In reference of bailey and love and s das compare pain , vomiting, fever, decubitus of appendicitis, pancreatitis, cholecystitis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have sufficient information from both Bailey & Love and S. Das for all three conditions. Let me compile the comprehensive comparison table.
Here is a detailed comparison of Acute Appendicitis, Acute Pancreatitis, and Acute Cholecystitis across four clinical parameters - pain, vomiting, fever, and decubitus (position of comfort) - as described in Bailey & Love's Short Practice of Surgery (28th Ed.) and S. Das's A Manual on Clinical Surgery (13th Ed.).
Comparison: Appendicitis vs. Pancreatitis vs. Cholecystitis
1. PAIN
| Feature | Acute Appendicitis | Acute Pancreatitis | Acute Cholecystitis |
|---|---|---|---|
| Onset | Gradual (catarrhal) or sudden (obstructive) | Rapid, reaching maximum intensity within minutes | Sudden, often nocturnal onset |
| Initial character | Visceral - periumbilical colic (central/midline) regardless of appendix position (as midgut is a median organ - S. Das) | Severe, constant, refractory to usual analgesic doses | Dull, continuous, severe - "colicky" but not truly colicky |
| Progression | Shifts and localises to right iliac fossa (RIF) as parietal peritoneum becomes irritated | Remains epigastric but may spread diffusely; sometimes localises to either upper quadrant | Localises to right upper quadrant (RUQ) or epigastric region |
| Radiation | None typical; pelvic appendix causes suprapubic pain + tenesmus; retrocaecal causes right flank/posterior pain | To the back in ~50%; relief by leaning forward; can radiate to chest (mimicking MI/pneumonia) | Radiates to the back or right shoulder tip |
| Aggravation | Coughing, sudden movement exacerbate RIF pain | Movement; no specific relief position gives consistent benefit | Movement; fatty food intake can precipitate/worsen episodes |
| Notes | Classic visceral-somatic sequence present in only ~50% (Bailey & Love). Non-obstructive: dull aching; obstructive: colicky (S. Das) | Can mimic most causes of the acute abdomen (Bailey & Love). The suddenness may simulate perforated peptic ulcer | Worsened by deep inspiration during palpation in right subcostal region - Murphy's sign (Bailey & Love) |
2. VOMITING
| Feature | Acute Appendicitis | Acute Pancreatitis | Acute Cholecystitis |
|---|---|---|---|
| Occurrence | Nausea and vomiting present; in obstructive type vomiting is common and early | Nausea, repeated vomiting and retching - usually marked | Present, with associated nausea |
| Severity | Moderate; related to degree of appendix distension (S. Das) | Severe, persistent retching that may continue even with an empty stomach / nasogastric aspiration (Bailey & Love) | Moderate; associated with biliary pain episodes |
| Relation to pain | Follows pain - S. Das emphasises "Pain → Vomiting → Fever" (Murphy's syndrome) | Accompanies pain from early on; hiccoughs also troublesome | Accompanies pain; food - especially fatty food - can trigger both |
| Notes | In catarrhal appendicitis: nausea/vomiting accompany discomfort. In obstructive appendicitis: sudden severe vomiting (S. Das) | Hiccoughs due to gastric distension or diaphragmatic irritation. NGT aspiration may not relieve retching (Bailey & Love) | Dislike for fatty foods is characteristic of gallbladder disease (S. Das: "qualitative dyspepsia") |
3. FEVER
| Feature | Acute Appendicitis | Acute Pancreatitis | Acute Cholecystitis |
|---|---|---|---|
| Timing | Comes last in the sequence (after pain and vomiting) - Murphy's syndrome (S. Das) | Initially body temperature may be normal or even subnormal; rises as inflammation develops (Bailey & Love) | Develops with acute cholecystitis; fever moderate in degree (S. Das) |
| Degree | Mild pyrexia 37.2-37.7°C in early stages; 20% of patients show no pyrexia initially (Bailey & Love). Quite high in children (S. Das). Temperature >38.5°C in children suggests other causes such as mesenteric adenitis (Bailey & Love) | Temperature part of SIRS criteria (>38°C or <36°C). Swinging pyrexia suggests cholangitis complicating gallstone pancreatitis (Bailey & Love) | Raised to a moderate degree - less dramatic than appendicitis in children (S. Das). Fever is a systemic sign in Tokyo Guidelines diagnostic criteria for acute cholecystitis (Bailey & Love) |
