Vasomotor control of nasal mucosa in detail for 20 marker question, in ms ent exam, according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed for a comprehensive 20-marker answer. Let me compose it.
Vasomotor Control of Nasal Mucosa
(A 20-marker answer for MS ENT examination, based on Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, K.J. Lee's Essential Otolaryngology, and Gray's Anatomy)
Introduction
The nasal mucosa is highly vascular and its blood flow is tightly regulated by the autonomic nervous system - a process collectively termed vasomotor control. This regulation determines nasal airway resistance, turbinate congestion, and nasal secretions. An adult inspires approximately 10,000 litres of air daily, and the nose accounts for up to 50% of the total airway resistance; therefore, fine vasomotor control is essential for normal respiratory homeostasis.
Vascular Architecture of the Nasal Mucosa
Before understanding vasomotor control, the vascular architecture must be appreciated.
The nasal mucosa contains three distinct vascular compartments:
- Arterioles - resistance vessels that regulate inflow
- Arteriovenous (AV) anastomoses - direct shunts between arterioles and venules, bypassing capillaries; their patency determines the extent of blood directed into sinusoids
- Venous sinusoids - large capacitance vessels forming the erectile tissue of the nasal mucosa, particularly concentrated on the anterior nasal septum and the inferior turbinates
The venous sinuses (cavernous sinusoidal tissue) have the ability to expand and shrink, directly impacting nasal resistance and airflow. Animal studies show nasal resistance increases by 1.2-1.3% per mmHg rise in venous pressure.
Two mechanisms govern nasal mucosal vessel capacitance:
- Hydrostatic pressure: Increased blood pressure expands the venous sinusoids passively
- Autonomic nervous system: Controls smooth muscle in the walls of arteriovenous anastomoses, actively regulating blood flow
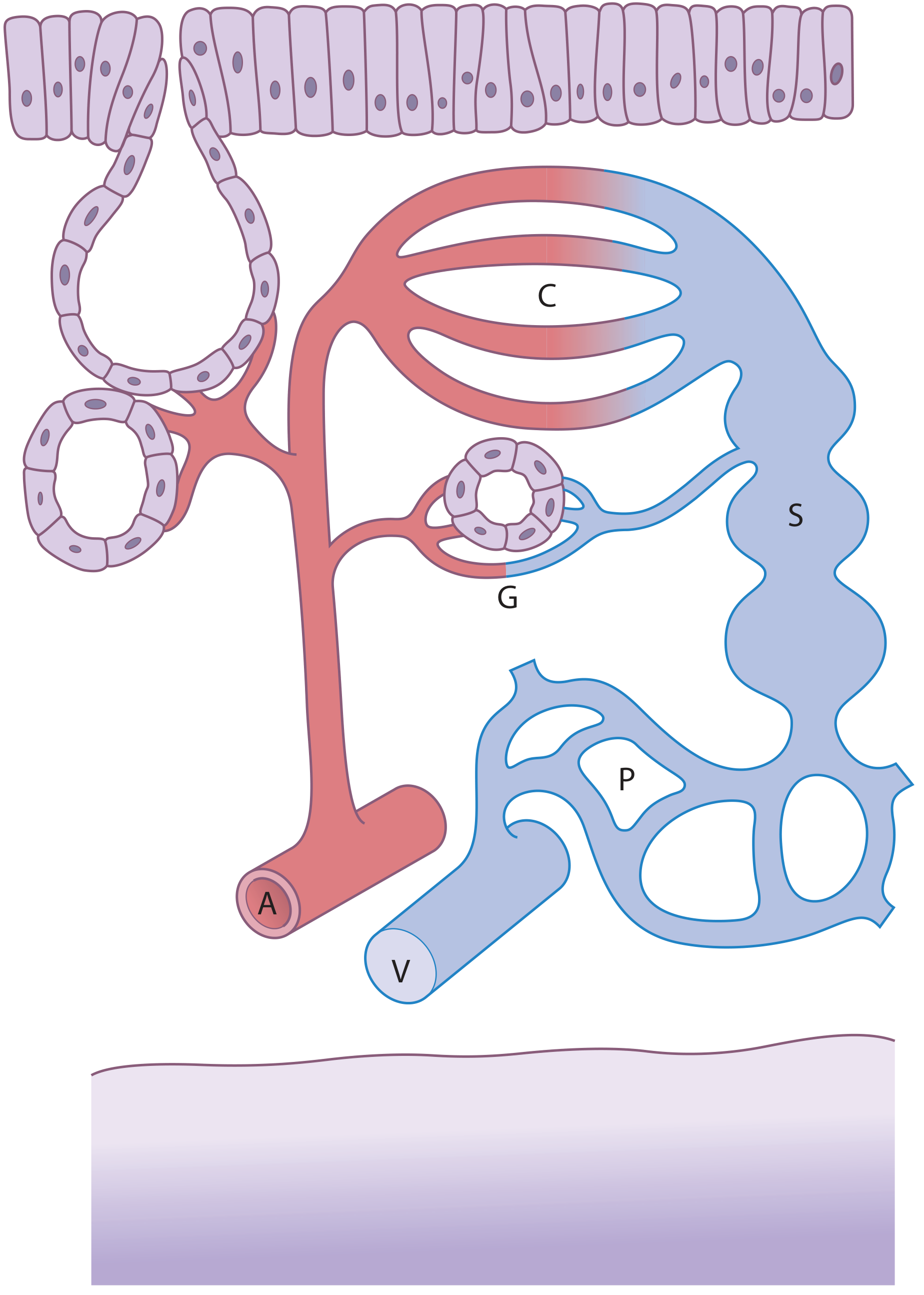
Fig: Schematic of the blood supply of the turbinates. A = arteriole; V = venule; C = capillaries; G = interstitial glands; P = venous plexus; S = venous sinusoids. (Scott-Brown's Otorhinolaryngology)
Autonomic Innervation of the Nasal Mucosa
The nasal mucosa receives both sympathetic and parasympathetic autonomic innervation. The key relay station for both is the sphenopalatine (pterygopalatine) ganglion.
