Describe diagnostic techniques in surgery with ct cray mri use biopsy with principle indications and contraindications
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I've now exhausted my query_library_db budget. I have enough textbook content from Pye's Surgical Handicraft and Fischer's Surgery to write a thorough answer. Let me now compile a comprehensive response drawing on my medical knowledge and the textbook content retrieved.
Diagnostic Techniques in Surgery
Overview
Surgery relies on a hierarchy of diagnostic tools - from non-invasive imaging to tissue sampling - to confirm diagnoses, plan operations, and monitor outcomes. The major modalities are:
- Plain X-ray (radiography)
- Ultrasound (US)
- Computed Tomography (CT)
- Magnetic Resonance Imaging (MRI)
- Biopsy (tissue diagnosis)
1. Computed Tomography (CT Scan)
Principle
CT uses a rotating X-ray tube and detector array to acquire multiple cross-sectional images. A computer reconstructs these into axial, coronal, and sagittal planes. IV contrast (iodinated) highlights vascular structures and enhances lesion detection. Oral/rectal contrast helps define bowel.
Surgical Indications
| System | Indication |
|---|---|
| Abdomen/Pelvis | Acute abdomen, intra-abdominal abscess, appendicitis, diverticulitis, bowel obstruction, peritonitis workup |
| Trauma | Solid organ injury (liver, spleen, kidney), aortic injury, pneumothorax, haemothorax |
| Oncology | Staging of GI, urological, thoracic, and head/neck tumors; lymph node assessment |
| Vascular | Aortic aneurysm (CT angiography), mesenteric ischaemia |
| Thorax | Pulmonary embolism (CTPA), mediastinal masses |
| Head/Neck | Parapharyngeal abscess, cervical lymphadenopathy |
| Orthopaedics | Fracture characterization, 3D reconstruction for preoperative planning |
As noted in Fischer's Mastery of Surgery: "cross-sectional imaging with a computed tomography (CT) scan is extremely helpful as a guide to operative intervention" - particularly in complicated intra-abdominal sepsis. CT should be obtained with venous-phase IV contrast; enteral contrast is considered when perforation of the foregut or hindgut is suspected.
Advantages
- Fast (seconds for whole-body scan)
- Widely available, 24/7 in emergency settings
- Excellent bone and vascular detail
- Guides interventional drainage (CT-guided drainage of abscesses)
- 3D reconstructions aid complex fracture planning
Contraindications
| Contraindication | Reason |
|---|---|
| Contrast allergy (iodine) | Risk of anaphylaxis; premedication or non-contrast CT used |
| Renal impairment (eGFR <30 mL/min) | Contrast-induced nephropathy |
| Pregnancy | Ionizing radiation - teratogenic risk, especially in first trimester |
| Unstable patient | Time delay may worsen outcome; proceed to surgery directly if diffuse peritonitis is obvious |
2. Magnetic Resonance Imaging (MRI)
Principle
MRI uses a powerful magnetic field and radiofrequency pulses to excite hydrogen protons in body tissues. Different tissues have different T1 and T2 relaxation times, producing image contrast without ionizing radiation. Gadolinium-based contrast agents are used for vascular and lesion enhancement.
Surgical Indications
| System | Indication |
|---|---|
| Hepatobiliary | Liver lesion characterization, cholangiocarcinoma (MRCP), biliary strictures |
| Colorectal | MRI rectum for rectal cancer staging (CRM, mesorectal fascia), fistula-in-ano mapping |
| Soft Tissue/Sarcoma | Characterization and resection planning of soft tissue tumors |
| Spine | Disc prolapse, spinal cord compression, preoperative planning for spinal surgery |
| Breast | Occult breast cancer, implant assessment, biopsy guidance |
| Vascular surgery | Cardiac anatomy, aortic coarctation: "cross-sectional imaging with MRI or CT has become essential to define the aortic, coronary, and pulmonary arterial anatomy prior to surgical repair" (Mulholland & Greenfield's Surgery) |
| Brain/neurosurgery | Tumor localization, epilepsy surgery planning, functional MRI |
| Musculoskeletal | Soft tissue tumors, ligament/tendon injury, avascular necrosis |
Advantages
- No ionizing radiation - safe in young patients and for repeated scans
- Superior soft tissue contrast compared to CT
- Multiplanar imaging without repositioning
- Does not require iodinated contrast (gadolinium used instead)
Contraindications
| Contraindication | Reason |
|---|---|
| Ferromagnetic metallic implants (pacemakers, cochlear implants, some aneurysm clips) | Risk of device malfunction, displacement, or heating |
| Claustrophobia | Patient cannot tolerate enclosed bore (open MRI or sedation used) |
| First trimester of pregnancy | Theoretical risk (acoustic noise, RF heating); avoided unless benefits outweigh risks |
| Gadolinium contrast in severe renal failure (eGFR <15) | Risk of nephrogenic systemic fibrosis (NSF) |
| Intraocular metallic foreign bodies | Risk of migration causing blindness |
| Agitated, uncooperative patients | Motion degrades images severely |
3. Biopsy
Principle
Biopsy is the removal of tissue (or cells) from a living body for histological or cytological examination. It provides definitive tissue diagnosis - the "gold standard" for most neoplasms and inflammatory conditions.
