Varicose vein in surgery in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"varicose veins"[MeSH Terms] AND "surgical treatment"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
varicose vein surgery saphenous stripping stab avulsion
I now have comprehensive content from multiple authoritative surgical textbooks. Let me compile a thorough, well-structured answer.
Varicose Veins — A Surgical Overview
1. Definition and Epidemiology
Varicose veins are dilated, tortuous, subcutaneous veins measuring ≥3 mm in diameter that result from sustained venous hypertension and valvular incompetence. They affect at least 10% of the general population, rising to >55% by age 65 (Edinburgh Vein Study). More time is lost from work due to vein-related pathology than from all arterial disease combined, including coronary artery disease. Annual US healthcare costs for chronic venous disease approach $1 billion.
— Schwartz's Principles of Surgery, 11e; Current Surgical Therapy, 14e
2. Anatomy of the Venous System
Key Vessels
| Structure | Relevance |
|---|---|
| Great Saphenous Vein (GSV) | Runs medially from foot to saphenofemoral junction (SFJ) in groin; most commonly affected |
| Small Saphenous Vein (SSV) | Runs posterolaterally to saphenopopliteal junction (SPJ) behind knee |
| Perforating veins | Connect superficial to deep system; incompetent perforators transmit deep venous hypertension |
| Deep venous system | Femoral, popliteal, tibial veins — must be assessed before any superficial intervention |
The saphenofemoral junction (where GSV drains into femoral vein) and saphenopopliteal junction are the critical sites of reflux in most patients.
3. Pathophysiology
Primary Varicose Veins
Result from intrinsic weakness of the venous wall and/or primary valvular incompetence — no underlying cause identified. The structural defect leads to venous dilation → valve cusps cannot coapt → reflux propagates distally.
Secondary Varicose Veins
Caused by identifiable conditions:
- Post-thrombotic syndrome (PTS) — DVT destroys valve architecture; the most common secondary cause
- Pregnancy and pelvic tumors (extrinsic compression)
- Arteriovenous fistulae
- Congenital syndromes: Klippel-Trenaunay syndrome, Parkes Weber syndrome, Ehlers-Danlos, May-Thurner syndrome
Hemodynamic Consequences
Valvular incompetence → ambulatory venous pressure (AVP) elevation → hydrostatic overload in the microcirculation. Skin manifestations are uncommon with AVP <35 mmHg but almost certain with AVP >90 mmHg. Sustained venous hypertension leads to:
- Capillary leakage → edema
- Leukocyte adhesion and activation → fibrin cuff deposition, lipodermatosclerosis
- Eventual ulceration (CEAP C6)
— Current Surgical Therapy, 14e; Schwartz's Principles of Surgery, 11e
4. CEAP Classification (2020 Revision)
The Clinical-Etiology-Anatomy-Pathophysiology (CEAP) system is the international standard:
| Class | Description |
|---|---|
| C0 | No visible or palpable signs |
| C1 | Telangiectasias or reticular veins (<3 mm) |
| C2 | Varicose veins (≥3 mm) |
| C2r | Recurrent varicose veins |
| C3 | Edema |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C4c | Corona phlebectatica |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
| C6r | Recurrent active venous ulcer |
The Venous Clinical Severity Score (r-VCSS) complements CEAP for monitoring outcomes.
