Pathogenesis of developmental dysplasia of femor
developmental dysplasia hip pathogenesis
Developmental Dysplasia of the Hip (DDH) - Pathogenesis
- Campbell's Operative Orthopaedics 15th Ed, p. 1402
- Miller's Review of Orthopaedics 9th Ed, p. 2797
Spectrum of Disease (Classification)
| Type | Description |
|---|---|
| Dysplasia | Shallow acetabulum, hip in joint |
| Subluxation | Partial dislocation; femoral head partially outside acetabulum |
| Dislocation | Complete loss of contact between femoral head and acetabulum |
| Teratologic | Dislocated in utero, irreducible; associated with neuromuscular conditions |
| Late dysplasia | Presents in adolescence or adulthood |
Theories of Pathogenesis
1. Mechanical / Intrauterine Positional Factors
-
Breech presentation (especially extended breech) causes abnormal hip flexion forces, easily producing femoral head dislocation. Breech is found in 3-4% of all deliveries, but in up to 30-50% of DDH cases.
-
The most common intrauterine position is left occiput anterior (LOA), which places the left hip in adduction against the rigid maternal lumbosacral spine - partially explaining why the left hip is more commonly affected (67% of cases).
-
Oligohydramnios restricts fetal movement, increasing mechanical stress on the hip.
-
Firstborn children have less intrauterine space (tighter primigravid uterus), restricting movement and predisposing to DDH.
-
Campbell's, p. 1402; Bailey & Love, p. 636
2. Hormone-Induced Joint Laxity
-
The maternal hormone relaxin, which relaxes the maternal pelvis during delivery, can cross the placenta and is transmitted via breast milk (in animal models).
-
This produces ligamentous laxity in the neonate, allowing dislocation of the femoral head in the perinatal period.
-
Girls are 4-5 times more commonly affected, presumably because they are more sensitive to the effects of relaxin and maternal estrogens.
-
Generalized joint laxity (often dominantly inherited) is also associated with DDH.
-
Campbell's, p. 1402; The Developing Human, p. 1007; Bailey & Love, p. 636
3. Primary Acetabular Dysplasia
-
Abnormal development of the acetabulum occurs in approximately 15% of neonates with DDH.
-
Breech posture during the terminal months of pregnancy may result in abnormal development of both the acetabulum and the head of the femur.
-
Without a properly formed acetabulum, the femoral head lacks bony coverage and stability.
-
The Developing Human, p. 1007
4. Genetic / Hereditary Factors
- A positive family history increases the risk of DDH significantly (approximately 10-20% incidence in first-degree relatives).
- The condition follows a multifactorial pattern of inheritance.
- DDH is more common in white and Navajo children and less common in Chinese and Black children, suggesting genetic predisposition.
- A 2024 systematic review (Jacobsen et al., BMC Musculoskeletal Disorders, PMID 39354451) confirms multiple genetic loci associated with DDH.
Risk Factors (in order of importance)
- Breech positioning (strongest)
- Positive family history / ligamentous laxity
- Female sex (~85% of cases)
- Firstborn child
- Left hip predisposition
- Oligohydramnios
- Congenital torticollis (~8% coexistence), metatarsus adductus
- Postnatal swaddling with hips in extension
Pathological Anatomy - Secondary Changes
- The acetabulum becomes increasingly shallow and dysplastic
- The acetabular labrum (limbus) becomes inverted and hypertrophied, blocking reduction
- The acetabular fossa fills with fibrofatty tissue (pulvinar), obstructing reduction
- The femoral head loses its normal round shape
- Increased femoral anteversion and valgus develop
- A pseudoacetabulum may form at the site of chronic dislocation
- The hip capsule becomes contracted (especially the inferomedial portion)
- The iliopsoas tendon constricts the contracted capsule (hourglass deformity)
- The ligamentum teres becomes hypertrophied and elongated
- The transverse acetabular ligament tightens across the acetabular floor
Iliopsoas tendon → Pulvinar → Hypertrophied ligamentum teres → Contracted inferomedial capsule → Transverse acetabular ligament → Inverted labrum
- Miller's Review of Orthopaedics, p. 2831
Cultural / Postnatal Factors
- Swaddling the legs together (hips in extension and adduction) exacerbates instability.
- Carrying babies astride the caregiver with hips in flexion and abduction improves hip stability.
- The relatively low incidence in Chinese children and high incidence in Navajo children likely reflects postnatal cultural practices combined with genetic susceptibility.
