Cholinestearse inhibitors
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching PubMed
"cholinesterase inhibitors" AND "Alzheimer disease"
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of cholinesterase inhibitors compiled from multiple authoritative sources.
Cholinesterase Inhibitors
Mechanism of Action
Cholinesterase inhibitors (ChEIs) antagonize acetylcholinesterase (AChE) - the enzyme responsible for hydrolysing acetylcholine (ACh) at synaptic clefts. By blocking this enzyme, they raise ACh concentration at both muscarinic and nicotinic receptors throughout the body.
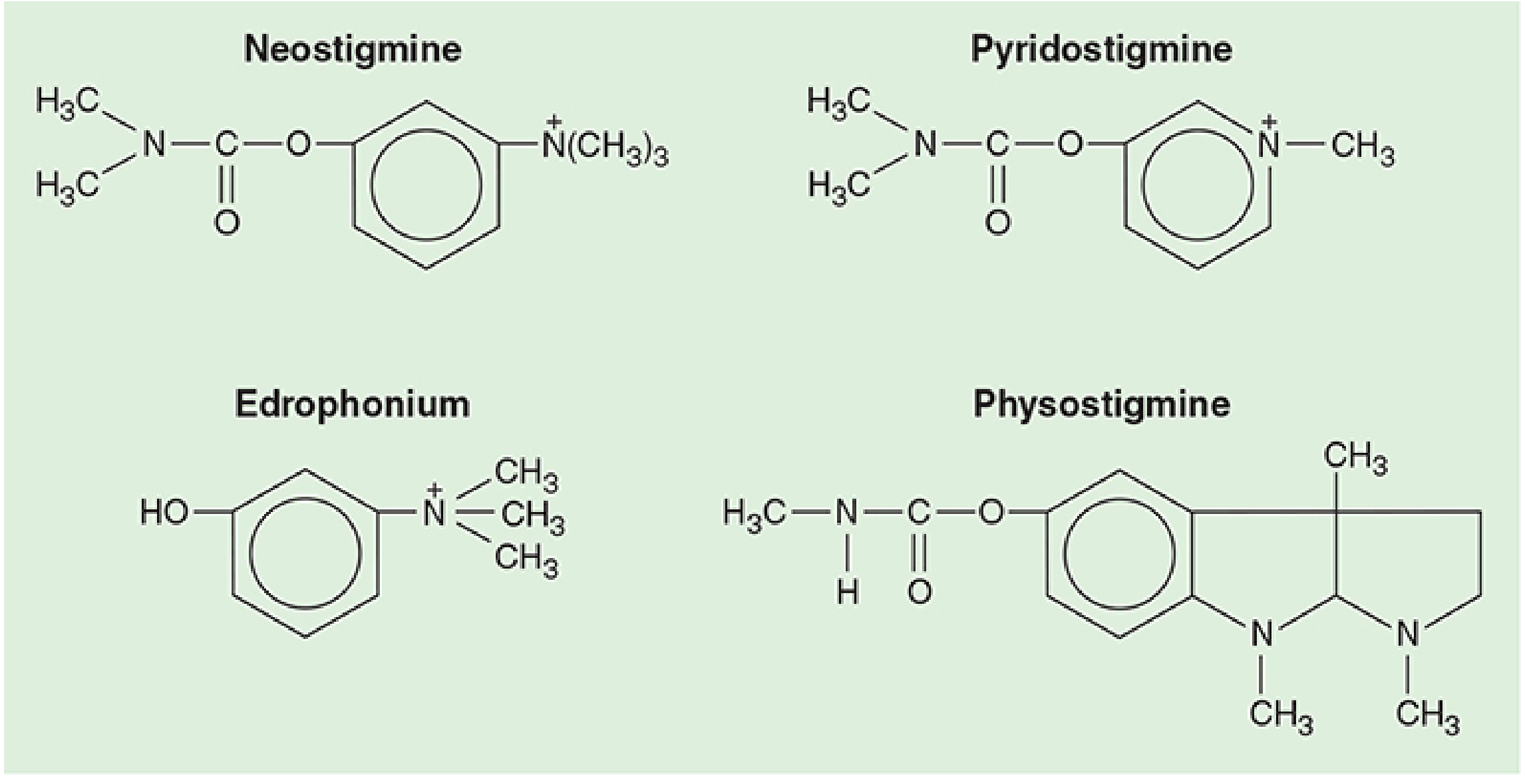
The nature of binding to the enzyme determines the duration of action:
- Edrophonium - electrostatic attraction and hydrogen bonding; short-lived interaction
- Neostigmine, pyridostigmine - covalent (carbamate) bonds; longer lasting but reversible
- Organophosphates - form stable, irreversible covalent bonds; effect persists long after the drug is cleared from circulation
Classification
1. Reversible ChEIs (Short-acting)
| Drug | Trade Name | Key Feature |
|---|---|---|
| Edrophonium | Tensilon | Electrostatic binding only; shortest duration |
| Neostigmine | Prostigmin | Carbamate bond; quaternary ammonium - does NOT cross BBB |
| Pyridostigmine | Mestinon | Carbamate bond; quaternary ammonium - does NOT cross BBB |
| Physostigmine | Eserine | Tertiary amine - crosses BBB |
2. Reversible ChEIs (for Dementia)
| Drug | Enzymes Inhibited | Mechanism | Key Feature |
|---|---|---|---|
| Donepezil | AChE only | Noncompetitive | Selective CNS; long t½ ~70 h; once daily |
| Rivastigmine | AChE + BuChE | Noncompetitive | Also inhibits butyrylcholinesterase; t½ 1 h but acts 10 h |
| Galantamine | AChE only | Competitive | Natural alkaloid from Galanthus nivalis (daffodil) |
| Tacrine | Non-selective | - | Obsolete - hepatotoxicity, 4x/day dosing |
3. Irreversible ChEIs (Organophosphates & Carbamates)
- Echothiophate - used in glaucoma (ophthalmic)
- Organophosphate pesticides (parathion, malathion) - agricultural; poisoning risk
- Nerve agents (sarin, VX, tabun) - chemical warfare; extremely toxic
Pharmacology of Individual Agents
Neostigmine
- Carbamate moiety + quaternary ammonium group - lipid insoluble, cannot cross BBB
- Dose for reversal: 0.04-0.08 mg/kg (max 5 mg adults)
- Effects apparent in 5 min, peak at 10 min, last >1 hour
- Also inhibits pseudocholinesterase (prolongs succinylcholine)