| Sequence | Pain → Vomiting → Fever last (Murphy's syndrome - S. Das) | Fever is not an early cardinal feature; part of SIRS; "never an early sign" in acute conditions (S. Das principle) | Fever moderate, part of systemic inflammatory response; accompanies local RUQ signs |
| Notes | After perforation: initially pain subsides temporarily, then peritonitis ensues with subnormal temperature and rising pulse (S. Das) | Cyanosis may be visible in haemorrhagic pancreatitis. Mild icterus seen in gallstone pancreatitis (Bailey & Love) | Intermittent fever (Charcot's triad: fever + rigor + jaundice) suggests calculus in common bile duct, not simple cholecystitis (S. Das) |
4. DECUBITUS (Position of Comfort / Posture)
| Feature | Acute Appendicitis | Acute Pancreatitis | Acute Cholecystitis |
|---|---|---|---|
| Preferred position | Patient lies still, typically on back or slightly flexed on the right side; reluctant to move as movement exacerbates pain | Patient may gain relief by sitting up or leaning forwards - reduces traction on inflamed retroperitoneal pancreas (Bailey & Love) | Patient lies still (movement worsens pain); no specific relief posture documented |
| Movements | Avoids movement; coughing or sudden movement exacerbates RIF pain (Bailey & Love) | Restless due to severity; leaning forward or assuming the knee-chest position may reduce pain | Avoids deep inspiration (Murphy's sign is based on this - pain on inspiring during RUQ palpation) |
| Abdominal wall | Guarding and rebound tenderness over RIF; hyperaesthesia in Sherren's triangle (S. Das) | Abdomen may be distended (ileus); epigastric mass may develop; tenderness with guarding | Tenderness RUQ; Murphy's sign positive; omentum may wall off gallbladder (mass palpable) |
| Notes | Retrocaecal appendicitis: pain and tenderness in right flank or posterior - patient may be rolled to the left side to elicit tenderness (S. Das) | "At the other extreme, gravely ill with profound shock, toxicity and confusion" - prostrated (Bailey & Love) | Contour of abdomen remains normal in uncomplicated cholecystitis and biliary colic (S. Das) |
Summary at a Glance
| Parameter | Appendicitis | Pancreatitis | Cholecystitis |
|---|---|---|---|
| Pain site | Periumbilical → RIF | Epigastric → diffuse | RUQ / epigastric |
| Pain radiation | None (varies by position) | Back (50%), chest | Back / right shoulder |
| Vomiting | Moderate; after pain | Severe, persistent, unrelieved by NGT | Moderate; with fatty food |
| Fever | Mild (37.2-37.7°C); last in sequence | Normal/subnormal early; rises later; SIRS | Moderate degree |
| Sequence | Pain → Vomiting → Fever (Murphy's syndrome) | Pain dominant; fever late | Pain + vomiting together; fever moderate |
| Decubitus | Lies still, reluctant to move | Leans forward / knee-chest for relief | Lies still; avoids deep inspiration |
Key teaching points from both texts:
- Murphy's syndrome (S. Das): In acute appendicitis, the invariable sequence is pain first, then vomiting, then fever. This sequence is diagnostically important.
- Pancreatitis pain is uniquely refractory to standard analgesics and is relieved (partially) by leaning forward - a posture not seen in the other two conditions (Bailey & Love).
- Cholecystitis fever is only moderate, distinguished from the higher fever of appendicitis (especially in children) and the SIRS-range fever of severe pancreatitis (S. Das).
- Vomiting is most severe and persistent in pancreatitis; it can persist despite nasogastric aspiration due to ongoing retching (Bailey & Love).
- The contour of the abdomen remains normal in biliary colic and acute cholecystitis, unlike the distension seen in pancreatitis (with ileus) (S. Das).
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed., Chapters 71 & 72 (pp. 1265-1295); S. Das, A Manual on Clinical Surgery, 13th Ed., Chapter on Inflammation/Acute Abdomen (pp. 460-490).