Types of Biopsy
| Type | Technique | Use |
|---|---|---|
| Excision biopsy | Complete surgical removal of the lesion | Small lesions (e.g. polyps, lymph nodes, skin lesions) |
| Incision biopsy | Partial surgical removal from the edge of a lesion | Large lesions, soft tissue masses |
| Core needle biopsy (Tru-Cut) | Large-bore cutting needle removes a tissue core | Breast, liver, kidney, prostate, soft tissue |
| Fine needle aspiration cytology (FNAC) | Aspirates cells (not tissue cores) via a fine needle | Thyroid, salivary gland, lymph node, breast |
| Punch biopsy | Circular cutting instrument removes a disc of tissue | Skin lesions |
| Endoscopic biopsy | Forceps passed through endoscope | GI tract mucosa (colonoscopy, gastroscopy) |
| Stereotactic/CT-guided biopsy | Image-guided needle biopsy | Brain lesions, deep-seated masses |
| Bone marrow biopsy (trephine) | Core from posterior iliac crest | Haematological malignancy staging |
Key Principles (from Pye's Surgical Handicraft)
- For suspected carcinoma on sigmoidoscopy: biopsy should be taken from the edge of the lesion using large cusp forceps
- A partial biopsy of a polyp should be avoided because:
- The pathologist may have insufficient material to assess invasion through the muscularis mucosae (the criterion of malignancy)
- It may subsequently be difficult to locate the lesion for complete removal
- Polyps should therefore be removed by complete excision biopsy
- After biopsy: the site must be inspected for bleeding
- A barium enema should not be performed within 10 days of a biopsy owing to the risk of perforation
Indications for Biopsy
- Suspected malignancy - to confirm diagnosis before treatment
- Characterization of inflammatory/granulomatous disease (TB, sarcoidosis, Crohn's)
- Lymphadenopathy of unknown cause
- Suspicious breast lump, thyroid nodule, or skin lesion
- Renal or hepatic parenchymal disease (interstitial nephritis, cirrhosis staging)
- Monitoring treatment response in known malignancy
- Suspected soft tissue sarcoma - mandatory before definitive surgery
- Bone tumors - core or incisional biopsy before limb-salvage surgery
Contraindications to Biopsy
Absolute:
- Uncooperative patient (no safe positioning possible)
- Suspicion of a vascular lesion / AV malformation without vascular imaging
- Suspected hydatid cyst (risk of anaphylaxis from cyst fluid spillage)
- No consent
Relative:
- Anticoagulant therapy or clotting disorders - risk of uncontrolled bleeding (as specifically noted in Pye's Surgical Handicraft: "a biopsy is contraindicated in patients on anticoagulants or with clotting disorders")
- Thrombocytopenia (platelets <50,000/mm3 for core biopsy)
- Overlying infection at the biopsy site (risk of seeding)
- Renal biopsy: solitary kidney (relative), uncontrolled hypertension, hydronephrosis
- Inaccessible site where procedure risk exceeds diagnostic benefit
- Suspected melanoma: incision biopsy is contraindicated (excision biopsy only, to avoid lymphatic dissemination)
4. Comparison Summary Table
| Feature | CT | MRI | Biopsy |
|---|---|---|---|
| Ionizing radiation | Yes | No | No |
| Speed | Fast (minutes) | Slow (30-60 min) | Variable |
| Cost | Moderate | High | Low to moderate |
| Soft tissue contrast | Good | Excellent | N/A (histology) |
| Tissue diagnosis | No | No | Yes (definitive) |
| Guided intervention | CT-guided drainage/biopsy | MRI-guided biopsy | Technique itself |
| Key contraindication | Contrast allergy, renal failure, pregnancy | Metal implants, severe renal failure (Gd) | Anticoagulation, bleeding disorder |
5. Clinical Decision Framework
- Emergency (trauma / acute abdomen): CT is first-line when patient is stable; proceed directly to surgery if obvious diffuse peritonitis exists.