— Current Surgical Therapy, 14e
5. Clinical Features
Symptoms
- Aching, heaviness, fatigue of the affected limb
- Pruritus over varicosities
- Mild ankle edema — worse at end of day
- All symptoms worsen with prolonged standing/sitting and are relieved by leg elevation
Signs — Progressive Severity
- Dilated, tortuous, visible superficial veins
- Telangiectasias and reticular veins
- Ankle edema
- Hyperpigmentation (hemosiderin deposition)
- Lipodermatosclerosis (fibrotic, woody induration of gaiter area)
- Atrophie blanche (white stellate scarring)
- Venous ulcer (typically medial malleolus)
- Thrombophlebitis and variceal bleeding
6. Investigations
Duplex Ultrasonography (DUS) — Gold Standard
- Maps superficial and deep venous anatomy
- Identifies sites of reflux (SFJ, SPJ, perforators)
- Rules out deep venous obstruction or post-thrombotic changes
- Mandatory before any intervention in patients with prior venous surgery, recurrent disease, or suspected deep incompetence
- Reflux is defined as retrograde flow >0.5 seconds after compression release
Other Investigations
- Venography — reserved for complex cases, deep venous reconstruction planning
- Plethysmography — measures venous reflux quantitatively
- CT/MR venography — for suspected iliac outflow obstruction (May-Thurner)
7. Management
7A. Conservative (Non-operative) Management
Elastic Compression Stockings (ECS)
- First-line treatment for all symptomatic patients
- Graduated compression: 20–30, 30–40, or 40–50 mmHg
- Length: knee-high to waist-high — should cover all symptomatic varices
- Reduces ambulatory venous pressure, relieves symptoms in many patients
- Continue indefinitely to prevent progression
Lifestyle Measures
- Weight reduction
- Leg elevation when resting
- Avoidance of prolonged standing
- Regular walking (activates calf muscle pump)
Indications for Intervention
Intervention is warranted when:
- Symptoms worsen despite compression therapy
- Lipodermatosclerosis or active/healed ulcer (CEAP C4b–C6)
- Thrombophlebitis, variceal bleeding
- Patient preference (cosmesis or significant quality-of-life impairment)
- Randomized trials demonstrate improved quality of life with interventional treatment over compression alone
7B. Sclerotherapy
Mechanism: Chemical destruction of venous endothelium → fibrosis → permanent obliteration.
Sclerosing Agents & Concentrations:
| Indication | Agent | Concentration |
|---|---|---|
| Telangiectasias | Hypertonic saline | 11.7–23.4% |
| Telangiectasias | Sodium tetradecyl sulfate (STS) | 0.125–0.25% |
| Telangiectasias | Polidocanol | 0.5% |
| Larger varicose veins | Hypertonic saline | 23.4% |
| Larger varicose veins | STS | 0.5–1.0% |
| Larger varicose veins | Polidocanol | 0.75–1.0% |
Technique:
- Inject sclerosant into target vein
- Apply elastic bandage immediately; worn continuously for 3–5 days
- After bandage removal, wear compression stocking for minimum 2 weeks
Foam Sclerotherapy (UGS):
- Sclerosant is aerated to form microfoam (Tessari technique)
- Displaces blood, maximizing endothelial contact
- Used for GSV/SSV under ultrasound guidance
- Up to 15 mL foam per session; sessions can be repeated in 24 hours
- Prefabricated polidocanol microfoam (Varithena/PEM) is FDA-approved (2013) for incompetent superficial veins
Complications of Sclerotherapy:
- Allergic reaction (rare anaphylaxis)
- Local skin hyperpigmentation (~10–30%)
- Superficial thrombophlebitis
- DVT
- Skin necrosis (if perivenous injection)
- Visual disturbances/stroke (paradoxical embolism via PFO — more common with foam)
— Schwartz's Principles of Surgery, 11e
7C. Endovenous Thermal Ablation (EVTA)
The preferred first-line treatment for GSV and SSV incompetence, replacing open surgery in most centers.
Radiofrequency Ablation (RFA) — ClosureFast™ system
Mechanism: Resistive heating of catheter electrode to 120°C → collagen contraction → vein wall fibrosis → obliteration.
Procedure:
- Ultrasound-guided percutaneous access (typically at knee level for GSV)
- Advance catheter to within 2 cm of the SFJ (or 3 cm from SPJ for SSV)
- Infiltrate tumescent anesthesia (dilute lidocaine + sodium bicarbonate in saline) perivenously under ultrasound — creates thermal barrier, collapses vein
- Trendelenburg positioning (empties vein of blood)
- Activate catheter; heat for 20 seconds per segment, withdraw 6.5 cm
- Repeat until entire treatment length is ablated
- Apply compression from foot to thigh post-procedure
For perforator veins (RFA):
- Treat four quadrants for 60 seconds each
- Withdraw 5 mm and repeat
Endovenous Laser Ablation (EVLA)
Mechanism: Laser energy (660–1470 nm) absorbed by hemoglobin/water in vein wall → heat → endothelial destruction and collagen shrinkage.