Create a image of human body showing peptic point and duodenal point
Generating Image
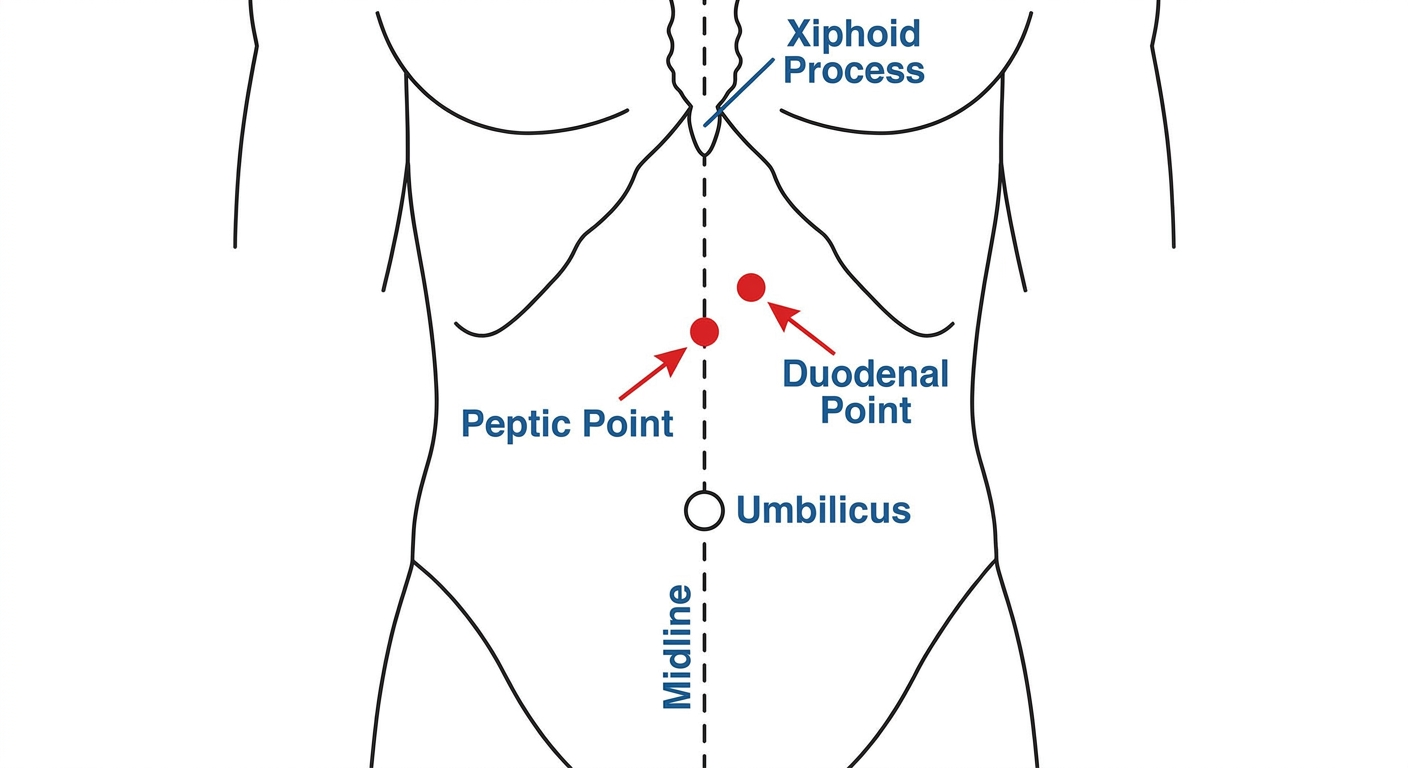
Here is the anatomical diagram showing both abdominal tender points:
-
Peptic Point - located on the midline in the epigastric region, midway between the xiphisternum and the umbilicus. Tenderness here is elicited in gastric ulcer.
-
Duodenal Point - located just to the right of the midline in the epigastric region, at roughly the same level as the peptic point. Tenderness here is characteristic of duodenal ulcer (also called the pyloroduodenal point in some texts).
Clinical note: Both points are used in the physical examination of peptic ulcer disease. In practice, the duodenal point is roughly 2-3 cm to the right of the midline at the level of the epigastrium. Deep palpation is used to elicit tenderness, and it should be done in a relaxed patient to distinguish true deep tenderness from superficial guarding.
This is a shared conversation. Sign in to Orris to start your own chat.