- Tumor staging/characterization: CT for initial staging; MRI for local staging (rectal cancer, liver lesions, sarcoma).
- Definitive tissue diagnosis: Biopsy is mandatory before chemoradiotherapy or major oncological resection.
- Pregnant patient: Avoid CT if possible; ultrasound or MRI preferred.
- Renal failure: Avoid iodinated CT contrast; MRI with gadolinium also risky below eGFR 15; use non-contrast modalities or US.
Sources: Pye's Surgical Handicraft, 22nd Ed. | Fischer's Mastery of Surgery, 8th Ed. | Mulholland & Greenfield's Surgery, 7th Ed. | Bailey & Love's Short Practice of Surgery, 28th Ed.
X ray
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have rich textbook content and images. Let me compile the comprehensive answer on X-ray as a diagnostic technique in surgery.
X-Ray (Plain Radiography) as a Diagnostic Technique in Surgery
Principle
X-rays are a form of electromagnetic radiation (wavelength 0.01–10 nm) that pass through the body and are differentially absorbed by tissues based on their density. The resulting image shows five basic radiographic densities:
| Density | Appearance on X-ray | Examples |
|---|---|---|
| Gas/Air | Black (radiolucent) | Bowel gas, pneumothorax, free air |
| Fat | Dark grey | Retroperitoneal fat planes |
| Soft tissue/Water | Grey | Muscle, liver, blood, fluid |
| Bone/Calcium | White (radiopaque) | Bones, calculi, calcifications |
| Metal | Bright white | Surgical implants, foreign bodies |
The X-ray tube emits a beam that passes through the patient and strikes a detector or film plate. Standard views are:
- PA (postero-anterior) - chest
- AP (antero-posterior) - abdomen, trauma
- Lateral - spine, chest, foreign bodies
- Erect - chest and abdomen to detect free gas and fluid levels
- Supine - abdomen (AXR)
Standard Views and Their Surgical Uses
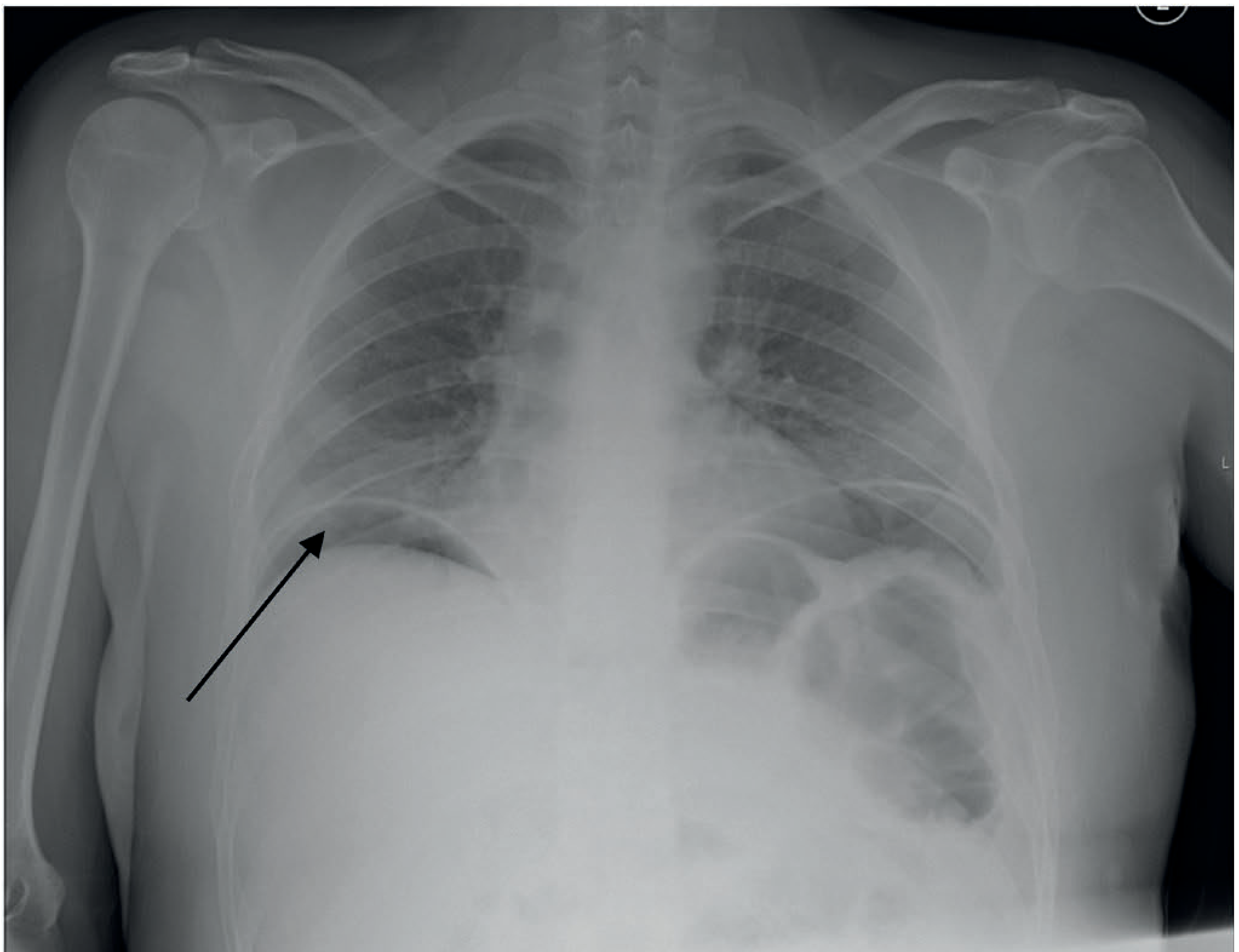
1. Erect Chest X-ray (CXR)
The erect CXR is the ideal first test for hollow organ perforation (Bailey & Love's Surgery, 28th ed). As little as 10-20 mL of free air can be detected as a crescent of gas under the diaphragm.