- Paired with glycopyrrolate (0.2 mg per 1 mg neostigmine) to block muscarinic side effects
Pyridostigmine
- Similar structure and mechanism to neostigmine
- Dose for reversal: 0.1-0.25 mg/kg
- Paired with glycopyrrolate (0.05 mg per mg)
- Used in myasthenia gravis (longer duration than neostigmine)
Edrophonium
- Quaternary ammonium compound; no carbamate - acts by electrostatic interaction only
- Fast onset but shorter duration than neostigmine
- Dose: 0.5-1 mg/kg
- Paired with atropine (0.014 mg per mg)
- Classic use: Tensilon test for myasthenia gravis diagnosis
Physostigmine
- Tertiary amine - crosses the blood-brain barrier (the only reversal-class ChEI that does)
- Used to reverse central anticholinergic syndrome (from atropine, scopolamine overdose)
- Dose: 0.01-0.03 mg/kg
- Not used to reverse neuromuscular blockers
- Unique: causes CNS diffuse excitation (muscarinic + nicotinic CNS stimulation)
Donepezil
- Selectively active within the CNS; minimal peripheral AChE inhibition - favorable GI side-effect profile
- Peak plasma in 3-4 hours; t½ ~70 hours in elderly
- Steady state in ~2 weeks; once-daily dosing
- Metabolized by CYP2D6 and CYP3A4
- Cirrhosis reduces clearance by ~20%
Rivastigmine
- Inhibits both AChE and butyrylcholinesterase (BuChE); BuChE is upregulated in Alzheimer disease brain
- t½ 1 hour but enzyme-bound activity lasts ~10 hours; twice-daily oral or once-daily transdermal patch
- More peripheral activity than donepezil - more GI side effects
- Metabolized by tissue esterases (not CYP - fewer drug-drug interactions)
- FDA-approved for Parkinson's disease dementia (PDD) as well
Galantamine
- AChE inhibition + allosteric modulation of nicotinic receptors (unique dual action)
- Maximum concentrations at 30 min - 2 hours; t½ ~6 hours
- Metabolized by CYP2D6 and CYP3A4
- Extracted from the daffodil Galanthus nivalis
Systemic (Muscarinic) Effects of ChEIs
When ChEIs raise ACh at muscarinic receptors throughout the body, the following effects occur (mnemonic: DUMBELS):
| System | Effect |
|---|---|
| Diarrhea, Urination | Increased GI/GU motility and secretion |
| Miosis + muscle weakness | Pupil constriction; nicotinic at NMJ |
| Bronchospasm + secretions | Bronchoconstriction, increased mucus |
| Excitation (CNS) | Agitation, seizures (physostigmine/OPs) |
| Lacrimation | Increased tear production |
| Salivation, Sweating, Seizures | Hypersecretion; CNS toxicity |
Cardiovascular: bradycardia, potential sinus arrest, fall in cardiac output.