1. Sympathetic Innervation
Function: Vasoconstriction and reduction in secretomotor activity
Pathway:
| Level | Structure |
|---|---|
| Centre | Hypothalamus (posterolateral) → descends in spinal cord |
| Preganglionic | Lateral horn cells of thoracic cord (T1) → enter sympathetic chain |
| First relay | Ascend in sympathetic trunk → Superior cervical ganglion (synapse) |
| Postganglionic | Follow internal carotid artery into the cranial cavity → leave as deep petrosal nerve |
| Vidian nerve | Deep petrosal nerve + Greater superficial petrosal nerve → Vidian nerve (nerve of pterygoid canal) |
| Terminal | Pass through the sphenopalatine ganglion without synapsing → distributed with branches of V2 (maxillary nerve) to nasal mucosa |
Target structures: Smooth muscle in walls of arterioles and venous sinusoids
Neurotransmitter: Noradrenaline (norepinephrine)
Effect on nasal mucosa:
- Vasoconstriction of arterioles and sinusoids → nasal decongestion
- Reduction in secretomotor activity of mucous glands
- Net effect: patent nasal airway, reduced secretions
"Sympathetic fibres predominantly innervate smooth muscle in the walls of arterioles and sinusoids. The primary neurotransmitter is noradrenalin, which causes vasoconstriction of the blood vessels." - Scott-Brown's Otorhinolaryngology
2. Parasympathetic Innervation
Function: Vasodilation and secretomotor stimulation
Pathway:
| Level | Structure |
|---|---|
| Centre | Superior salivatory nucleus (pons, CN VII) |
| Preganglionic | Travel in nervus intermedius → leave CN VII at geniculate ganglion → Greater superficial petrosal nerve (GSPN) |
| Vidian nerve | GSPN + deep petrosal nerve → Vidian nerve → enters sphenopalatine fossa |
| Relay | Synapse in sphenopalatine (pterygopalatine) ganglion |
| Postganglionic | Distributed to nasal mucosa with deep branches of V2 (maxillary nerve) |
Neurotransmitters (two primary):
- Acetylcholine (ACh) - acts on muscarinic receptors → induces serous (watery) secretions from mucous glands
- Vasoactive Intestinal Peptide (VIP) - a co-transmitter → causes vasodilation of nasal mucosal blood vessels
Effect on nasal mucosa:
- Vasodilation of sinusoids and capillaries → nasal congestion
- Increased nasal secretions (serous and mucous)
- Net effect: nasal stuffiness and rhinorrhoea
"Parasympathetic system controls the congestion and increases nasal secretions by vasodilation of the sinusoids and capillaries in the mucosa, whereas the sympathetic system provides a steady vasoconstrictor tone." - Cummings Otolaryngology
The Nasal Cycle
The nasal cycle is a key clinical expression of vasomotor control. It was first described by Heetderks in 1927.
Key features:
- Observed in approximately 80% of the normal population
- Characterised by alternating turgescence (congestion) of the inferior turbinates on each side
- While one side congests, the contralateral side decongests
- Total nasal resistance remains constant throughout the cycle
- Mean cycle duration: approximately 2.5 hours
- Controlled by alternating sympathetic tone to each side, regulated by the hypothalamus
Positional effect: The turbinates in the dependent nasal fossa fill when the patient is in the lateral decubitus position (due to altered venous pressure and reflex sympathetic changes). This may have the physiological purpose of causing a sleeping person to turn sides.
