Management Guidelines Of Pneumonia ?
Reading File
Finding Sources
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND "management"[tiab]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have enough rich, detailed content from authoritative textbooks. Let me now compile the comprehensive answer.
Management Guidelines of Pneumonia
1. Classification
Pneumonia is categorized by acquisition setting, which drives the entire management pathway:
| Type | Definition |
|---|---|
| CAP (Community-Acquired) | Acquired outside hospital/healthcare settings |
| HAP (Hospital-Acquired) | Develops ≥48 hrs after admission |
| VAP (Ventilator-Associated) | Develops ≥48 hrs after endotracheal intubation |
| HCAP | Associated with recent healthcare contact (nursing home, dialysis, IV therapy) |
2. Initial Assessment and Severity Scoring
The first clinical priority is assessing severity to determine the site of care.
CURB-65 Score (bedside tool)
| Criterion | Points |
|---|---|
| C - Confusion (to person, place, or time) | 1 |
| U - Urea (BUN > 20 mg/dL) | 1 |
| R - Respiratory rate ≥ 30 breaths/min | 1 |
| B - Blood pressure: systolic <90 or diastolic ≤60 mmHg | 1 |
| 65 - Age ≥ 65 years | 1 |
- Score 0-1: Low risk → outpatient treatment
- Score 2: Moderate risk → consider inpatient
- Score ≥3: High risk → inpatient; consider ICU if ≥4-5
CURB-65 should guide but not replace clinical judgment. Among patients with the same CURB-65 score, mortality rates vary up to 26-fold depending on clinician assessment of need for admission. - Symptom to Diagnosis, 4th Ed.
Pneumonia Severity Index (PSI)
A more precise scoring system using age, sex, comorbidities, physical exam, and labs. PSI Classes I-III (≤90 points) support outpatient management; Classes IV-V indicate hospitalization. The PSI is preferred over CURB-65 when lab values are available. - Goldman-Cecil Medicine
3. ICU Admission Criteria (ATS/IDSA)
ICU admission is indicated if 1 major criterion OR ≥3 minor criteria are met:
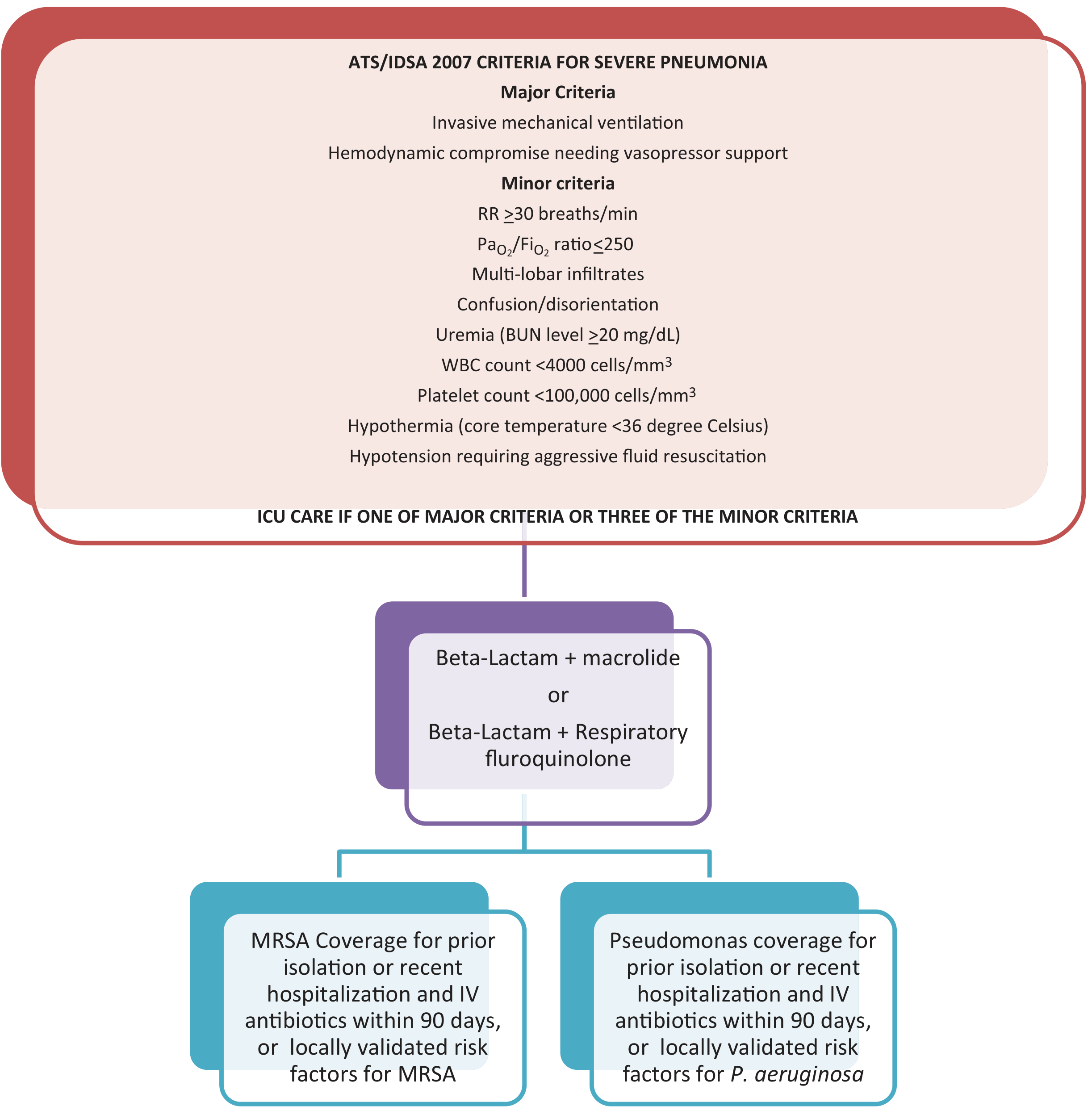
Major Criteria:
- Invasive mechanical ventilation required
- Septic shock requiring vasopressor support
Minor Criteria:
- RR ≥ 30 breaths/min
- PaO2/FiO2 ratio ≤ 250
- Multilobar infiltrates
- Confusion/disorientation
- Uremia (BUN ≥ 20 mg/dL)
- WBC < 4,000 cells/mm³
- Platelets < 100,000 cells/mm³
- Hypothermia (core temp < 36°C)
- Hypotension requiring aggressive fluid resuscitation
4. Investigations
All patients:
- Chest X-ray (confirm infiltrate)
- Pulse oximetry (SpO2 <95% is abnormal)
- COVID-19 PCR; influenza PCR (in season)