Technique points (from Bailey & Love's):
- Allow ~10 minutes after sitting the patient upright before taking the film so air can rise
- Seek free air under the right hemidiaphragm (to avoid confusion with left-sided gastric air bubble)
- Recognize Chilaiditi's syndrome - harmless asymptomatic interposition of large bowel between liver and diaphragm - as a mimic
- Postoperative free air can persist for up to 5-7 days - interpret with caution
- If CXR is equivocal or walled-off perforation is suspected, CT is the next step
2. Plain Abdominal Radiograph (AXR)
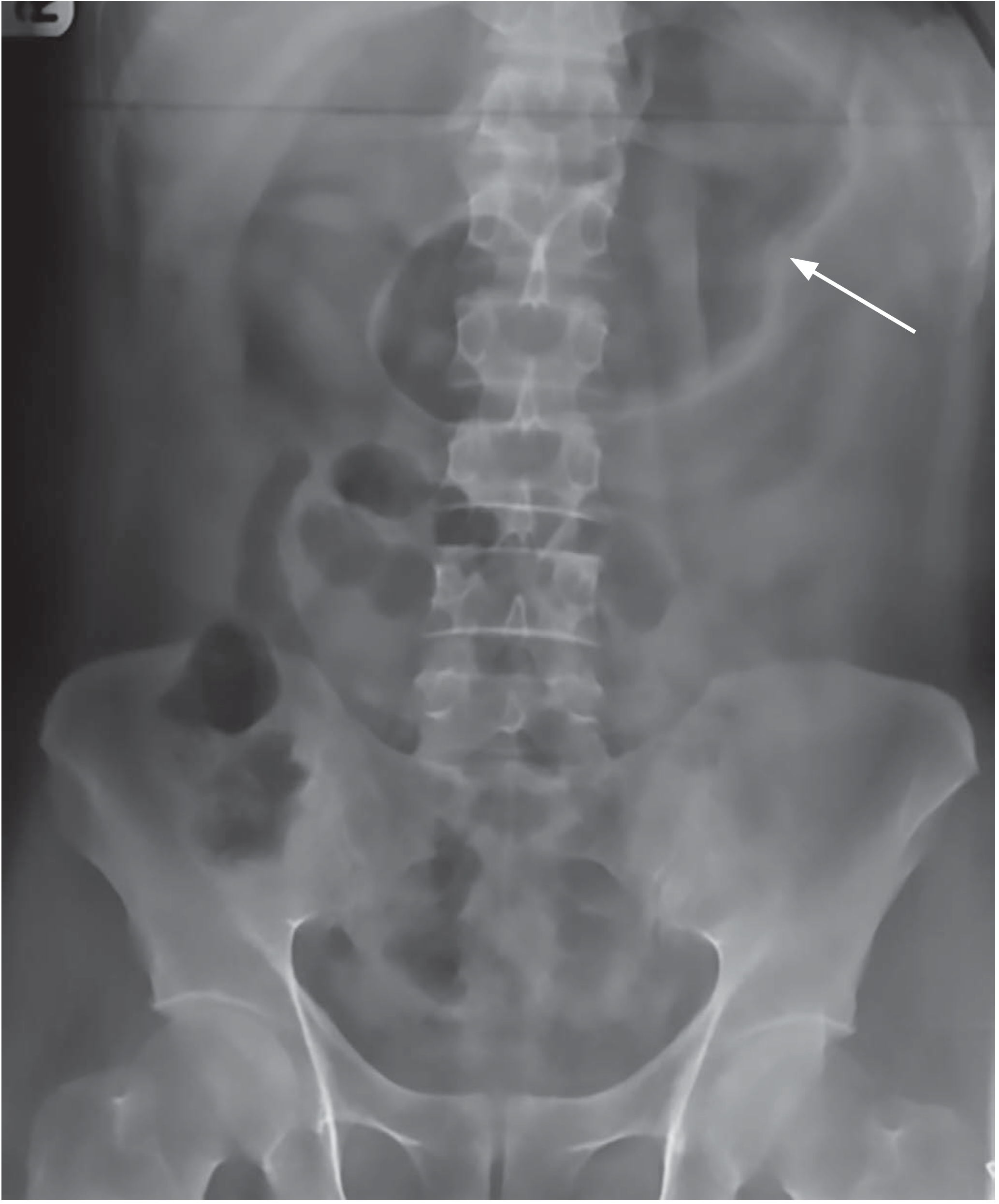
Rigler's Sign: Gas is visible on both sides of the bowel wall - indicates free intraperitoneal gas (perforation).
Surgical Indications for X-ray
A. Acute Abdomen
| Finding | Sign | Condition |
|---|---|---|
| Free gas under diaphragm | Subdiaphragmatic air (erect CXR) | Perforated hollow viscus |
| Rigler's sign | Gas on both sides of bowel wall | Perforation (when cannot sit erect) |