Clinical relevance: In patients with a fixed septal deviation, the nasal cycle becomes clinically evident - when the normal (undeviated) side congests during its phase, the patient notices obstruction that mirrors the congestion phase.
Neural Reflexes in Vasomotor Control
Nasal vasomotor tone is also modulated by several reflex arcs:
| Reflex | Stimulus | Response |
|---|---|---|
| Nasobronchial reflex | Cold/irritant contact with nasal mucosa | Bronchoconstriction via vagal arc |
| Diving reflex | Cold water on face | Intense sympathetic nasal vasoconstriction |
| Exercise | Physical activity | Sympathetic tone rises → nasal decongestion |
| Postural/body position | Lateral decubitus | Dependent side congests |
| Sexual arousal | Autonomic | Nasal congestion (parasympathetic) |
Non-Neural Factors Modifying Vasomotor Control
Several additional factors influence nasal vascular tone:
- Temperature and humidity: Cold, dry air stimulates mucosal engorgement (protective)
- Hormonal influences: Exogenous hormones and oral contraceptives alter neural input to the mucosa and may cause mucosal hypertrophy and obstruction (e.g., pregnancy rhinitis)
- Medications:
- Sympathomimetics (ephedrine, xylometazoline): act on alpha-1 receptors → vasoconstriction → decongestant effect
- Rebound vasodilation (rhinitis medicamentosa) after prolonged use
- Beta-blockers (for hypertension): block sympathetic vasoconstrictive tone → nasal congestion
- Ipratropium bromide: blocks muscarinic receptors → reduces secretions (used in vasomotor rhinitis)
- Pilocarpine (parasympathomimetic): causes vasodilation and watery secretions
Summary Table: Sympathetic vs. Parasympathetic Vasomotor Effects
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Centre | Hypothalamus / T1 spinal cord | Superior salivatory nucleus (pons) |
| Preganglionic relay | Superior cervical ganglion | Geniculate ganglion (not a relay - passes through) |
| Postganglionic relay | None (passes through SPG) | Sphenopalatine ganglion |
| Nerve | Deep petrosal → Vidian nerve | GSPN → Vidian nerve |
| Neurotransmitter | Noradrenaline | Acetylcholine + VIP |
| Receptor | Alpha-1 adrenergic | Muscarinic (M3) |
| Effect on vessels | Vasoconstriction | Vasodilation |
| Effect on glands | Reduced secretion | Increased serous/mucous secretion |
| Net nasal effect | Decongestion (patent airway) | Congestion + rhinorrhoea |
| Target tissue | Smooth muscle of arterioles & sinusoids | Mucous glands + sinusoidal endothelium |
Clinical Applications
-
Vasomotor rhinitis (Non-allergic rhinitis): Dysregulation of autonomic (particularly parasympathetic) control leads to chronic rhinorrhoea and congestion without an immunological basis. Treatment includes topical ipratropium bromide and posterior nasal nerve neurectomy/vidian neurectomy.
-
Nasal decongestants: Topical alpha-adrenergic agonists (xylometazoline, oxymetazoline) mimic sympathetic vasoconstriction. Resistance to nasal airflow reduces by one-third after topical decongestion.
-
Rhinitis medicamentosa: Rebound vasodilation from prolonged sympathomimetic use, from down-regulation of alpha receptors.
-
Vidian neurectomy: Surgical section of the vidian nerve eliminates parasympathetic input to the nasal mucosa; used in refractory vasomotor rhinitis.
-
Nasal cycle in septal deviation: Patients with deviated nasal septum experience cyclical worsening of nasal obstruction correlating with the congestion phase of the nasal cycle on the narrowed side.
Conclusion
Vasomotor control of the nasal mucosa is a dynamic, autonomically regulated process. The sympathetic system, via noradrenaline, maintains basal vasoconstrictor tone to keep the airway patent. The parasympathetic system, via acetylcholine and VIP, produces vasodilation and glandular secretion. The interplay of these two systems, mediated through the sphenopalatine ganglion and vidian nerve, governs the nasal cycle, mucosal blood flow, and secretions. Disruption of this balance results in clinically significant conditions such as vasomotor rhinitis.
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Chapters 87 & 89 (Nasal Physiology, Nasal Blood Flow, Autonomic Nervous System)
- Cummings Otolaryngology Head and Neck Surgery, Chapter on Nasal Physiology: Resistance and Airflow; Nasal Cycle
- K.J. Lee's Essential Otolaryngology, Chapter on Autonomic Innervation of Nasal Mucosa
- Gray's Anatomy for Students, Sympathetic and Parasympathetic Innervation of Nasal Cavity
This is a shared conversation. Sign in to Orris to start your own chat.