Hospitalized patients additionally:
- CBC, blood glucose, renal function (BMP/CMP)
- ABG if tachypneic
- Blood cultures x2 (before antibiotics, for severe/ICU cases)
- Sputum Gram stain + culture (if producing sputum)
- Urine Legionella antigen (severe CAP, outbreak setting)
- Urine pneumococcal antigen (severe CAP)
- Procalcitonin (aids bacterial vs. viral distinction; guides de-escalation)
Routine urine antigen testing is NOT recommended except in severe CAP or Legionella outbreaks. - Goldman-Cecil Medicine
5. Common Causative Pathogens
| Setting | Key Pathogens |
|---|---|
| Outpatient, healthy | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, respiratory viruses |
| Outpatient, comorbidities | Above + DRSP, enteric Gram-negatives, anaerobes (if aspiration) |
| Inpatient, non-ICU | S. pneumoniae (incl. DRSP), H. influenzae, atypicals, Legionella, enteric GNRs |
| Severe CAP (ICU) | S. pneumoniae, Legionella, enteric GNRs, S. aureus/MRSA, M. pneumoniae, viruses |
| Severe CAP + Pseudomonas risk | All above + P. aeruginosa |
Respiratory viruses account for 20-27% of all CAP cases. No pathogen is identified in 55-66% of cases. - Goldman-Cecil Medicine
6. Antibiotic Management by Site of Care
A. Outpatient (Mild CAP)
Previously healthy, no recent antibiotics:
- Amoxicillin monotherapy (preferred, newer 2026 ATS guideline)
- Doxycycline monotherapy
- Azithromycin or clarithromycin (macrolide) - only if local resistance <25%
With comorbidities (COPD, heart/liver/kidney disease, diabetes, asplenia, immunosuppression, antibiotic use in last 3 months):
- Respiratory fluoroquinolone alone: levofloxacin or moxifloxacin
- OR beta-lactam (amoxicillin-clavulanate, cefpodoxime, or cefuroxime) + macrolide or doxycycline
Duration: 5 days for uncomplicated outpatient CAP (per updated 2026 ATS guidelines)
B. Inpatient, Non-ICU (Moderate CAP)
No MRSA or Pseudomonas risk factors:
- Respiratory fluoroquinolone (levofloxacin or moxifloxacin) monotherapy
- OR beta-lactam (ceftriaxone, cefotaxime, ampicillin-sulbactam) + macrolide (azithromycin) or doxycycline
Newer non-inferior alternatives (especially when fluoroquinolones should be avoided):
- Omadacycline monotherapy
- Lefamulin monotherapy (contraindicated in prolonged QT or moderate/severe liver disease)
Avoid fluoroquinolones in: prolonged QT interval, history of C. difficile infection, tendinopathy risk, neurological concerns. - Goldman-Cecil Medicine
IV to oral switch: Clinically stable patients (T ≤37.8°C, HR <100, RR <24, SpO2 ≥90%, SBP ≥90, normal mental status) do NOT need 3 days of IV before switching to oral.
