Nephrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material for a thorough answer. Here is the complete guide to nephrotic syndrome:
Nephrotic Syndrome
Definition
Nephrotic syndrome is defined as proteinuria >3.5 g/day (or >3.5 g/1.73 m²/day), serum albumin <3.5 g/dL, accompanied by hyperlipidemia and clinically apparent edema. These four features - heavy proteinuria, hypoalbuminemia, hyperlipidemia, and edema - constitute the classic tetrad.
- NKF Primer on Kidney Diseases, 8e, p. 190
- Brenner and Rector's The Kidney, p. 1338
Etiologies

Primary (Idiopathic) Glomerular Causes
| Disease | Key Feature | Predominant Age Group |
|---|---|---|
| Minimal Change Disease (MCD) | Foot process effacement only on EM | Children (70-90%), Adults (10-15%) |
| Focal Segmental Glomerulosclerosis (FSGS) | Focal + segmental sclerosis on LM | Adults, especially African descent (25%) |
| Membranous Nephropathy (MN) | Subepithelial deposits, PLA2R antibody | Adults (most common idiopathic cause) |
| Membranoproliferative GN | Mesangial + endocapillary hypercellularity | Young adults |
Secondary Causes
1. Infections:
- Bacterial: post-streptococcal GN, infective endocarditis, syphilis, tuberculosis, leprosy
- Viral: hepatitis B, hepatitis C, HIV, CMV, EBV
- Parasitic: malaria (especially quartan/Plasmodium malariae), schistosomiasis, toxoplasmosis
2. Systemic diseases:
- Diabetic kidney disease (most common systemic cause worldwide)
- Amyloidosis (AL and AA)
- Systemic lupus erythematosus (class V lupus nephritis)
- Henoch-Schönlein purpura
3. Drugs and chemicals:
- NSAIDs, gold, penicillamine, mercury, captopril, lithium, heroin, interferon-α, pamidronate, anabolic steroids
4. Neoplasms:
- Solid tumors (lung, colon, stomach, breast) - often associated with membranous nephropathy
- Hodgkin lymphoma - associated with MCD
5. Hereditary/Genetic:
- Congenital nephrotic syndrome (Finnish type): mutations in NPHS1 (nephrin)
- NPHS2 (podocin) mutations: early childhood FSGS, corticosteroid-resistant
- Alport syndrome
Pathophysiology
Why the Glomerular Filtration Barrier Fails
The glomerular filtration barrier normally restricts proteins by size and charge. In nephrotic syndrome, podocyte injury is the central mechanism. The three components of the barrier are:
- Fenestrated endothelium (with negative glycocalyx charge)
- Glomerular basement membrane (GBM)
- Podocytes with slit diaphragms (key proteins: nephrin, podocin, CD2AP)
Injury to podocyte foot processes - whether immune-mediated (MCD, FSGS primary), structural (secondary FSGS), or immune complex deposition (MN, lupus) - leads to proteinuria.