Most used wavelength: 1470 nm (water-absorbing; less post-procedural pain than older 810/980 nm).
Procedure:
- Ultrasound-guided access with microsheath and 0.035-inch guidewire
- Position laser fiber tip ≥2 cm distal to epigastric vein at SFJ (for SSV: ≥3 cm from SPJ)
- Tumescent anesthesia + Trendelenburg
- Pull back fiber+sheath 1 cm every 3–5 seconds
- Energy delivery: 40 J/cm (1470 nm) or 80 J/cm (810 nm)
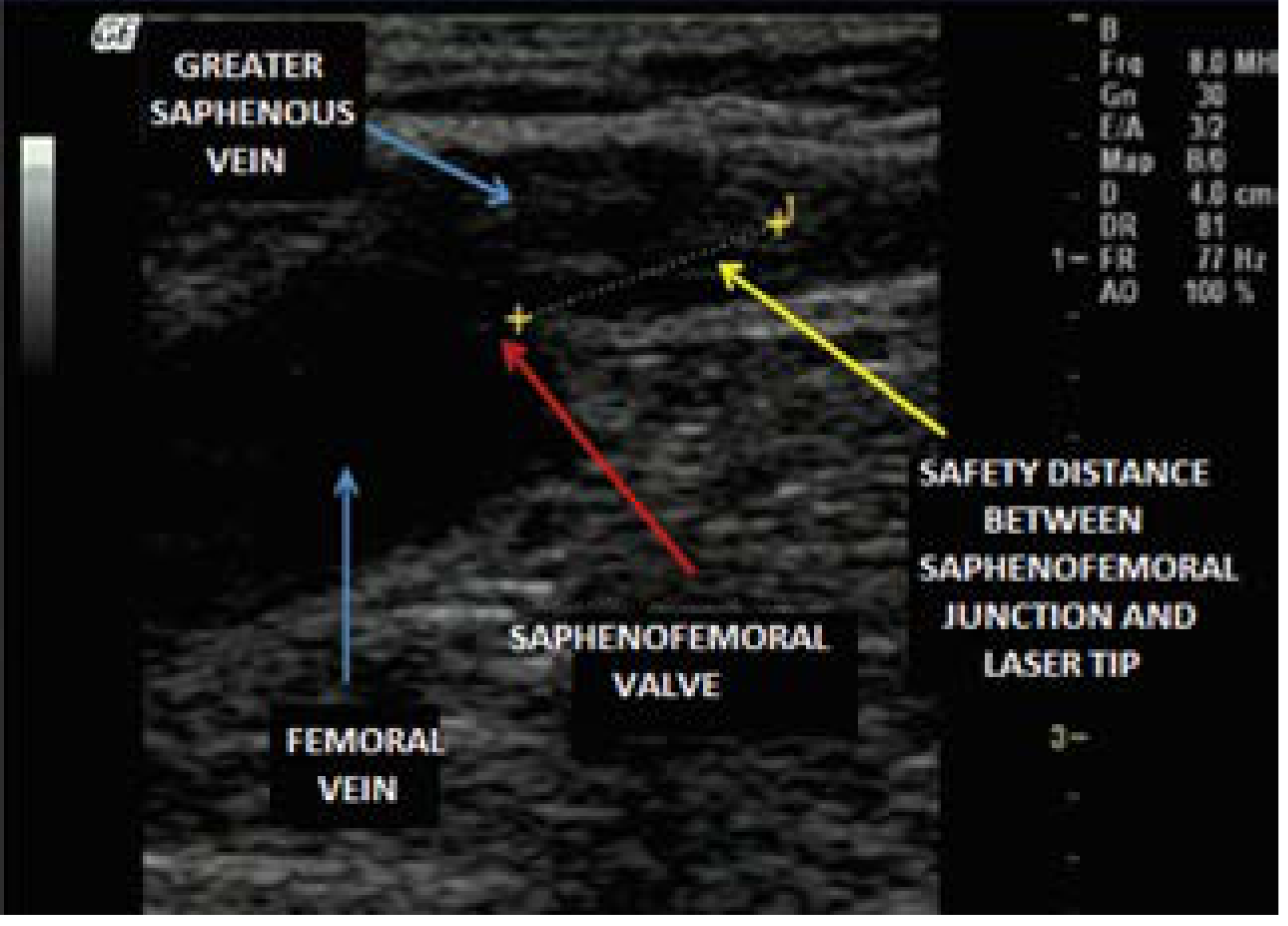
Endovenous laser fiber positioned at the saphenofemoral junction under ultrasound guidance (Current Surgical Therapy, 14e)
Post-procedure care (both RFA and EVLA):
- Duplex ultrasound at 2–5 days to confirm GSV ablation and exclude DVT/EHIT
- Compression stocking applied immediately and continued
EVTA vs. Open Surgery: Both equally effective; EVTA offers more rapid postprocedure recovery, less bruising, and lower complication rates.
