Explain each and everything about Spinal Cord and Ascending, Descending, and lntersegmental Tracts. I want even the minor details about the topic. Also explain all the clinicals along the content
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Here is a complete, detailed reference on the Spinal Cord and all its tracts, drawn from Gray's Anatomy for Students, Neuroanatomy through Clinical Cases, Localization in Clinical Neurology, Medical Physiology (Guyton & Hall), Harrison's Principles, Campbell's Operative Orthopaedics, and Goldman-Cecil Medicine.
The Spinal Cord: Complete Reference
1. OVERVIEW AND BASIC STRUCTURE
The spinal cord is a thin, tubular extension of the central nervous system (CNS) contained within the bony spinal canal. It originates at the medulla oblongata (level of the foramen magnum) and continues caudally, terminating as the conus medullaris at approximately the L1-L2 vertebral level in adults (L3 in neonates). From the conus, a fibrous cord called the filum terminale connects the spinal cord to the dorsum of the first coccygeal segment. The adult spinal cord is approximately 46 cm long.
The spinal cord is enclosed in three protective membranes - the pia, arachnoid, and dura mater - which are continuous with the cranial meninges:
- Pia mater: innermost, highly vascular, adherent directly to cord surface. Forms the denticulate ligament midway between anterior and posterior roots, which anchors the cord within the subarachnoid space.
- Arachnoid mater: middle layer; creates the subarachnoid space (filled with CSF) between itself and the pia. This space extends to S2 level, below the cord - the basis for safe lumbar puncture.
- Dura mater: outermost tough fibrous layer.
31 pairs of spinal nerves emerge from the cord. There are 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal pairs. Key point: there are 8 cervical segments but only 7 cervical vertebrae, so C1-C7 nerves exit above their corresponding vertebra; C8 exits below C7. All subsequent nerves exit below their corresponding vertebra.
- Gray's Anatomy for Students
- Harrison's Principles of Internal Medicine 22E
2. EXTERNAL FEATURES
The spinal cord has several longitudinal fissures and sulci on its surface:
- Anterior median fissure: deep midline groove on the anterior surface. The anterior spinal artery runs here.
- Posterior median sulcus: shallower midline groove on the posterior surface.