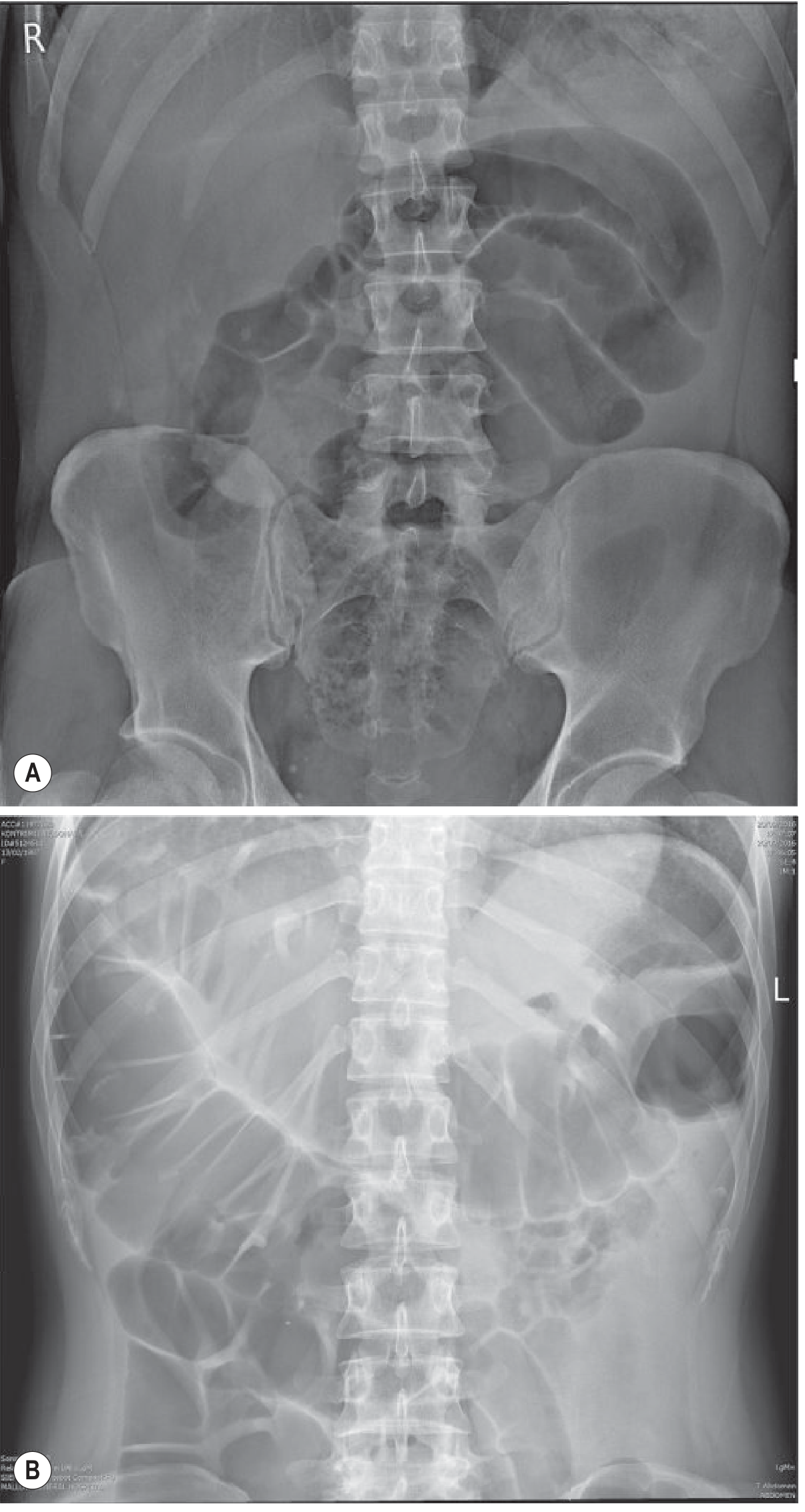
| Dilated central bowel loops + valvulae conniventes | Small bowel obstruction pattern | SBO |
| Dilated peripheral loops + haustral markings | Large bowel obstruction pattern | LBO |
| "String of beads" sign | Line of gas bubbles between valvulae | SBO, near-complete fluid fill |
| Calcified appendicolith | Calcification in right iliac fossa | Appendicitis |
| Sentinel loop | Localized ileus | Adjacent inflammation (pancreatitis) |
| Ground glass opacity | Loss of normal psoas shadow | Free peritoneal fluid |
Differentiating small vs. large bowel on AXR (from Grainger & Allison / Bailey & Love):
| Feature | Small Bowel | Large Bowel |
|---|---|---|
| Position | Central | Peripheral |
| Folds | Valvulae conniventes (cross entire lumen) | Haustra (partial folds) |
| Diameter (when obstructed) | 3.5-5 cm | 5-8 cm (caecum up to 9 cm) |
A normal plain radiograph does not exclude bowel obstruction - if clinical concern persists, CT is indicated.
