I have my university exam of 1 st year of subject biochemistry These are the important long answer give me answer of this "Regulation of blood glucose" and remeber it's a university examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need for a thorough university-level answer. Let me compose the full answer.
Regulation of Blood Glucose
Introduction
Blood glucose concentration is one of the most tightly regulated parameters in human physiology. In a normal fasting adult, blood glucose is maintained between 70-100 mg/dL (some sources quote 80-90 mg/dL). After a meal, it may rise to 120-140 mg/dL, but returns to baseline within about 2 hours. Maintaining this narrow range is essential because glucose is the primary - and often the only - fuel for the brain, retina, and germinal epithelium of the gonads.
Normal Blood Glucose Values
| State | Blood Glucose Level |
|---|---|
| Fasting (normal) | 70-100 mg/dL |
| Postprandial (2h) | <140 mg/dL |
| Impaired fasting glucose | 100-125 mg/dL |
| Diabetes diagnosis | ≥126 mg/dL (fasting) |
Sources of Blood Glucose
Blood glucose is maintained by a balance between glucose entry into the blood and its removal:
Sources that raise blood glucose:
- Intestinal absorption - after carbohydrate-containing meals
- Glycogenolysis - breakdown of glycogen in liver (primary source during short fasting)
- Gluconeogenesis - synthesis of glucose from non-carbohydrate precursors (amino acids, lactate, glycerol) - becomes progressively more important with prolonged fasting
Pathways that lower blood glucose:
- Glycolysis - oxidation of glucose for energy
- Glycogenesis - storage of glucose as glycogen (liver and muscle)
- Lipogenesis - conversion of glucose to fat
- Pentose phosphate pathway - generates NADPH and ribose-5-phosphate
Hormonal Regulation - The Key Players
Blood glucose regulation is primarily hormonal, involving a carefully orchestrated interplay of several hormones. They can be divided into:
- Hypoglycemic hormone: Insulin (only one)
- Hyperglycemic (counterregulatory) hormones: Glucagon, Epinephrine, Cortisol, Growth Hormone, Somatostatin
1. Insulin (the Major Hypoglycemic Hormone)
Source: Beta (β) cells of the Islets of Langerhans in the pancreas
Synthesis: Insulin is synthesized as preproinsulin → proinsulin → insulin + C-peptide. The C-peptide is released in equimolar amounts with insulin and serves as a marker of endogenous insulin secretion.
Stimuli for Insulin Secretion
- Elevated blood glucose (primary stimulus) - glucose enters β cells via GLUT-2 transporters; glucokinase phosphorylates it, raising the ATP/ADP ratio, which closes K⁺ channels, depolarizes the cell membrane, opens Ca²⁺ channels, and triggers exocytosis of insulin granules
- Elevated plasma amino acids (arginine, lysine)
- Gastrointestinal hormones - GLP-1 and GIP (incretins) - these cause an "anticipatory" insulin rise even before food is fully absorbed
- Glucagon, growth hormone, cortisol (potentiate the glucose response)
- Parasympathetic stimulation (vagal activity after a meal)
Stimuli that Decrease Insulin Secretion
- Low blood glucose
- Somatostatin (from δ cells)
- Sympathetic stimulation (α-adrenergic, stress response)
Actions of Insulin on Blood Glucose (Hypoglycemic Effects)
| Tissue | Action |
|---|---|
| Liver | Increases glycogenesis; inhibits glycogenolysis; inhibits gluconeogenesis; promotes glycolysis |
| Muscle | Increases glucose uptake via GLUT-4 translocation; increases glycogenesis; promotes protein synthesis |
| Adipose | Increases glucose uptake via GLUT-4; promotes lipogenesis; inhibits lipolysis (inhibits hormone-sensitive lipase) |
Mechanism of action: Insulin binds to its receptor - a tetrameric receptor tyrosine kinase (α₂β₂ structure). Binding activates the β-subunit's intrinsic tyrosine kinase, leading to autophosphorylation. This triggers phosphorylation of insulin receptor substrates (IRS), activating downstream signaling cascades (PI3K/Akt pathway) that ultimately stimulate GLUT-4 translocation to the cell membrane.
