3
- Base deficit > +4 or < -4 is abnormal
- Positive = alkalosis; Negative = acidosis
Quick Reference: Common Patterns
| Pattern | pH | PaCO2 | HCO3- | Cause examples |
|---|---|---|---|---|
| Respiratory acidosis | ↓ | ↑ | Normal/↑ | COPD, hypoventilation, opioids |
| Respiratory alkalosis | ↑ | ↓ | Normal/↓ | Anxiety, PE, altitude, fever |
| Metabolic acidosis | ↓ | Normal/↓ | ↓ | DKA, lactic acidosis, renal failure |
| Metabolic alkalosis | ↑ | Normal/↑ | ↑ | Vomiting, diuretics, NG suctioning |
Sources: Current Surgical Therapy 14e; Barash, Cullen & Stoelting's Clinical Anesthesia 9e
If you have a specific ABG result you want interpreted, paste the values (pH, PaCO2, HCO3-, PaO2) and I'll walk through it with you!
Sodium correction
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Here is a complete guide to sodium correction, covering all three clinical contexts:
Sodium Correction
1. Corrected Sodium for Hyperglycemia (Pseudohyponatremia)
When blood glucose is elevated, glucose draws water out of cells into the ECF, which dilutes serum sodium - giving a falsely low reading.
Formula:
Corrected Na+ = Measured Na+ + 1.6 × [(Glucose - 100) / 100]
(Some sources use 2.4 mEq/L per 100 mg/dL for very high glucose >400 mg/dL)
Example:
- Measured Na+ = 126 mEq/L, Glucose = 1000 mg/dL
- Corrected Na+ = 126 + [0.016 × (1000 - 100)]
- Corrected Na+ = 126 + 14.4 = 140.4 mEq/L - normal!
- This is factitious (pseudohyponatremia) - treat the hyperglycemia, not the sodium
(Roberts & Hedges' Clinical Procedures in Emergency Medicine; Current Surgical Therapy 14e)
2. Hyponatremia - Safe Correction
Classification by severity
| Serum Na+ | Severity |
|---|---|
| 130 - 135 mEq/L | Mild |
| 125 - 129 mEq/L | Moderate |
| < 125 mEq/L | Severe |
Correction Rules (to prevent Osmotic Demyelination Syndrome - ODS)
| Situation | Target Rate |
|---|---|
| Symptomatic / acute (seizures, coma) | Bolus 100 mL of 3% NaCl IV over 10 min, repeat x2 as needed; goal +4 to +6 mEq/L urgently |
| Mild-moderate symptoms | 3% NaCl at 0.5 - 2 mL/kg/hour |
| Chronic asymptomatic | No more than 0.5 mEq/L/hour |
| Maximum in 24 hours | ≤ 8 mEq/L/day (high-risk patients); ≤ 12 mEq/L/day (general) |
| Chronic hyponatremia | Even slower: ≤ 6 mEq/24 hours |
Warning: Overcorrection leads to Osmotic Demyelination Syndrome (ODS / central pontine myelinolysis) - pseudobulbar palsy, ataxia, dysarthria, locked-in state, death. Risk factors: Na+ < 105 mEq/L, hypokalemia, alcoholism, malnutrition, liver disease.
If overcorrection occurs: Slow rate + give hypotonic fluids to bring Na+ back down + consider desmopressin (vasopressin analogue).
(Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Schwartz's Principles of Surgery 11e)
3. Hypernatremia - Free Water Deficit Calculation
Hypernatremia = free water deficit. Replace the deficit slowly.
Step 1 - Calculate Total Body Water (TBW):
- Men: TBW = 0.50 × lean body weight (kg)
- Women: TBW = 0.40 × lean body weight (kg)
Step 2 - Calculate Free Water Deficit:
Water deficit (L) = [(Serum Na+ - 140) / 140] × TBW
Example:
- 70 kg man, Na+ = 165 mEq/L
- TBW = 0.60 × 70 = 42 L
- Deficit = [(165 - 140) / 140] × 42 = 7.5 L
Step 3 - Replace slowly:
| Situation | Rate |
|---|---|
| Acute symptomatic hypernatremia | ≤ 1 mEq/L/hour; max 12 mEq/day |
| Chronic hypernatremia | Even slower: ≤ 0.7 mEq/L/hour |
Warning: Overly rapid correction of hypernatremia causes cerebral edema and herniation.
Fluids to use: 5% dextrose in water (D5W), D5W in quarter-normal saline, or oral/enteral water. In hypovolemic patients - restore volume with normal saline first, then correct the free water deficit.
(Schwartz's Principles of Surgery 11e; Roberts & Hedges' Emergency Medicine)
Quick Summary Table
| Scenario | Formula | Max Correction Rate |
|---|---|---|
| Pseudohyponatremia (hyperglycemia) | Na+ corrected = Na+ + 1.6 × [(Glu-100)/100] | Treat hyperglycemia |
| Hyponatremia correction | 3% NaCl titration | ≤ 8-12 mEq/L per 24h |
| Hypernatremia free water deficit | Deficit = [(Na+-140)/140] × TBW | ≤ 1 mEq/L/hour; ≤ 12 mEq/day |
Do you want to work through a specific patient case, or would you like details on SIADH management, choosing IV fluid types, or the sodium deficit formula for replacement?
This is a shared conversation. Sign in to Orris to start your own chat.