- Posterolateral sulci (bilateral): where posterior (dorsal) root fibers enter.
- Anterior rootlets emerge in a line lateral to the anterior median fissure.
Two enlargements accommodate neurons for the limbs:
- Cervical enlargement (C5-T1): for brachial plexus / upper extremities
- Lumbar (lumbosacral) enlargement (L2-S3): for lumbar plexus / lower extremities
Below the lumbosacral enlargement, the cord tapers as the conus medullaris. Below that, the remaining lumbar and sacral nerve roots form the cauda equina ("horse's tail"), which floats freely within the subarachnoid space before exiting at their respective foramina.
- Gray's Anatomy for Students
3. INTERNAL FEATURES - CROSS-SECTIONAL ANATOMY
3A. Gray Matter
A cross-section of the spinal cord reveals centrally-placed gray matter surrounded by white matter. The gray matter is butterfly-shaped (or H-shaped), with two lateral columns joined by a transverse gray commissure. It is divided into:
Dorsal (posterior) horn: involved mainly in sensory processing.
Intermediate zone: contains interneurons and autonomic nuclei.
Ventral (anterior) horn: contains motor neurons (alpha and gamma).
There is also an intermediolateral gray column from T1-L2 - the source of preganglionic sympathetic fibers. Sacral segments S2-S4 contain a similar column for parasympathetic outflow.
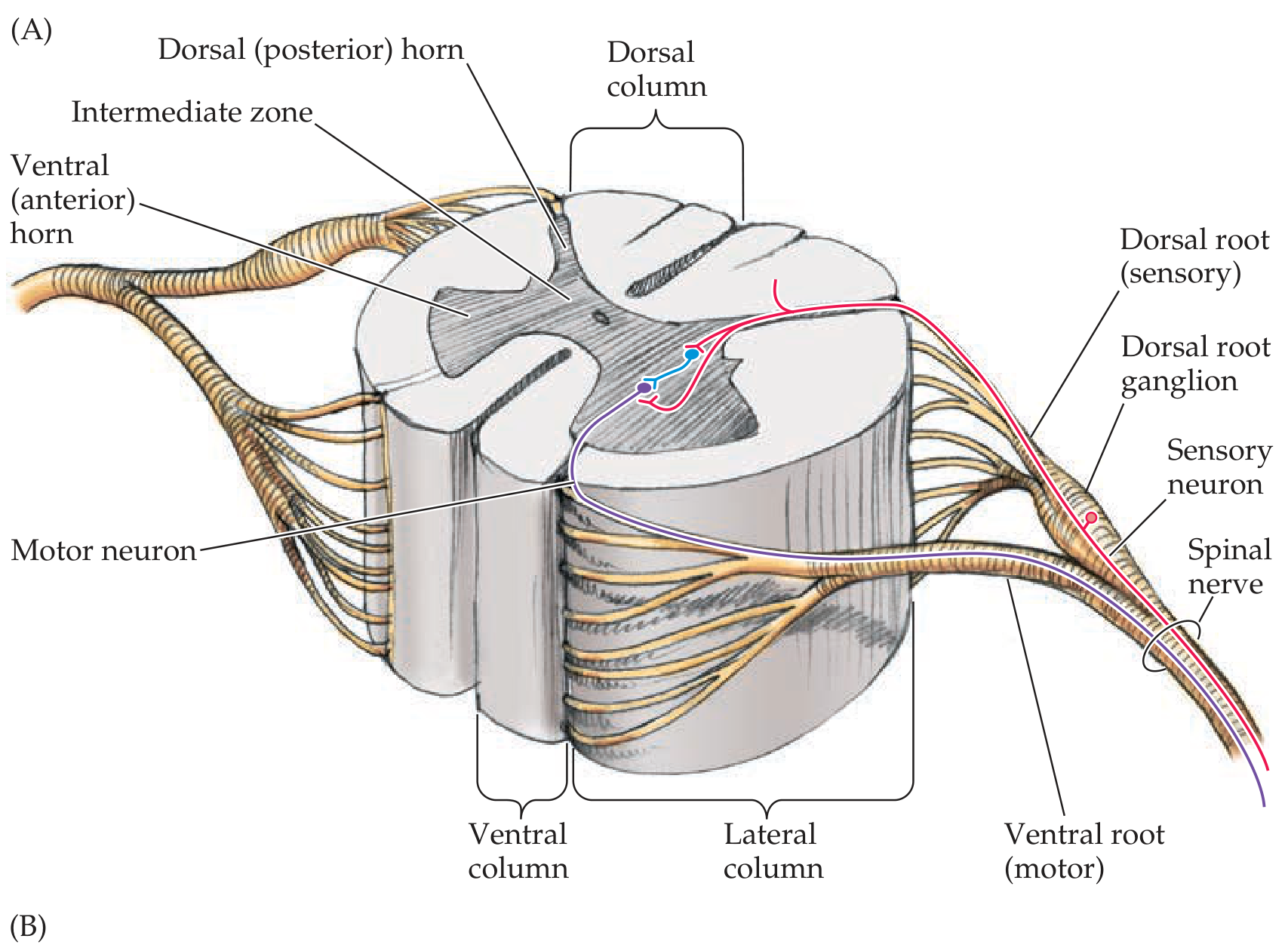
Spinal cord - gray matter, white matter, dorsal and ventral root organization. - Neuroanatomy through Clinical Cases 3rd Ed
3B. Rexed's Laminae (Cytoarchitecture)
The Swedish anatomist Bror Rexed described 10 cell layers within the gray matter:
| Lamina | Region | Key Nuclei/Function |
|---|---|---|
| I | Dorsal horn (tip) | Nucleus posteromarginalis (posterior marginal nucleus) - pain/temperature |
| II | Dorsal horn | Substantia gelatinosa of Rolando - pain modulation |
| III & IV | Dorsal horn | Nucleus proprius dorsalis - sensory processing |
| V | Dorsal horn (neck) | Nucleus reticularis - receives spinoreticular input |
| VI | Base of dorsal horn | Proprioception from muscle spindles |
| VII | Intermediate zone | Nucleus dorsalis of Clarke (C8-L3) - spinocerebellar relay; autonomic neurons |
| VIII | Ventral horn (medial) | Interneurons, commissural neurons |
| IX | Ventral horn | Alpha and gamma motor neurons (extrafusal and intrafusal muscle fibers) |
| X | Central canal zone | Gray commissure (dorsal and ventral) |