Recent Evidence Update
Create a visual summary of DDH pathology stages (dysplasia→subluxation→dislocation)
Medical educational diagram showing the 4 stages of Developmental Dysplasia of the Hip (DDH) in a horizontal progression. Clean clinical illustration style on white background. Stage 1 - NORMAL HIP: Cross-section showing femoral head perfectly seated in deep acetabulum, round femoral head, normal labrum, normal joint space. Label: "Normal Hip" Stage 2 - DYSPLASIA: Shallow acetabulum with inadequate coverage of femoral head, femoral head still in joint but poorly covered, labrum beginning to deform. Label: "Dysplasia - Shallow acetabulum, femoral head in joint but uncovered" Stage 3 - SUBLUXATION: Femoral head partially displaced laterally and superiorly out of shallow acetabulum, labrum inverted, capsule stretched. Label: "Subluxation - Partial displacement, labrum inversion begins" Stage 4 - DISLOCATION: Femoral head completely outside acetabulum, displaced superolaterally, acetabulum filled with pulvinar (fibrofatty tissue), hypertrophied ligamentum teres, contracted capsule with hourglass deformity from iliopsoas, pseudoacetabulum forming. Label: "Dislocation - Complete displacement, secondary changes: pulvinar, inverted labrum, contracted capsule" Below the stages, a horizontal arrow labeled "Spectrum of DDH" pointing right. Each stage connected by arrows showing progression. At the bottom, a summary box listing secondary soft tissue obstructions to reduction: Iliopsoas tendon, Pulvinar, Ligamentum teres (hypertrophied), Inferomedial capsule (contracted), Transverse acetabular ligament, Inverted labrum. Color coding: Normal = green tones, Dysplasia = yellow, Subluxation = orange, Dislocation = red. Femoral head = pink sphere, acetabulum = blue/grey bone, cartilage = light blue, soft tissue = peach.
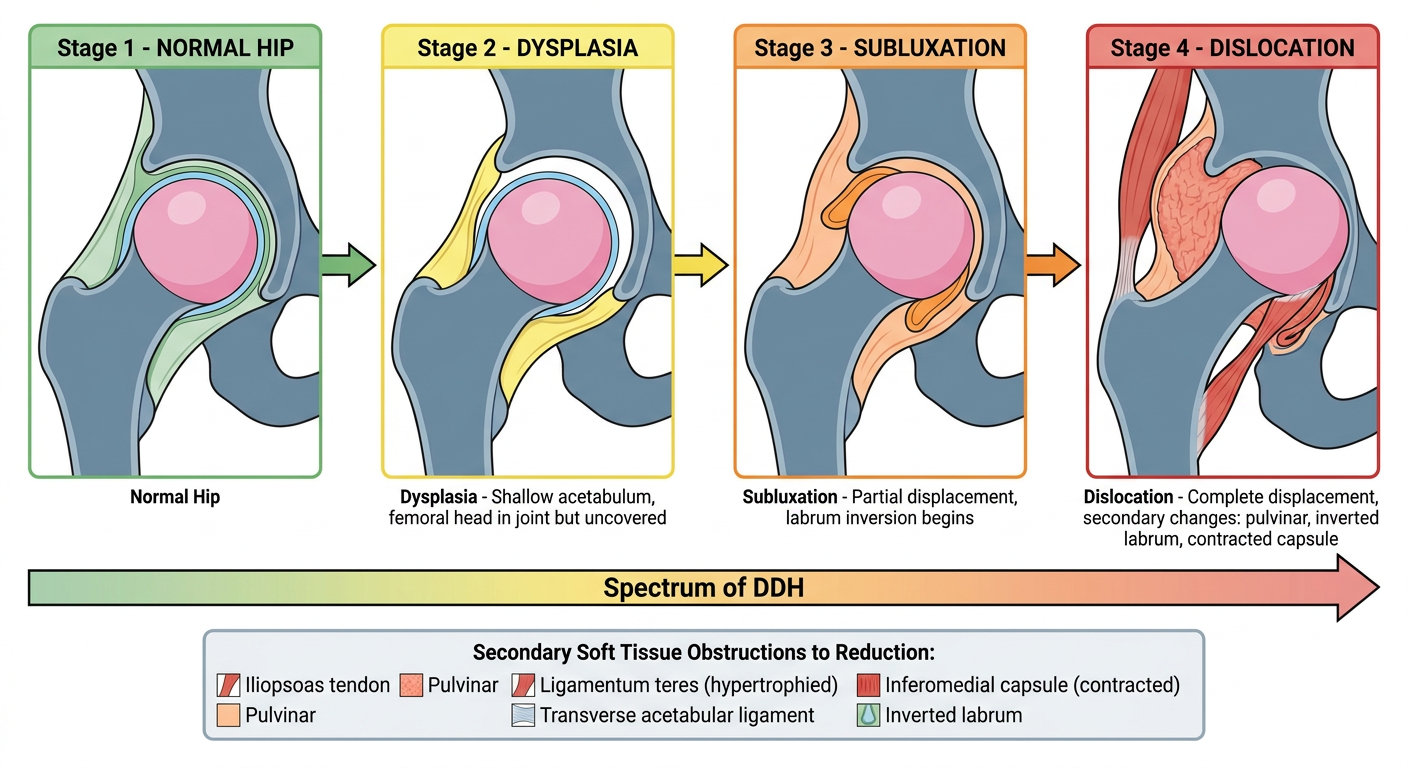
- Normal Hip - femoral head fully seated in a deep acetabulum
- Dysplasia - shallow acetabulum with inadequate femoral head coverage (still in joint)
- Subluxation - partial lateral/superior displacement, labrum begins to invert
- Dislocation - complete displacement with all secondary changes labeled:
- Pulvinar filling the acetabulum
- Inverted/hypertrophied labrum
- Contracted hourglass capsule from iliopsoas
- Pseudoacetabulum formation