— Current Surgical Therapy, 14e; Sabiston Textbook of Surgery
7D. Nonthermal Endovenous Techniques
These require no tumescent anesthesia (key advantage in clinic settings):
| Technique | Mechanism |
|---|---|
| MOCA (Mechanochemical Ablation — ClariVein™) | Rotating wire causes endothelial disruption + simultaneous sclerosant infusion |
| CAC (Cyanoacrylate Adhesive Closure — VenaSeal™) | Proprietary cyanoacrylate glue injected into vein lumen; no heat or tumescence required |
| PEM (Polidocanol Endovenous Microfoam — Varithena™) | FDA-approved prefabricated foam; up to 15 mL/session; treats incompetent superficial veins including GSV |
All require ultrasound guidance. Early results are promising with low DVT rates.
7E. Open Surgical Management
Saphenous Vein Ligation and Stripping
Indications:
- GSV diameter >2 cm (too large for thermal ablation)
- Failed endovenous treatment
- Patient/surgeon preference
- Incompetent veins not suitable for catheter-based access
Procedure — Ligation and Stripping of GSV:
- Groin incision (medial, over SFJ)
- Identify and flush ligate the GSV at the SFJ — all tributaries divided (prevents neovascularization/recurrence)
- Small incision at medial knee or ankle
- Pass a blunt-tip catheter or invagination pin stripper from groin to knee incision
- The GSV is invaginated onto the stripper and removed
- Below-knee stripping is controversial (risk of saphenous nerve injury)

Removal of varicose veins via stab avulsions (Schwartz's Principles of Surgery, 11e)
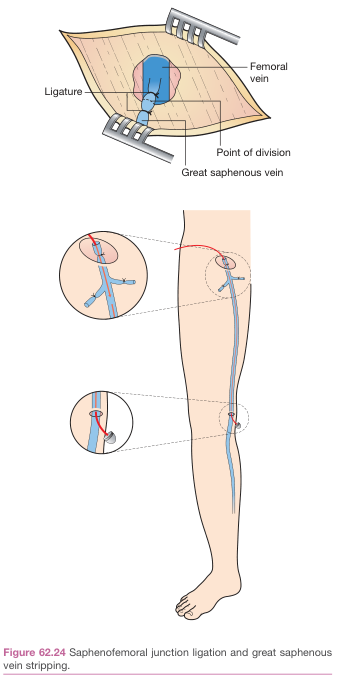
Saphenofemoral junction ligation and great saphenous vein stripping — Bailey & Love's Surgery
GSV stripping is superior to SFJ ligation alone: Lower recurrence rate and better quality of life with stripping.