2. Glucagon (the Major Hyperglycemic Hormone)
Source: Alpha (α) cells of the Islets of Langerhans
Primary target: Liver (hepatocytes)
Stimuli for Glucagon Secretion
- Low blood glucose (primary stimulus)
- Elevated plasma amino acids (especially arginine) - prevents hypoglycemia after protein meals
- Catecholamines (epinephrine, norepinephrine) - during stress
Stimuli that Decrease Glucagon Secretion
- Elevated blood glucose
- Insulin (paracrine inhibition)
- Somatostatin
Actions of Glucagon on Blood Glucose (Hyperglycemic Effects)
- Stimulates hepatic glycogenolysis - activates glycogen phosphorylase via cAMP → PKA → phosphorylation cascade
- Stimulates gluconeogenesis - promotes use of amino acids, lactate, glycerol as substrates
- Inhibits glycolysis - decreases fructose 2,6-bisphosphate levels (the allosteric activator of PFK-1)
- Inhibits glycogenesis - phosphorylates and inactivates glycogen synthase
- Promotes lipolysis and fatty acid oxidation - frees glycerol for gluconeogenesis and provides energy
Mechanism: Glucagon binds to Gs-protein coupled receptor → activates adenylyl cyclase → ↑ cAMP → activates PKA → phosphorylates key enzymes.
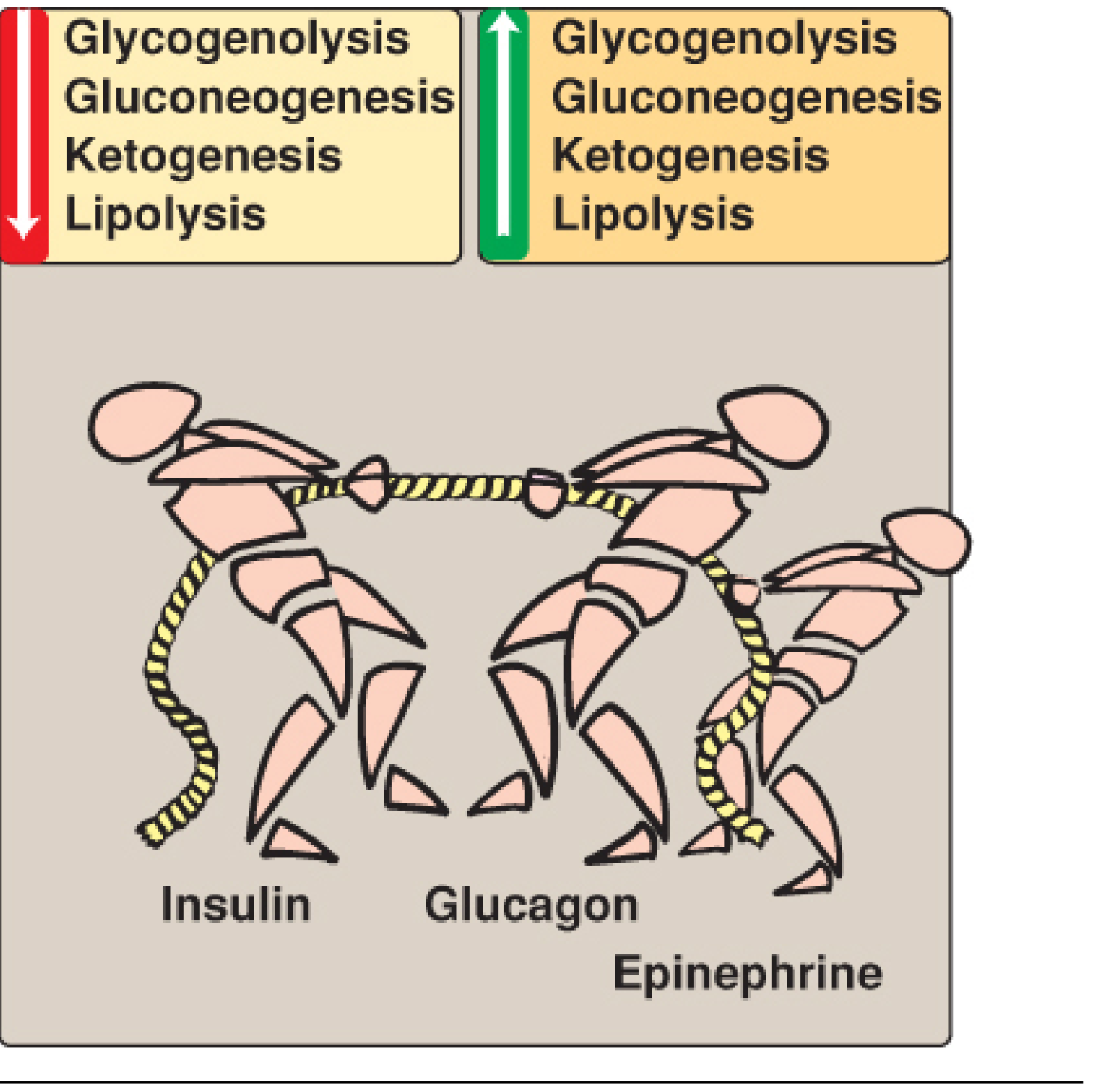
Figure: Tug-of-war between insulin (lowers glycogenolysis, gluconeogenesis, ketogenesis, lipolysis) vs glucagon + epinephrine (raises all of these). - Lippincott's Biochemistry, 8th ed.
3. Epinephrine (Adrenaline)
Source: Adrenal medulla (chromaffin cells)
Trigger: Hypoglycemia, stress, exercise - mediated via hypothalamus → sympathetic nervous system
Actions:
- Strongly stimulates hepatic glycogenolysis (via β-adrenergic receptors → cAMP pathway, and α-adrenergic receptors → IP₃/DAG pathway)
- Stimulates gluconeogenesis in liver
- Stimulates glycogenolysis in muscle