Alpha motor neurons (large): innervate extrafusal skeletal muscle fibers.
Gamma motor neurons (small): innervate intrafusal muscle fibers of muscle spindles, regulating spindle sensitivity.
Renshaw cells: inhibitory interneurons in the anterior horn; receive collaterals from alpha motor neuron axons and provide lateral inhibition to adjacent motor neurons, sharpening motor output.
- Neuroanatomy through Clinical Cases 3rd Ed
- Localization in Clinical Neurology 8e
3C. White Matter - Funiculi
Each half of the spinal cord white matter is divided into three funiculi (columns):
- Dorsal (posterior) funiculus: between dorsomedian and dorsolateral sulci - contains dorsal column tracts
- Lateral funiculus: between dorsolateral and ventrolateral sulci - contains spinocerebellar tracts, spinothalamic tract, corticospinal tract
- Ventral (anterior) funiculus: between ventrolateral sulcus and anterior median fissure - contains anterior corticospinal tract, vestibulospinal, reticulospinal tracts
Dorsal and ventral white commissures run alongside the corresponding gray commissures and allow decussation of fibers between sides.
The white matter is thickest at cervical levels (where most ascending fibers have entered and most descending fibers have not yet terminated) and thinnest at sacral levels (mostly gray matter).
- Localization in Clinical Neurology 8e
- Neuroanatomy through Clinical Cases 3rd Ed
4. ASCENDING TRACTS (Sensory Pathways)
All ascending tracts transmit sensory information from the periphery to higher centers. They are classic 3-neuron pathways for conscious perception.
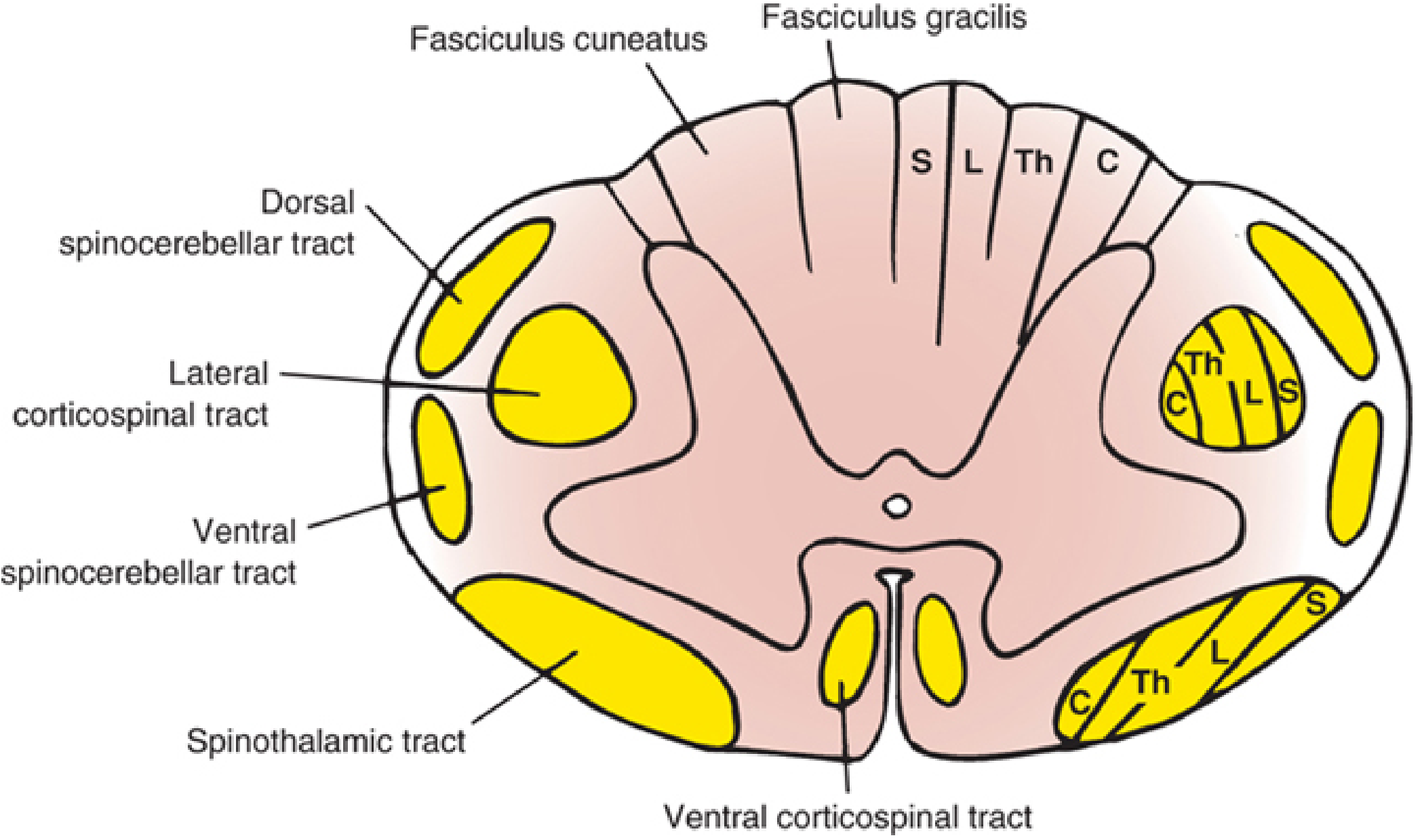
Cross-sectional anatomy showing tract lamination: S=sacral, L=lumbar, Th=thoracic, C=cervical. - Localization in Clinical Neurology 8e
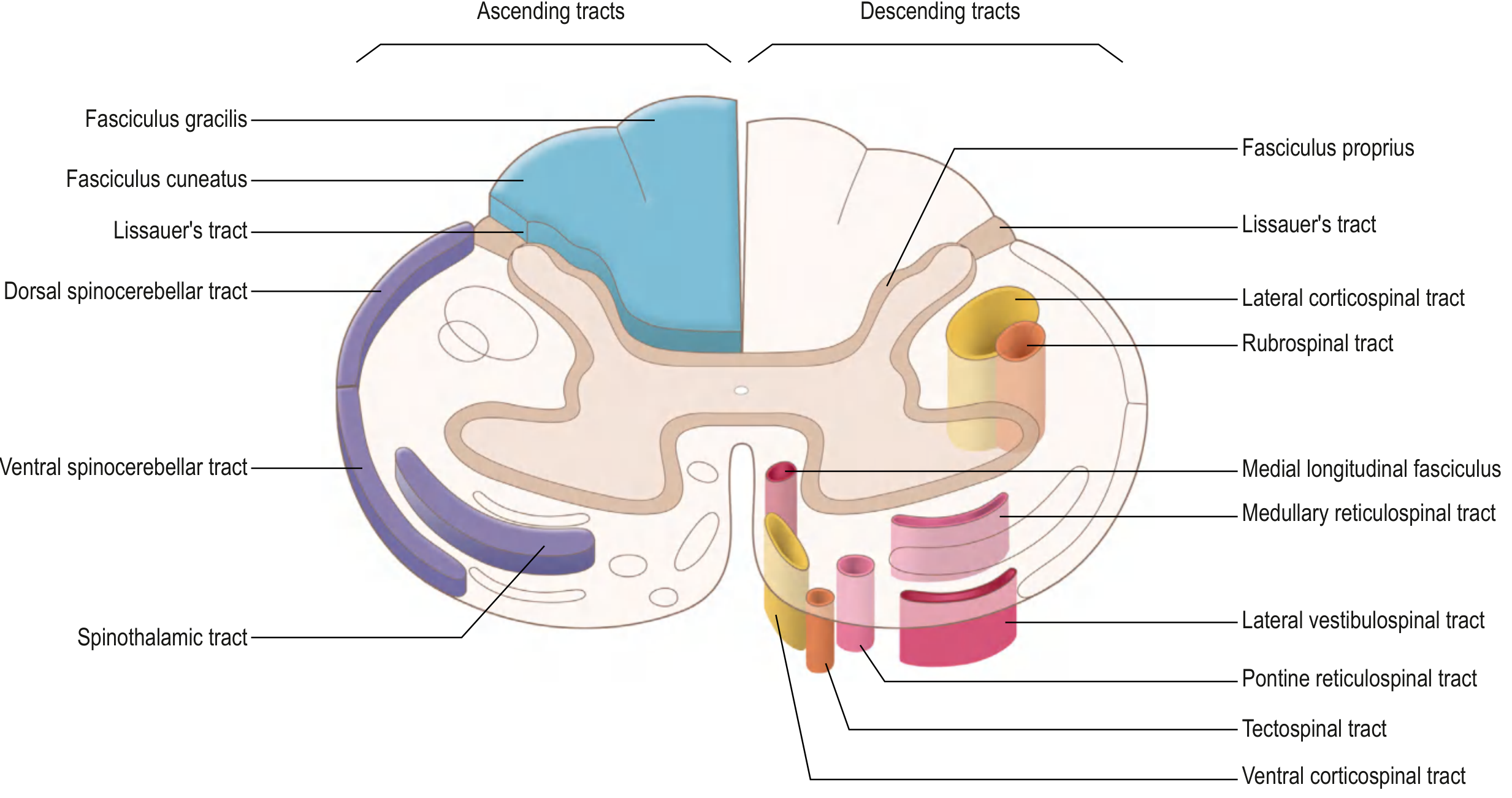
All ascending tracts (left) and descending tracts (right) in a spinal cord cross-section. - Gray's Anatomy for Students
4A. ANTEROLATERAL SYSTEM (Spinothalamic + Related Tracts)
This system carries pain, temperature, and crude/light touch. It is composed of three tracts:
4A-1. Lateral Spinothalamic Tract (Neospinothalamic Tract)
Modalities: Sharp, localized pain; temperature
Pathway (3 neurons):
- 1st-order neuron: Cell body in the dorsal root ganglion (DRG). Axon enters the spinal cord via the posterior root, splits into the zone of Lissauer (posterolateral tract of Lissauer) - ascending or descending 1-2 segments before synapsing.