Stab Avulsion Phlebectomy (Ambulatory Phlebectomy)
- Used for large tributary varicosities after axial vein treatment
- 2-mm stab incisions made directly over marked varicosities
- Vein is dissected from subcutaneous tissue and avulsed (pulled out) proximally and distally — no suture ligation required in most cases
- Bleeding controlled by leg elevation + manual compression + tumescent anesthesia
- Performed under local anesthesia; outpatient
SEPS (Subfascial Endoscopic Perforator Surgery)
- Endoscopic division of incompetent perforating veins via ports placed away from diseased skin
- Used in CEAP C4b–C6 patients with perforator incompetence
- Now largely supplanted by ultrasound-guided percutaneous perforator ablation
7F. Pre- and Post-operative Duplex Mapping
Pre-operative: Mandatory — marks the GSV/SSV, confirms reflux at SFJ/SPJ, assesses diameter, identifies anomalous anatomy, ensures patent deep system.
Post-operative: Duplex at 2–5 days post-EVTA to:
- Confirm axial vein obliteration
- Detect EHIT (Endovenous Heat-Induced Thrombus) — classified by Kabnick:
- EHIT Class 1: Thrombus in GSV only
- EHIT Class 2: Thrombus at SFJ, not entering femoral vein
- EHIT Class 3: Partial non-occlusive extension into deep vein → usually anticoagulate
- EHIT Class 4: Occlusive DVT → 3-month anticoagulation
- EHIT resolves in 7–10 days in most cases
8. Complications of Surgical/Interventional Treatment
| Complication | Associated Procedure |
|---|---|
| DVT / PE | All procedures; <1% risk per endovenous procedure |
| EHIT | Thermal ablation (RFA/EVLA) |
| Saphenous nerve injury | Below-knee GSV stripping; stab avulsions in the calf |
| Sural nerve injury | SSV stripping |
| Hematoma / ecchymosis | Stripping, phlebectomy |
| Lymphocele / lymphatic injury | Groin dissection |
| Hyperpigmentation | Sclerotherapy |
| Skin necrosis | Perivenous sclerosant extravasation |
| Recurrence / neovascularization | Incomplete SFJ ligation; missed tributaries |
| Wound infection | Open groin surgery |
9. Management of Complications — Venous Ulcer (CEAP C5/C6)
Venous leg ulcers represent the end-stage of chronic venous insufficiency. Management:
- Multilayer compression bandaging (≥40 mmHg ankle pressure) — ESVS 2022 Class I recommendation
- Wound care and dressings
- Treat underlying superficial reflux (ablation improves ulcer healing and reduces recurrence)
- Compression stockings lifelong after healing
10. Special Surgical Scenarios
Recurrent Varicose Veins (CEAP C2r)
- Most common cause: neovascularization at the SFJ or missed tributaries at initial surgery
- Re-do surgery in groin is hazardous (lymphatic and nerve injury risk)
- Foam sclerotherapy or EVTA preferred for recurrence
- Always re-map with duplex before re-intervention
Varicose Veins in Pregnancy
- Conservative management (ECS) for duration of pregnancy
- Majority improve postpartum — defer definitive treatment for 3–6 months post-delivery
- Intervention only if thrombophlebitis, ulceration, or severe symptoms
Bleeding Varicose Vein (Emergency)
- Leg elevation is the single most effective emergency maneuver
- Direct firm pressure
- Rarely requires emergency surgery; consider injection sclerotherapy under elective conditions once bleeding controlled
11. Summary: Treatment Algorithm
Varicose Veins (Symptomatic)
|
▼
Duplex Ultrasonography
|
┌───┴────────────────────────┐
│ │
Deep venous disease? Superficial reflux only
(post-thrombotic) (GSV/SSV)
│ │
Conservative ▼
+ treat CEAP C1: Sclerotherapy /
underlying DVT transcutaneous laser
│
CEAP C2–C6: Endovenous ablation
(EVTA = RFA or EVLA) — preferred
│
Adjunct: Phlebectomy for tributaries
│
Surgical stripping (GSV >2 cm or failed EVTA)
│
Compression therapy lifelong
Sources: Schwartz's Principles of Surgery 11e | Current Surgical Therapy 14e | Sabiston Textbook of Surgery | Bailey & Love's Short Practice of Surgery 28e
This is a shared conversation. Sign in to Orris to start your own chat.