Amphotericin b
Reading File
Finding Sources
Finding Sources
Searching PubMed
"amphotericin B" AND "liposomal"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Amphotericin B based on authoritative pharmacology textbooks (Katzung's Basic & Clinical Pharmacology 16th Ed. and Goodman & Gilman's Pharmacological Basis of Therapeutics):
Amphotericin B
Source & Chemistry
Amphotericin B is produced by the bacterium Streptomyces nodosus (along with the clinically unused Amphotericin A). It is an amphoteric polyene macrolide - "polyene" refers to its many conjugated double bonds (it is a heptaene, containing 7 trans-double bonds), and "macrolide" refers to its large lactone ring. The drug contains a mycosamine sugar (3-amino-3,6-dideoxymannose) attached via a glycosidic bond. It is nearly insoluble in water.
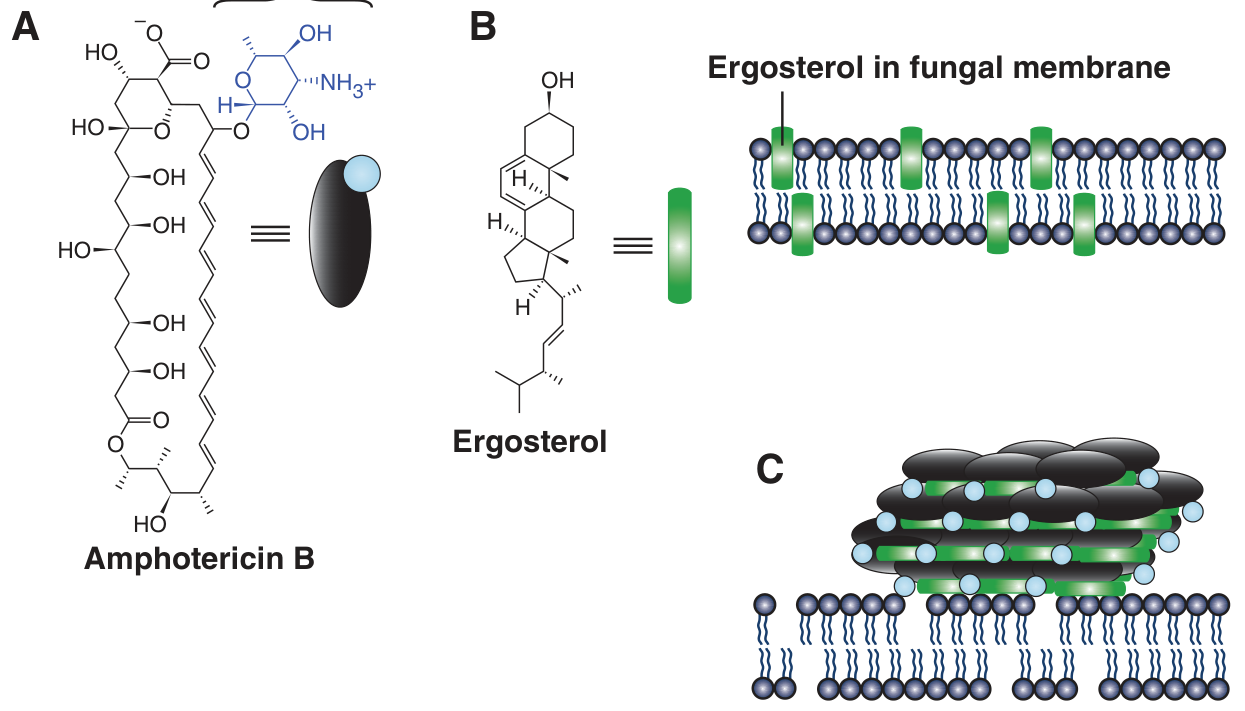
Mechanism of Action
Amphotericin B exploits the difference in membrane sterol composition between fungi and humans:
- Fungal membranes contain ergosterol
- Human/bacterial membranes contain cholesterol
The drug selectively binds ergosterol and:
- Classical view: Forms transmembrane pores/channels that allow leakage of intracellular ions and macromolecules, causing cell death
- Updated view (Goodman & Gilman): Recent evidence suggests it forms aggregates that sequester ergosterol from lipid bilayers, like a selective sponge, disrupting membrane integrity
Some binding to human cholesterol does occur, which accounts for the drug's significant toxicity.
Resistance occurs when ergosterol binding is impaired - either by decreasing membrane ergosterol concentration or by modifying the sterol target to reduce drug affinity. Intrinsically resistant organisms include Candida lusitaniae and Pseudallescheria boydii.