- Synapse: On 2nd-order neurons in laminae I and V of the dorsal horn.
- 2nd-order neuron: Axons cross obliquely within the anterior commissure, traveling over 2-3 segments before joining the anterolateral tract on the contralateral side. They then ascend to the ventral posterolateral (VPL) nucleus of the thalamus.
- 3rd-order neuron: From VPL, fibers pass through the posterior limb of the internal capsule to reach the primary somatosensory cortex (postcentral gyrus, areas 3, 1, 2).
Laminar arrangement (somatotopy): In the lateral spinothalamic tract, fibers from cervical segments are situated dorsomedially, and sacral fibers are ventrolaterally (C-Th-L-S from inside out). There is also a segregation between pain and temperature fibers within the tract.
Clinical significance: Lesions of the anterior commissure (e.g., syringomyelia) interrupt crossing fibers, producing a cape-like bilateral loss of pain and temperature at the affected segments while sparing touch and proprioception (dissociated sensory loss).
4A-2. Spinoreticular Tract (Paleospinothalamic System)
Modalities: Poorly localized, burning, chronic pain; emotional/arousal aspects of pain
Pathway: Similar 1st-order neuron. 2nd-order axons project to the reticular formation of the brainstem instead of the thalamus. From the reticular formation, signals go to the intralaminar nuclei of the thalamus, then diffusely to the cortex.
Key point: This system is responsible for the suffering and autonomic component of pain. It projects to the limbic system, explaining why pain has emotional dimensions.
4A-3. Spinomesencephalic Tract
Pathway: 2nd-order axons project to the periaqueductal gray (PAG) and superior colliculi in the midbrain.
Function: Central modulation/inhibition of pain. The PAG is the main center for endogenous opioid-mediated pain suppression. Stimulation here causes profound analgesia.
4A-4. Anterior (Ventral) Spinothalamic Tract
Modality: Light touch (crude touch)
Pathway: Similar to lateral spinothalamic - 2nd-order axons cross through the ventral white commissure and ascend as the ventral spinothalamic tract to the VPL thalamus.
Note: Light touch is also carried by the dorsal column-medial lemniscal pathway, so isolated damage to the ventral spinothalamic tract does not completely abolish light touch.
4B. POSTERIOR COLUMN - MEDIAL LEMNISCAL PATHWAY (Dorsal Column System)
Modalities: Fine/discriminative touch, two-point discrimination, vibration sense, conscious proprioception (joint position sense), stereognosis, graphesthesia.
Pathway (3 neurons):
- 1st-order neuron: Cell body in the DRG. Heavily myelinated axons (fast conduction) enter through the medial bundle of the dorsal root. They pass ipsilaterally into the dorsal funiculus and ascend without synapsing all the way to the caudal medulla.
- Fibers from the lower body (sacral, lumbar, lower 6 thoracic levels) enter medially and form the fasciculus gracilis (Goll's column) - carries lower limb and trunk sensation
- Fibers from the upper body (upper 6 thoracic + all cervical levels) add laterally to form the fasciculus cuneatus (Burdach's column) - carries upper limb and neck sensation
- Synapse: In the caudal medulla at the nucleus gracilis (for gracilis) and nucleus cuneatus (for cuneatus)
- 2nd-order neuron: Axons from these nuclei cross the midline as internal arcuate fibers (medial lemniscal decussation), forming the medial lemniscus, which ascends through the brainstem to the VPL nucleus of the thalamus.
- 3rd-order neuron: VPL nucleus projects via the posterior limb of the internal capsule to the primary somatosensory cortex.
Somatotopy in dorsal columns: As fibers accumulate from below, sacral fibers are most medial, then lumbar, then thoracic, and cervical fibers are most lateral. This is the opposite of the spinothalamic tract arrangement.
Clinical significance: Damage to dorsal columns causes:
- Loss of vibration and proprioception ipsilaterally below the lesion
- Positive Romberg sign (patient falls when eyes closed due to loss of proprioceptive input)
- Sensory ataxia: unsteady gait, worse in the dark
- Subacute combined degeneration (Vitamin B12 deficiency) causes demyelination of dorsal columns + lateral corticospinal tracts
- Tabes dorsalis (tertiary syphilis): selective degeneration of dorsal columns and dorsal roots
4C. SPINOCEREBELLAR TRACTS (Subconscious Proprioception)
These carry proprioceptive and kinesthetic information to the cerebellum for subconscious coordination - not for conscious perception.
4C-1. Dorsal (Posterior) Spinocerebellar Tract
Origin: Clarke's nucleus (nucleus dorsalis, lamina VII), present only at C8-L3
Course: Axons enter the lateral funiculus ipsilaterally and ascend to enter the cerebellum via the inferior cerebellar peduncle
Function: Carries proprioceptive signals from muscle spindles and Golgi tendon organs of the ipsilateral lower limb and trunk
4C-2. Ventral (Anterior) Spinocerebellar Tract
Origin: Laminae V-VII (border cells), thoracolumbar cord
Course: Axons cross to the contralateral lateral funiculus and ascend to enter the cerebellum via the superior cerebellar peduncle. Many fibers then recross within the cerebellum, so the final information is largely ipsilateral.