B. Trauma
- CXR in trauma: detect pneumothorax, haemothorax, rib fractures, widened mediastinum (aortic injury), diaphragmatic hernia
- Pelvic X-ray: pelvic ring disruption, acetabular fractures
- Limb X-rays: fractures, dislocations, foreign bodies
- Cervical spine X-ray: C-spine injury in trauma (now largely replaced by CT)
C. Orthopaedics
- Initial assessment of all suspected fractures
- Two views at 90° to each other are mandatory (AP + lateral) - a fracture visible only in one plane will be missed on a single view
- Two joints should be included for long-bone fractures (to exclude associated dislocation)
- Comparison views of opposite limb in children (to differentiate growth plates from fractures)
- Post-reduction and post-fixation assessment
- Monitoring of fracture healing - callus formation, union
D. Chest (General Surgery & Preoperative)
- Preoperative assessment for cardiorespiratory disease
- Lung cancer screening (though CT low-dose is now preferred)
- Pleural effusion, pulmonary collapse, pneumonia
- Mediastinal shift, widening
- Diaphragmatic hernia: bowel loops visible in chest
E. Urology
- KUB (Kidney-Ureter-Bladder) film: detect radio-opaque renal/ureteric calculi (80-90% of stones are radio-opaque)
- Bladder calculi
- Note: uric acid stones are radiolucent - missed on plain X-ray, require CT/IVU
F. Vascular Surgery
- Calcified aortic aneurysm outline on AXR (eggshell calcification)
- Foreign bodies/embolized stents
G. Swallowed/Inhaled Foreign Bodies
- CXR for inhaled foreign bodies
- Neck + chest X-ray for oesophageal foreign bodies
- Abdominal series to track ingested objects through GI tract
Special X-ray Techniques in Surgery
| Technique | Description | Use |
|---|---|---|
| Contrast studies | Barium/Gastrografin swallow, meal, enema | Bowel obstruction, leak, fistula |
| Gastrografin follow-through | Water-soluble contrast (osmotic effect) | Suspected SBO - also therapeutic; monitors contrast reaching colon |
| Fluoroscopy | Real-time X-ray | Intraoperative cholangiography, joint manipulation |
| Intraoperative X-ray / C-arm | Portable image intensifier | Fracture reduction, nail/plate positioning, foreign body localization |
Contraindications
Absolute
- None that are absolute in a true emergency (life-saving benefit outweighs risk)
Relative / Important Considerations
| Contraindication | Reason | Alternative |
|---|---|---|
| Pregnancy (especially 1st trimester) | Ionizing radiation is teratogenic; risk highest to fetus in organogenesis (3-8 weeks) | Ultrasound or MRI if possible; X-ray only if clinically essential |
| Repeated exposures in children | Higher lifetime risk of radiation-induced malignancy (growing tissues more sensitive) | Ultrasound preferred (e.g., appendicitis in children) |
| Reproductive organs in young patients | Gonadal irradiation - reproductive risk | Use gonadal shielding; minimize views |
| Allergy to contrast agents | Applies to contrast studies only | Gadolinium-based contrast (MRI) or non-contrast CT |
| Renal failure | Applies to contrast studies (iodinated/barium) | Non-contrast imaging |
Key radiation dose reference (approximate):
- CXR = 0.1 mSv (equivalent to ~10 days natural background radiation)
- AXR = 0.7 mSv
- CT abdomen = 8-10 mSv (much higher - a major reason to prefer X-ray for initial assessment)
Limitations of Plain X-ray in Surgery
- Low sensitivity for early/subtle findings - e.g., a normal AXR does not exclude SBO if loops are fluid-filled
- Limited soft tissue contrast - CT and MRI are far superior for organ detail
- No vascular information without contrast
- 2D image - overlapping structures cause confusion; CT provides true cross-sectional anatomy
- Operator/viewer dependent - requires experienced interpretation
- Ionizing radiation - cumulative exposure is a concern
Summary
Plain X-ray is the fastest, most available, and cheapest first-line imaging modality in surgical emergencies. Its most valuable surgical roles are:
- Erect CXR for free gas in perforation
- AXR for bowel obstruction
- Bone X-rays for fractures
- KUB for radio-opaque urinary stones
- Preoperative CXR for cardiopulmonary assessment
A normal plain X-ray never definitively excludes serious pathology - clinical judgement must prevail, and CT is the modality of choice for further evaluation when X-ray is equivocal.
Sources: Bailey & Love's Short Practice of Surgery, 28th ed. | Grainger & Allison's Diagnostic Radiology | Fischer's Mastery of Surgery, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.