Formulations
| Formulation | Brand | Physical Form | Dose (mg/kg/d) | Nephrotoxicity | Infusional Toxicity |
|---|---|---|---|---|---|
| Conventional (C-AMB) + deoxycholate | Fungizone | Micelles | 0.5-1 | High | High |
| Liposomal (L-AMB) | AmBisome | Spheres | 3-5 | Reduced | Reduced |
| Lipid complex (ABLC) | Abelcet | Ribbons | 5 | Reduced | Reduced |
| Colloidal dispersion (ABCD) | Amphotec | Disks | 5 | Reduced | Increased |
Why lipid formulations? Amphotericin binds to the lipid vehicle with affinity between that for fungal ergosterol and human cholesterol. The lipid acts as a reservoir, reducing nonspecific binding to human membranes. Some fungi also have lipases that liberate free amphotericin directly at the infection site.
Pharmacokinetics of conventional formulation:
- IV dosing 0.5-1 mg/kg/d achieves blood levels of 0.3-1 mcg/mL
-
90% protein-bound
- Half-life ~15 days
- Widely distributed in most tissues
- Only 2-3% penetrates CSF (may require intrathecal therapy for some fungal meningitides)
- No dose adjustment needed for renal or hepatic impairment; dialysis has little impact
Antifungal Spectrum (Broadest of All Antifungals)
- Yeasts: Candida albicans, C. tropicalis, Cryptococcus neoformans
- Endemic mycoses: Histoplasma capsulatum, Blastomyces dermatitidis, Coccidioides immitis
- Molds: Aspergillus fumigatus, agents of mucormycosis
- Resistant organisms: Candida lusitaniae, Pseudallescheria boydii
Clinical Uses
- First-line induction therapy for nearly all life-threatening systemic mycoses
- Used as initial induction to rapidly reduce fungal burden, then switched to an azole for chronic/maintenance therapy
- Especially important in immunosuppressed patients - severe cryptococcal meningitis, disseminated histoplasmosis, coccidioidomycosis, invasive aspergillosis
- Cryptococcal meningitis: AmB + flucytosine (synergy via enhanced flucytosine penetration through damaged fungal membranes)
- Mucormycosis: AmB is the drug of choice (azoles are largely ineffective)
- Visceral leishmaniasis: Liposomal AmB is the preferred treatment in India (where resistance to stibogluconate is high); a single IV dose of 10 mg/kg has been used
- Local uses: Bladder irrigation for Candida UTIs, topical drops for fungal keratitis/corneal ulcers, intra-articular injection for fungal arthritis
- Intrathecal (cisterna magna, lumbar, lateral ventricle) for Coccidioidal meningitis unresponsive to other agents
Adverse Effects
1. Infusion-Related (Acute) Reactions
Nearly universal with conventional AmB. Mediated via TLR2 and CD14 signaling:
- Fever, chills, muscle spasms, vomiting, headache, hypotension, tachypnea
- Frank anaphylaxis and bronchospasm are rare
- Reactions end spontaneously in 30-45 minutes
Management:
- Slow infusion rate or reduce daily dose
- Premedicate with antipyretics (acetaminophen/ibuprofen), antihistamines, meperidine (shortens fever duration), or IV hydrocortisone 0.7 mg/kg
- Test dose of 1 mg IV before first infusion to gauge reaction severity
- Febrile reactions tend to lessen with subsequent infusions
2. Cumulative (Chronic) Toxicity
| Toxicity | Details |
|---|---|
| Nephrotoxicity | Azotemia occurs in ~80% of patients on C-AMB. Dose-dependent, usually transient; worsened by concurrent aminoglycosides or cyclosporine. Permanent tubular histological changes can occur |
| Hypokalemia/Hypomagnesemia | From renal tubular wasting; requires supplementation |
| Anemia | Normochromic, normocytic; due to reduced erythropoietin production from damaged renal tubular cells |
| Liver toxicity | Occasional elevation of liver function tests |
| Intrathecal | Seizures and chemical arachnoiditis with serious neurologic sequelae |
Lipid formulations are significantly less nephrotoxic than C-AMB.
Synergy with Flucytosine
Amphotericin B + flucytosine is a classic synergistic combination for cryptococcal meningitis. The mechanism: AmB damages the fungal membrane, enhancing penetration of flucytosine into fungal cells. Note that flucytosine must not be used as monotherapy because resistance develops rapidly.
Key Points to Remember
- Produced by Streptomyces nodosus
- Polyene macrolide; heptaene (7 double bonds)
- Target: ergosterol in fungal cell membrane
- Broadest spectrum antifungal available
- C-AMB is nephrotoxic in ~80% of patients; lipid formulations dramatically reduce this
- CSF penetration is poor (2-3%) - may need intrathecal dosing
- Half-life ~15 days; no dose adjustment for renal/hepatic impairment
- Drug of choice for mucormycosis and severe endemic mycoses
- "Gold standard" induction agent before azole step-down therapy
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1330-1332
- Goodman & Gilman's Pharmacological Basis of Therapeutics, pp. 1213-1216
Recent Evidence Update: A 2024 systematic review and meta-analysis on high-dose liposomal AmB (PMID 37971463) confirmed its safety and effectiveness profile, and a 2025 systematic review on liposomal AmB prophylaxis in pediatrics (PMID 40493030) supports its use in immunocompromised children - both consistent with current textbook guidance.
This is a shared conversation. Sign in to Orris to start your own chat.