Function: Monitors spinal cord interneuron activity and provides the cerebellum with information about the state of motor activity (efference copy/internal feedback)
4C-3. Cuneocerebellar Tract
Origin: Accessory (external) cuneate nucleus in medulla
Function: Carries proprioception from upper limb to cerebellum (analogous to dorsal spinocerebellar tract for lower limb). Since Clarke's nucleus only extends to C8, upper limb proprioception cannot use the dorsal spinocerebellar tract directly.
5. DESCENDING TRACTS (Motor Pathways)
Descending tracts are involved in voluntary movements, postural control, and coordination of head, neck, and eye movements. They originate in the cerebral cortex and brainstem and are organized into lateral and medial motor systems.
Each descending pathway has two neurons:
- Upper motor neuron (UMN): cell body in cortex or brainstem
- Lower motor neuron (LMN): cell body in anterior horn of spinal cord
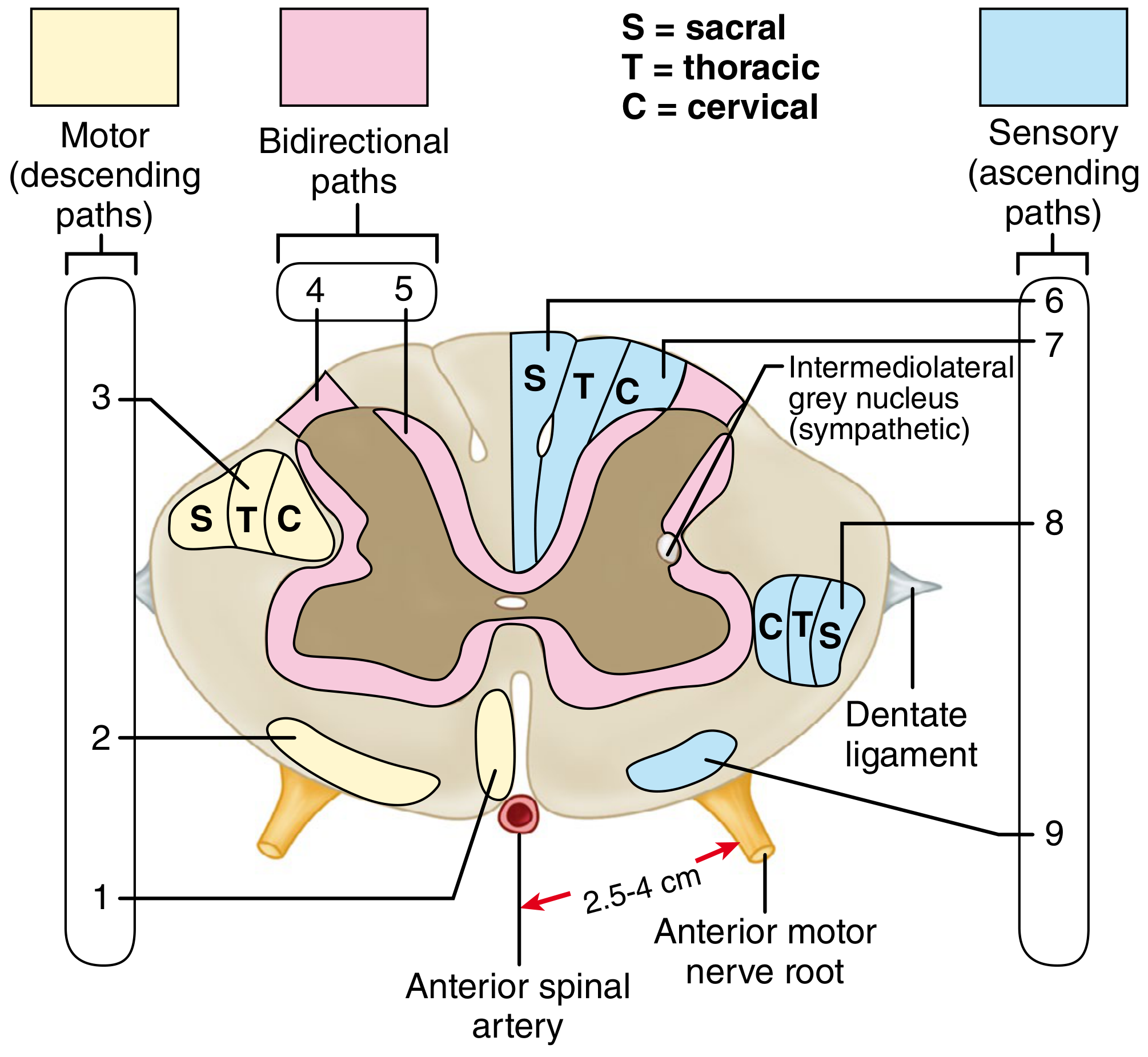
Schematic cross section of the cervical spinal cord showing numbered ascending and descending tracts with somatotopic lamination. - Campbell's Operative Orthopaedics 15th Ed
5A. LATERAL MOTOR SYSTEM
Controls distal limb muscles (fine, skilled movements). Tracts are located in the lateral column and synapse on lateral anterior horn cells.
5A-1. Lateral Corticospinal Tract (Pyramidal Tract)
This is the most clinically important motor tract.
Origin: Primary motor cortex (precentral gyrus, Brodmann area 4), supplementary motor area, premotor cortex.
Course:
- Axons converge in the corona radiata → descend through the posterior limb of the internal capsule
- → form the crus cerebri in the midbrain
- → pass through the anterior pons as small bundles (scattered by transverse pontocerebellar fibers)
- → regroup at the medulla to form the pyramids (the large swellings on the anterior medullary surface - hence "pyramidal tract")
- → at the caudal medulla: ~85-90% of fibers decussate at the pyramidal decussation (cervicomedullary junction) to form the lateral corticospinal tract in the contralateral lateral column
- → descend through the entire spinal cord, synapsing on lower motor neurons in the lateral anterior horn at all levels
Somatotopy: Cervical (arm) fibers are central (medial); thoracic, lumbar, sacral fibers are progressively peripheral (lateral). This explains central cord syndrome.