Clinical Uses
1. Reversal of Neuromuscular Blockade (Anesthesia)
- Neostigmine, pyridostigmine, edrophonium reverse nondepolarizing NMBAs (e.g., rocuronium, vecuronium)
- They prolong depolarizing blockade (succinylcholine) - never use together
- Must co-administer an anticholinergic (glycopyrrolate or atropine) to block muscarinic side effects
- Contraindicated if no twitches are present after 50 Hz tetany for 5 seconds (blockade too deep)
- Note: sugammadex has now replaced ChEIs for reversal of rocuronium/vecuronium in many centers
2. Alzheimer's Disease and Dementia
- First-line symptomatic treatment for mild-to-moderate AD: donepezil, rivastigmine, galantamine
- Donepezil approved for all stages (mild through severe); others mild-moderate only
- Effect: modest ~6-12 month delay in progression; improvement in memory, apathy, behavioral symptoms
- Often combined with memantine (NMDA antagonist) for moderate-severe disease
- Also used in Lewy body dementia, Parkinson's disease dementia, vascular dementia, TBI
3. Myasthenia Gravis
- Pyridostigmine is the drug of choice for symptomatic management
- Increases ACh at the NMJ to compensate for reduced/blocked nicotinic receptors
- Edrophonium (Tensilon test) used diagnostically - brief reversal of weakness confirms MG
4. Glaucoma
- Echothiophate (irreversible) - reduces IOP via pupillary constriction and increased aqueous outflow
- Pilocarpine is the cholinergic agonist typically preferred now
5. Anticholinergic Overdose / Postoperative Cognitive Dysfunction
- Physostigmine reverses central anticholinergic syndrome (confusion, delirium, hyperthermia from atropine/scopolamine)
- Only ChEI that crosses the BBB
Organophosphate Toxicology
Organophosphates cause irreversible cholinesterase inhibition. This leads to massive ACh accumulation at all cholinergic synapses.
Clinical features - the DUMBELS syndrome (see above) plus nicotinic overstimulation:
- Muscle fasciculations → weakness → respiratory paralysis
- CNS: agitation, confusion, seizures, coma
- Lab: depressed RBC acetylcholinesterase and plasma butyrylcholinesterase
Treatment:
- Decontaminate (remove clothing, wash skin); protect rescue personnel
- Atropine IV (0.5-5 mg; repeated until muscarinic signs resolve) - blocks muscarinic effects only; no effect on nicotinic
- Pralidoxime (2-PAM) - reactivates AChE if given before "aging" occurs; active at both muscarinic and nicotinic sites. Dose: 1-2% solution IV over 15-30 min, then 1% infusion (200-500 mg/h)
- Respiratory support (2-PAM does not enter CNS; ventilation is often required)
- Benzodiazepines for seizures
Aging: the organophosphate-AChE complex undergoes a time-dependent stabilization that makes it resistant to 2-PAM reactivation. This is why pralidoxime must be given early.
Adverse Effects Summary
| Drug | Key Adverse Effects |
|---|---|
| Donepezil | Nausea, diarrhea (<3%), bradycardia, syncope, weight loss |
| Rivastigmine | Nausea, vomiting, dizziness, anorexia (more GI than donepezil) |
| Galantamine | Dizziness, nausea, diarrhea (mild and transient) |
| Tacrine | Hepatotoxicity (ALT↑ in 25-30%), 4x daily dosing - now obsolete |
| Neostigmine/Pyridostigmine | Bradycardia, bronchospasm, excess secretions, GI cramps |
| Physostigmine | CNS excitation, seizures if overdosed |
| Organophosphates | DUMBELS + nicotinic toxidrome, death from respiratory failure |
Drug Interactions
- All ChEIs should be used cautiously with anticholinergic drugs (antagonistic) and with drugs that slow the heart (additive bradycardia risk - e.g., beta-blockers, digoxin)
- Donepezil and galantamine: CYP2D6/3A4 inhibitors (ketoconazole, paroxetine) increase plasma levels
- Rivastigmine: metabolized by esterases - fewer CYP-based interactions
- Succinylcholine: markedly prolonged by ChEIs (via both AChE and pseudocholinesterase inhibition)
Recent Evidence
Recent systematic reviews (2024) confirm ongoing clinical relevance:
- A 2024 meta-analysis (PMID 38439609) confirmed the safety and efficacy of AChEIs in Alzheimer's disease
- A 2024 Cochrane review of galantamine (PMID 39498781) confirmed modest but consistent cognitive benefits
- A 2024 comparative meta-analysis (PMID 38640313) evaluated the comparative efficacy and safety of AD drugs including ChEIs combined with memantine
Sources: Katzung's Basic and Clinical Pharmacology 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Morgan and Mikhail's Clinical Anesthesiology 7e; Kaplan and Sadock's Synopsis of Psychiatry; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.