- Promotes lipolysis in adipose (liberates glycerol and fatty acids)
- Inhibits insulin secretion (via α₂-receptors)
4. Cortisol
Source: Adrenal cortex (zona fasciculata); secreted in response to ACTH from the pituitary
Actions (longer-term, over hours to days):
- Stimulates gluconeogenesis (promotes breakdown of muscle protein → amino acids → glucose)
- Decreases glucose utilization by peripheral tissues (anti-insulin effect)
- Decreases glucose uptake by muscles and adipose (reduces GLUT expression)
- Promotes lipolysis
5. Growth Hormone
Source: Anterior pituitary; secreted during hypoglycemia via hypothalamic signaling
Actions:
- Decreases glucose uptake and utilization by muscle and fat
- Promotes lipolysis (spares glucose)
- Stimulates gluconeogenesis
- Called "diabetogenic" because it antagonizes insulin action
6. Somatostatin
Source: Delta (δ) cells of the Islets of Langerhans; also secreted from the hypothalamus
Action: Inhibits both insulin and glucagon secretion, thereby modulating the rate of glucose entry into blood after a meal (acts as a "governor").
The Liver as the Central Buffer Organ
The liver plays a uniquely important role in blood glucose regulation because it:
- Is the only organ (besides kidney) that expresses glucose-6-phosphatase, allowing it to release free glucose into the blood
- Rapidly takes up glucose after a meal (stores up to 2/3 of absorbed glucose as glycogen)
- Releases glucose back during fasting via glycogenolysis and gluconeogenesis
- Monitors blood glucose via glucokinase (hepatic glucose sensor), which is not inhibited by its product glucose-6-phosphate, and increases activity proportionally with glucose concentration
Without the liver buffer, fluctuations in blood glucose after meals would be approximately 3 times greater.