Function: Voluntary, skilled, fractionated movements of the contralateral limbs (especially fine finger movements).
Termination: Primarily at cervical and lumbosacral enlargements, on LMN cell bodies and interneurons.
5A-2. Rubrospinal Tract
Origin: Red nucleus (magnocellular division), midbrain tegmentum
Decussation: Ventral tegmental decussation in the midbrain (immediately after leaving the nucleus)
Course: Descends in the lateral column of the spinal cord, parallel and anterior to the lateral corticospinal tract
Termination: Only to cervical cord levels, on interneurons in the lateral anterior horn
Function: Facilitates flexor muscle activity and inhibits extensor activity of the upper limb. In humans, its function is considered uncertain / largely redundant with the lateral corticospinal tract.
5B. MEDIAL MOTOR SYSTEM
Controls axial and proximal muscles (posture, balance, automatic gait). Tracts are in the anterior and medial columns and project bilaterally on interneurons, making individual tract testing difficult clinically.
5B-1. Anterior (Ventral) Corticospinal Tract
Origin: Primary motor cortex + supplementary motor area (the ~10-15% of fibers that did NOT decussate at the pyramidal decussation)
Course: Descends ipsilaterally in the medial aspect of the anterior column
Termination: Cervical and upper thoracic cord. Most fibers eventually cross at the segmental level via the anterior white commissure before terminating on LMNs in the medial anterior horn.
Function: Control of bilateral axial and girdle muscles (trunk, neck). This bilateral control explains why axial movements (trunk, neck) are much less affected by unilateral cortical lesions.
5B-2. Vestibulospinal Tracts
Two separate tracts arise from different vestibular nuclei:
Lateral Vestibulospinal Tract:
- Origin: Lateral (Deiters') vestibular nucleus in the pons/medulla (receives input from cerebellum and inner ear)
- Course: Descends ipsilaterally through the entire length of the spinal cord in the anterior column
- Function: Facilitates extensor/antigravity muscle tone (ipsilateral), inhibits flexors. Critical for maintaining balance and upright posture in response to vestibular signals.
Medial Vestibulospinal Tract:
- Origin: Medial and inferior vestibular nuclei
- Course: Descends bilaterally only to cervical and upper thoracic cord, within the medial longitudinal fasciculus (MLF)
- Function: Positioning of the head and neck in response to vestibular input
Example: When you trip and your head jerks forward, vestibulospinal activation extends the upper limb to break the fall.
5B-3. Reticulospinal Tracts
Two components arise from the reticular formation:
Pontine (medial) Reticulospinal Tract:
- Origin: Pontine reticular formation (nucleus reticularis pontis caudalis/oralis)
- Course: Descends ipsilaterally in the anterior column
- Function: Facilitates extensor motor neurons, facilitates voluntary movements
Medullary (lateral) Reticulospinal Tract:
- Origin: Medullary reticular formation (nucleus reticularis gigantocellularis)
- Course: Descends ipsilaterally (mostly) in the anterior/lateral column
- Function: Inhibits extensor motor neurons; regulates voluntary movement, reflex activity, and autonomic outflow
Together, these tracts regulate automatic postural and gait-related movements and modulate spinal reflexes. They also carry descending autonomic commands to sympathetic and parasympathetic preganglionic neurons.
5B-4. Tectospinal Tract
Origin: Superior colliculus (dorsal midbrain) - a visual processing center
Decussation: Dorsal tegmental decussation (immediately crosses in the midbrain)
Course: Descends near the anterior median fissure through brainstem, then into cervical cord only
Termination: Interneurons in the anterior horn of cervical cord, bilaterally
Function: Reflex postural movements in response to visual stimuli (orienting movements of the head and eyes toward visual targets). Function in humans is considered uncertain.
6. SUMMARY TABLE OF ALL TRACTS
| # | Tract | Column | Function | Decussation | Laterality at Cord |
|---|---|---|---|---|---|
| ASCENDING | |||||
| 1 | Lateral spinothalamic | Lateral | Pain, temperature | Anterior commissure (2-3 segs above) | Contralateral |
| 2 | Anterior spinothalamic | Anterior | Light touch (crude) | Anterior commissure | Contralateral |
| 3 | Spinoreticular | Lateral | Arousal/affective pain | Anterior commissure | Bilateral |
| 4 | Spinomesencephalic | Lateral | Pain modulation (PAG) | Anterior commissure | Contralateral |
| 5 | Fasciculus gracilis | Posterior | Proprioception/vibration/fine touch (lower body) | Internal arcuate fibers (medulla) | Ipsilateral |
| 6 | Fasciculus cuneatus | Posterior | Proprioception/vibration/fine touch (upper body) | Internal arcuate fibers (medulla) | Ipsilateral |
| 7 | Dorsal spinocerebellar | Lateral | Subconscious proprioception (lower limb) | None (ipsilateral) | Ipsilateral |
| 8 | Ventral spinocerebellar | Lateral | Spinal cord motor state (recrosses in cerebellum) | Crosses twice | Ipsilateral net |
| DESCENDING | |||||
| 9 | Lateral corticospinal | Lateral | Voluntary skilled movement (contralateral limbs) | Pyramidal decussation (medulla) | Contralateral |
| 10 | Anterior corticospinal | Anterior | Bilateral axial/girdle motor | Segmental (at termination) | Bilateral |
| 11 | Rubrospinal | Lateral | Flexor facilitation of upper limb | Ventral tegmental dec. (midbrain) | Contralateral |
| 12 | Lateral vestibulospinal | Anterior | Extensor tone, balance | None | Ipsilateral |
| 13 | Medial vestibulospinal | Anterior | Head/neck positioning | None (bilateral) | Bilateral |
| 14 | Pontine reticulospinal | Anterior | Extensor facilitation, posture | None | Ipsilateral |
| 15 | Medullary reticulospinal | Lateral/Anterior | Extensor inhibition, autonomic | None | Ipsilateral |
| 16 | Tectospinal | Anterior | Visual-motor reflex (head/eye orient.) | Dorsal tegmental dec. (midbrain) | Contralateral |
7. INTERSEGMENTAL TRACTS (Propriospinal Fibers)
Fasciculus Proprius (Propriospinal System):
The intersegmental tracts - also called propriospinal fibers or the fasciculus proprius - are a collar of white matter that immediately surrounds the gray matter on all sides. They are one of the most important yet under-appreciated components of the spinal cord.