C. Severe CAP (ICU)
Dual therapy is mandatory - no monotherapy in ICU patients:
- Beta-lactam (ceftriaxone or cefotaxime) + macrolide (azithromycin)
- OR beta-lactam + respiratory fluoroquinolone (levofloxacin/moxifloxacin)
Add MRSA coverage (vancomycin or linezolid) if:
- Prior MRSA isolation from respiratory tract
- Recent hospitalization AND IV antibiotics within 90 days
- Locally validated epidemiologic risk factors
Add anti-Pseudomonal coverage (piperacillin-tazobactam, cefepime, or carbapenem) if:
- Prior P. aeruginosa isolation
- Recent hospitalization AND IV antibiotics within 90 days
- Structural lung disease (bronchiectasis)
- Corticosteroid therapy >10 mg/day
- Broad-spectrum antibiotics >7 days in past month
For CA-MRSA (necrotizing CAP post-influenza): linezolid alone or vancomycin + clindamycin (toxin inhibition). - Fishman's Pulmonary Diseases
7. De-escalation and Duration
- De-escalate antibiotics when cultures return and no MDR pathogen identified
- Standard duration: 5 days for non-severe CAP with clinical improvement
- Severe CAP or bacteremic cases: typically 7-10 days
- Legionella, MRSA, Pseudomonal CAP: 14-21 days may be needed
- Use procalcitonin to guide safe early discontinuation (supported by meta-analysis)
8. Supportive Care
| Intervention | Detail |
|---|---|
| Oxygen | Maintain SpO2 ≥94% (88-92% in COPD); high-flow nasal cannula or NIV for hypoxemia |
| Fluids | IV fluids for dehydration/hypotension; avoid fluid overload |
| Antipyretics/Analgesia | Paracetamol for fever and pleuritic pain |
| Nutrition | Early enteral nutrition in ICU patients |
| DVT prophylaxis | Subcutaneous LMWH for hospitalized patients |
| Early mobilization | Reduces complications, improves recovery |
| Mechanical ventilation | If respiratory failure (lung-protective strategy: tidal volume 6 mL/kg) |
9. Aspiration Pneumonia - Special Considerations
- Most episodes caused by Gram-negative organisms (not anaerobes, contra historical belief)
- Current IDSA/ATS guidelines do not recommend routine anaerobic coverage
- Treat with standard CAP regimens; add anaerobic coverage only if clear aspiration event with periodontal disease, lung abscess, or foul-smelling sputum
10. Complications to Monitor
| Complication | Frequency |
|---|---|
| Empyema | 3-5% of hospitalized cases |
| Acute cardiac events (AF, MI, HF) | ~20-25% of hospitalized patients |
| Respiratory failure | Variable (ICU cases) |
| Septic shock | Severe CAP |
| Parapneumonic effusion | Common |
11. Prevention
| Vaccine | Target |
|---|---|
| Pneumococcal vaccine (PCV15/PCV20 or PPSV23) | Adults ≥65, immunocompromised, chronic disease |
| Annual influenza vaccine | All adults; reduces post-influenza bacterial pneumonia |
| COVID-19 vaccine | All eligible adults |
| Smoking cessation | Major modifiable risk factor |
Recent Evidence (2024-2026)
The 2026 ATS Clinical Practice Guideline (PMID: 40679934) now supports beta-lactam monotherapy in low-risk outpatient CAP, departing from prior dual-therapy recommendations. A 2025 network meta-analysis (PMID: 40404065) confirmed no significant outcome difference between beta-lactam/macrolide vs. beta-lactam/fluoroquinolone combination strategies in hospitalized patients. A 2025 French guideline update (PMID: 40037948) also emphasizes antimicrobial stewardship to limit unnecessary broad-spectrum coverage.
Sources: Goldman-Cecil Medicine (International Edition) | Fishman's Pulmonary Diseases and Disorders | Symptom to Diagnosis, 4th Ed. | ATS/IDSA Guidelines (2019, 2026 update)
This is a shared conversation. Sign in to Orris to start your own chat.