Integrated Response: Fed vs. Fasted State
Postprandial (Fed) State - "Anabolic"
Blood glucose rises → Insulin ↑, Glucagon ↓
- Liver: glycogenesis ↑, glycolysis ↑, gluconeogenesis ↓
- Muscle: glucose uptake ↑ (GLUT-4), glycogenesis ↑, protein synthesis ↑
- Adipose: glucose uptake ↑ (GLUT-4), lipogenesis ↑, lipolysis ↓
Fasting State - "Catabolic"
Blood glucose falls → Glucagon ↑, Insulin ↓
- Liver: glycogenolysis ↑ (first 12 hours), then gluconeogenesis ↑
- Muscle: amino acid release (alanine) → substrate for gluconeogenesis
- Adipose: lipolysis ↑ → glycerol and fatty acids released
Prolonged Fasting / Starvation
- Glucagon + cortisol + growth hormone dominate
- Ketone bodies produced by liver become fuel for the brain
- Muscle protein catabolism supplies amino acids for gluconeogenesis
Counterregulatory Response to Hypoglycemia
When blood glucose falls below ~70 mg/dL, a sequential series of counterregulatory responses is triggered:
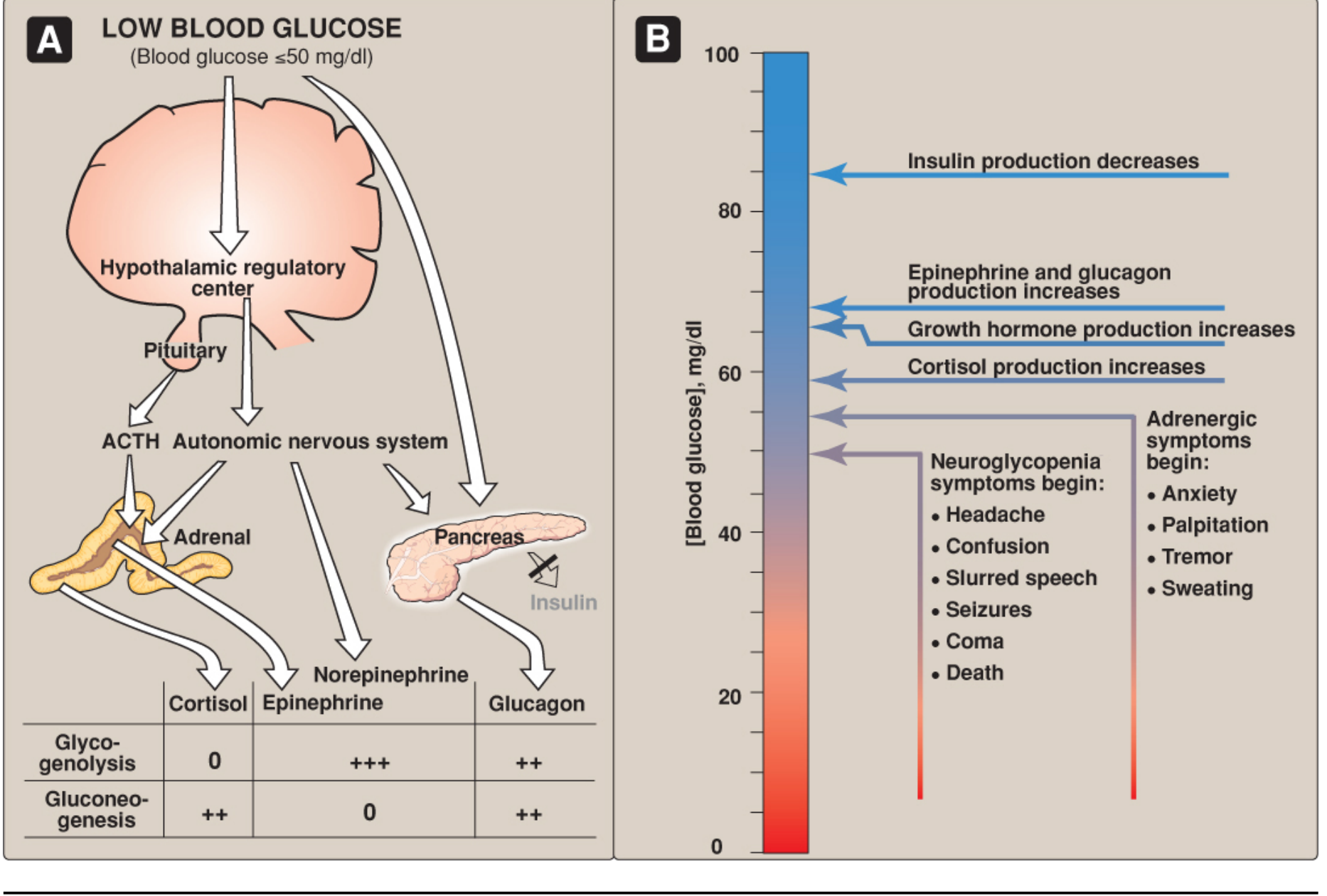
Figure: (A) Hypothalamic-pituitary-adrenal and autonomic responses to hypoglycemia. (B) Sequential glycemic thresholds at which each counterregulatory response is activated. - Lippincott's Biochemistry, 8th ed.