Key facts:
- More than half of all the nerve fibers that ascend and descend in the spinal cord are propriospinal fibers (Guyton & Hall).
- These fibers run from one segment of the cord to another - they do NOT project to the brain.
- When sensory fibers enter the cord via the posterior roots, they bifurcate and send branches both up and down the cord - some travel only 1-2 segments, others many segments.
- They are present in all three funiculi (posterior, lateral, and anterior) immediately adjacent to the gray matter.
Functions:
- Multisegmental reflexes: Propriospinal fibers coordinate reflexes that involve multiple cord segments simultaneously - for example, coordinating simultaneous movements of the forelimbs and hindlimbs during locomotion.
- Long propriospinal neurons (C3-C4): A specific group of propriospinal neurons at C3-C4 segments mediate part of the corticospinal command for upper limb movements. Corticospinal fibers synapse on C3-C4 propriospinal neurons, which then relay commands to cervical motor neurons.
- Interlimb coordination: Coordinate bilateral limb movements (e.g., the stepping reflex involves intersegmental communication via propriospinal fibers).
- Provide short-loop feedback within the cord for segmental reflexes.
- Bidirectional pathways - the fasciculus proprius has both ascending and descending fibers.
Lissauer's Tract (Posterolateral Tract / Zone of Lissauer):
-
Located at the tip of the posterior horn, between the dorsal gray column and the cord surface
-
Contains both ascending and descending fibers
-
Carries finely myelinated (Aδ) and unmyelinated (C) fibers for pain and temperature
-
Allows 1st-order pain afferents to travel up or down 1-2 segments before synapsing, enabling a wider zone of input convergence
-
The zone of Lissauer separates the dorsal gray column from the cord surface
-
Guyton and Hall Textbook of Medical Physiology
-
Gray's Anatomy for Students
-
Eric Kandel - Principles of Neural Science 6th Ed
8. VASCULAR SUPPLY
Three main longitudinal vessels supply the spinal cord:
Anterior Spinal Artery (ASA):
- Formed by union of two branches from the vertebral arteries within the cranial cavity
- Runs in the anterior median fissure throughout the cord's length
- Sulcal (central) branches supply the anterior horn, lateral horn, central gray, and anterior 2/3 of the cord (including the lateral corticospinal tract and spinothalamic tracts)
- Reinforced at the lower thoracic/upper lumbar level by the Artery of Adamkiewicz (great radicular artery of Adamkiewicz) - usually on the left side, enters between T9-L2. Its occlusion can cause catastrophic anterior spinal cord infarction.
Posterior Spinal Arteries (PSA) (paired):
- Branches of vertebral arteries or PICA
- Run along posterolateral sulci
- Supply dorsal horns and dorsal funiculi (posterior 1/3 of cord)
Segmental/Radiculomedullary Arteries: 6-10 reinforce the ASA; 10-23 reinforce the PSA. The largest is the Artery of Adamkiewicz.
Vulnerable Zone: The midthoracic region (T3-T8) is the most poorly vascularized area, making it most susceptible to ischemia.
- Gray's Anatomy for Students
- Localization in Clinical Neurology 8e
9. CLINICAL CORRELATES
9A. Upper Motor Neuron (UMN) vs. Lower Motor Neuron (LMN) Lesions
| Feature | UMN Lesion (above anterior horn) | LMN Lesion (anterior horn or below) |
|---|---|---|
| Weakness | Spastic (increased tone) | Flaccid (decreased tone) |
| Reflexes | Hyperreflexia, Babinski sign (+) | Hyporeflexia / areflexia |
| Atrophy | Disuse atrophy (late, mild) | Rapid, severe muscle atrophy |
| Fasciculations | Absent | Present |
9B. Spinal Cord Injury Syndromes
Complete Cord Transection
- Loss of ALL motor, sensory, and autonomic function below the level of the lesion
- Initially: Spinal shock - flaccid paralysis, absent reflexes, urinary retention, hypotension
- After weeks: Spasticity, hyperreflexia, autonomic dysreflexia
Brown-Séquard Syndrome (Cord Hemisection)
- Cause: Penetrating trauma (stab wound), tumor, demyelinating lesion affecting one lateral half
- Ipsilateral below lesion: Loss of motor function (corticospinal tract), loss of proprioception and vibration (dorsal column)
- Contralateral below lesion: Loss of pain and temperature (spinothalamic tract - crossed 2-3 segments above)
- At the level of lesion: Ipsilateral LMN signs (segmental weakness, loss of all sensation)
Central Cord Syndrome
- Most common incomplete SCI, typically from hyperextension injury in older patients with cervical spondylosis
- Affects the central cord first: arm fibers (cervical) are most central in the lateral corticospinal tract; leg fibers are peripheral
- Classic presentation: Arm weakness > Leg weakness (arms affected worse than legs - "man in a barrel" syndrome)
- Bladder dysfunction (urinary retention) common
- Pain and temperature reduced; proprioception often spared
- Best prognosis for recovery among incomplete syndromes
Anterior Cord Syndrome
- Cause: Anterior spinal artery occlusion (e.g., aortic surgery, hyperflexion injury)
- Bilateral loss of motor function (corticospinal tract), pain, and temperature (spinothalamic) below the level
- Preserved: Posterior column functions (vibration, proprioception, fine touch) - because PSA is intact
- Worst prognosis for ambulation among incomplete syndromes
Posterior Cord Syndrome
- Rare; due to posterior spinal artery occlusion or posterior column damage
- Bilateral loss of vibration, proprioception, and fine touch below the lesion
- Motor function and pain/temperature preserved