Order of activation (as glucose falls progressively):
- ~85 mg/dL: Insulin secretion decreases
- ~68 mg/dL: Glucagon and epinephrine secretion increases
- ~66 mg/dL: Growth hormone secretion increases
- ~58 mg/dL: Cortisol secretion increases
- ~50 mg/dL: Adrenergic symptoms appear (anxiety, sweating, palpitations, tremor)
- <50 mg/dL: Neuroglycopenic symptoms appear (confusion, seizures, coma, death)
The hypothalamic glucoreceptors detect low glucose and activate:
- The sympathetic nervous system → epinephrine release
- The anterior pituitary → ACTH release → cortisol; GH release
Summary Table: Hormonal Regulation at a Glance
| Hormone | Source | Blood Glucose Effect | Key Mechanism |
|---|---|---|---|
| Insulin | β cells, pancreas | Decreases ↓ | Glycogenesis ↑, Glycolysis ↑, GLUT-4 translocation, gluconeogenesis ↓ |
| Glucagon | α cells, pancreas | Increases ↑ | Glycogenolysis ↑, gluconeogenesis ↑ (cAMP pathway) |
| Epinephrine | Adrenal medulla | Increases ↑ | Glycogenolysis ↑↑↑ (liver+muscle), gluconeogenesis ↑ |
| Cortisol | Adrenal cortex | Increases ↑ | Gluconeogenesis ↑↑, peripheral glucose use ↓ |
| Growth Hormone | Anterior pituitary | Increases ↑ | Anti-insulin effect, gluconeogenesis ↑, lipolysis ↑ |
| Somatostatin | δ cells, pancreas | Modulator | Inhibits both insulin and glucagon |
| GLP-1, GIP | Intestinal L/K cells | Indirect ↓ | Potentiate insulin secretion (incretins) |
Why Blood Glucose Regulation Matters
- Brain dependency - the brain cannot synthesize or store glucose; it requires a continuous supply (uses ~120 g/day)
- Hyperglycemia causes osmotic diuresis, glycation of proteins, damage to blood vessels and nerves
- Hypoglycemia causes neurological dysfunction, seizures, coma, and death if uncorrected
- Failure of this regulatory system leads to Diabetes Mellitus (Type 1: no insulin; Type 2: insulin resistance)
Key Points for Examination
- Normal fasting blood glucose: 70-100 mg/dL
- Insulin is the only hormone that lowers blood glucose
- Glucagon is insulin's principal antagonist and the first responder to hypoglycemia
- The insulin receptor is a receptor tyrosine kinase (α₂β₂ tetramer)
- GLUT-4 translocation to the cell membrane requires insulin (in muscle and adipose)
- GLUT-2 (liver and β cells) and glucokinase act together as the glucose sensor system
- The liver is the central glucose buffer - expresses glucose-6-phosphatase (allows glucose release)
- Cortisol and growth hormone are long-term counterregulatory hormones; epinephrine and glucagon are short-term
- The C-peptide is released in equimolar amounts with insulin and measures endogenous insulin production
Sources: Lippincott Illustrated Reviews: Biochemistry, 8th ed. | Guyton & Hall Textbook of Medical Physiology | Basic Medical Biochemistry - A Clinical Approach, 6th ed. | Tietz Textbook of Laboratory Medicine, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.