- Patient has profound sensory ataxia
Conus Medullaris Syndrome
- Lesion at L1-L2 (the conus)
- Mix of UMN and LMN signs: UMN signs from sacral cord + LMN signs from anterior horn cells
- Bowel and bladder dysfunction, saddle anesthesia (S3-S5 dermatomes), sexual dysfunction
- Lower limb weakness may be present
Cauda Equina Syndrome
- Lesion below the conus (L2 and below) - affects spinal nerve roots, not cord tissue
- Pure LMN signs: Flaccid weakness, areflexia, atrophy
- Saddle anesthesia, bowel/bladder/sexual dysfunction
- Often from large central disc herniation, tumor, or epidural hematoma
- Surgical emergency - early decompression is required
9C. Specific Tract Lesion Syndromes
Syringomyelia:
- Fluid-filled cavity (syrinx) expands within the central cord, destroying crossing fibers of the anterior commissure
- Bilaterally destroys spinothalamic fibers as they cross
- Cape-like dissociated sensory loss: bilateral loss of pain and temperature over the shoulders, arms, and upper trunk - while dorsal columns (proprioception, vibration) are preserved
- As the syrinx enlarges: anterior horn cells destroyed → LMN weakness and wasting of hands; then lateral columns → spastic paraparesis
Subacute Combined Degeneration (B12 deficiency):
- Demyelination of dorsal columns + lateral corticospinal tracts (bilateral)
- Dorsal column: loss of proprioception/vibration → sensory ataxia, positive Romberg
- Corticospinal: UMN signs (spasticity, hyperreflexia, Babinski)
- Combined picture: spastic ataxia, with sensory > motor deficits early
Tabes Dorsalis (3° syphilis):
- Selective degeneration of dorsal roots and dorsal columns
- Loss of proprioception/vibration, severe sensory ataxia (tabetic gait - high-stepping, stamping)
- Charcot joints (neuropathic arthropathy) due to loss of joint position sense
- Lightning pains (episodic lancinating pain)
- Argyll Robertson pupils (accommodate but don't react to light)
Anterior Spinal Artery Syndrome:
- Occlusion of ASA → infarction of anterior 2/3 of cord
- Bilateral paralysis + pain/temperature loss below lesion
- Preserved posterior column (vibration/proprioception)
- Can follow aortic aneurysm repair, embolism
Amyotrophic Lateral Sclerosis (ALS):
- Degeneration of both UMN (lateral corticospinal tracts) and LMN (anterior horn cells)
- Combined UMN + LMN signs in the same patient/same region: fasciculations + hyperreflexia; wasting + spasticity
- Sensory system spared - hallmark of ALS
Spinal Shock:
- Occurs immediately after acute complete cord transection
- Temporary loss of all spinal reflexes below the level of injury (bulbocavernosus, anal wink, muscle stretch reflexes)
- Also: neurogenic hypotension, peripheral vasodilation, ileus, urinary retention
- If lesion at T3 or above: sympathetic tone to heart is lost → bradycardia + hypotension = neurogenic shock triad (bradycardia + hypotension + peripheral vasodilation)
Autonomic Dysreflexia:
- Occurs in chronic complete SCI at T6 or above
- Noxious stimulus below lesion (full bladder, fecal impaction, pressure sore) → massive sympathetic discharge below lesion
- Severe hypertension, pounding headache, flushing/sweating above lesion, bradycardia (baroreceptor-mediated)
- Medical emergency - can cause stroke or myocardial infarction
9D. Causes of Spinal Cord Dysfunction (Harrison's Classification)
| Category | Examples |
|---|---|
| Compressive | Epidural/intradural/intramedullary neoplasm, epidural abscess, epidural hemorrhage, cervical spondylosis, herniated disc, fracture-dislocation |
| Vascular | Anterior spinal artery infarct, AVM, dural fistula, antiphospholipid syndrome |
| Inflammatory/Demyelinating | Multiple sclerosis, neuromyelitis optica (Devic's), sarcoidosis, ADEM |
| Autoimmune | SLE, Sjögren's syndrome, Behcet's disease, anti-MOG, paraneoplastic |
| Infectious | VZV, HSV-1/2, CMV, HIV myelopathy, HTLV-1 (tropical spastic paraparesis) |
| Degenerative | ALS, hereditary spastic paraplegia |
| Metabolic/Nutritional | B12 deficiency (subacute combined degeneration), copper deficiency |
| Developmental/Congenital | Syringomyelia, tethered cord, Chiari malformation |
- Harrison's Principles of Internal Medicine 22E
- Goldman-Cecil Medicine
10. QUICK LOCALIZATION GUIDE
| Finding | Tract Affected | Location |
|---|---|---|
| Contralateral pain/temp loss | Lateral spinothalamic | Anterolateral quadrant, opposite side |
| Ipsilateral proprioception/vibration loss | Fasciculus gracilis/cuneatus | Posterior column, same side |
| Ipsilateral spastic paresis | Lateral corticospinal | Lateral column, same side |
| Bilateral pain/temp loss ("cape") | Crossing spinothalamic fibers | Anterior commissure |
| Bilateral motor + proprioception loss | LCS + dorsal column | Subacute combined degeneration |
| Arm weak > leg weak | LCS (central fibers) | Central cord |
| Loss of motor + pain/temp, preserved proprioception | ASA territory | Anterior 2/3 of cord |
| Loss of proprioception, preserved motor + pain | PSA territory | Posterior 1/3 |
Sources: Gray's Anatomy for Students (ISBN 9780323934237) | Neuroanatomy through Clinical Cases 3rd Ed (ISBN 9781605359625) | Localization in Clinical Neurology 8e (ISBN 9781975160241) | Guyton and Hall Medical Physiology (ISBN 9780443111013) | Harrison's Principles of Internal Medicine 22E (ISBN 9781265977061) | Campbell's Operative Orthopaedics 15th Ed 2026 (ISBN 9780443117633) | Goldman-Cecil Medicine (ISBN 9780323930345)
This is a shared conversation. Sign in to Orris to start your own chat.