The Cascade: Proteinuria → Complications
Heavy Proteinuria (>3.5 g/day)
↓
Hypoalbuminemia
↓
↓ Plasma oncotic pressure → Fluid shifts to interstitium → EDEMA
↓
Two mechanisms of edema:
• Underfill: ↓ ECV → ↑ RAAS, ↑ ADH → Na/water retention
• Overfill: Primary renal Na retention → ↑ plasma vol → edema
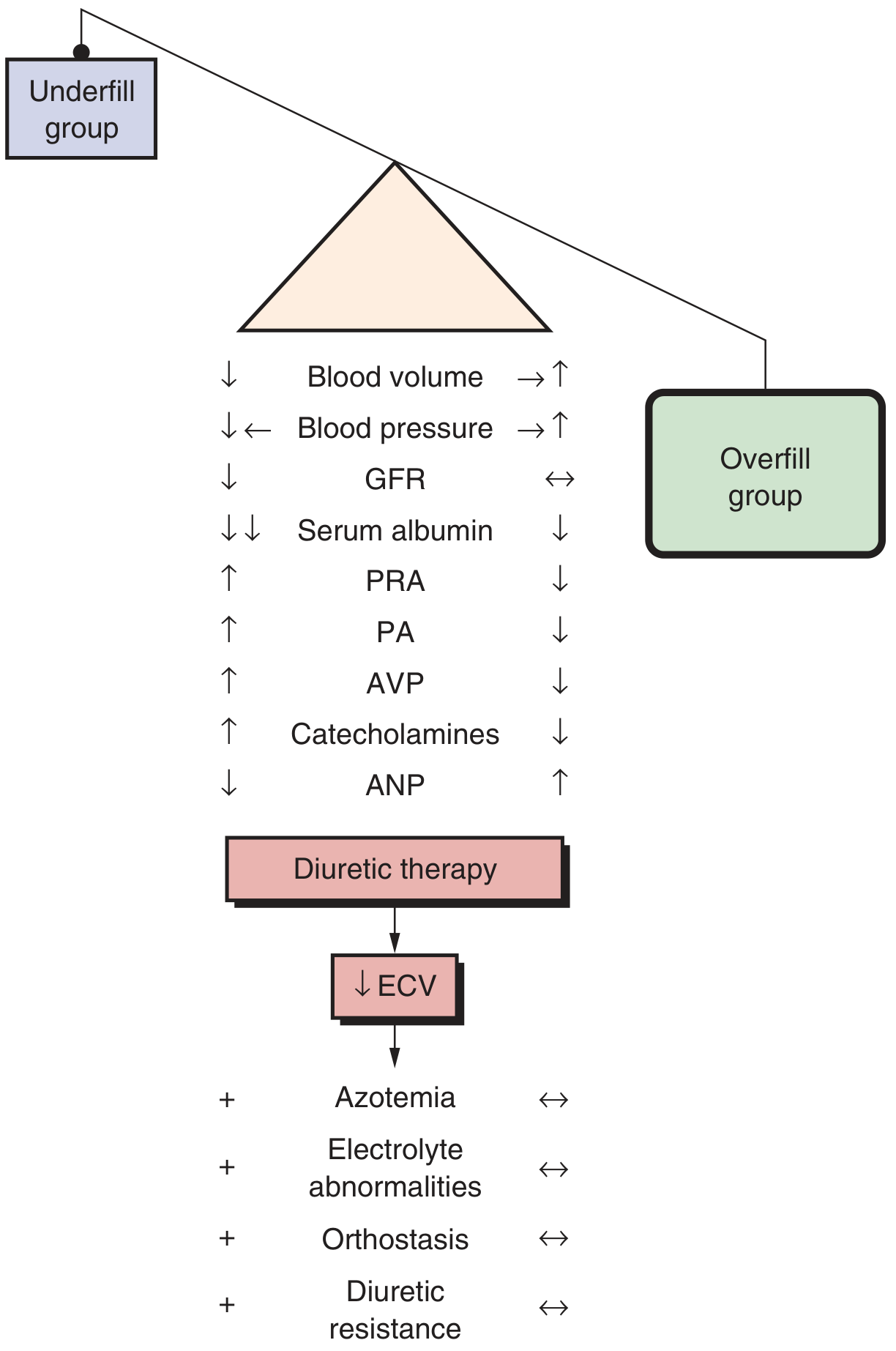
- Minimal change disease: typically underfill pattern (contracted plasma volume, stimulated RAAS)
- Other causes of NS: typically overfill pattern (expanded plasma volume, suppressed RAAS)
Hyperlipidemia
The liver compensates for low oncotic pressure by increasing lipoprotein synthesis (particularly VLDL and LDL). Decreased lipoprotein lipase activity also impairs lipid clearance. Urinary loss of HDL cholesterol shifts the ratio adversely.
Protein Losses and Their Consequences
The nephrotic kidney leaks not just albumin but many proteins, each loss generating distinct complications:
| Lost Protein | Consequence |
|---|---|
| Albumin | Hypoalbuminemia, edema |
| IgG | Hypogammaglobulinemia → susceptibility to encapsulated organisms (pneumococcus) |
| Antithrombin III, Protein C, Protein S | Hypercoagulable state → DVT, pulmonary embolism, renal vein thrombosis |
| Transferrin | Iron-deficiency anemia |
| Vitamin D-binding protein | Vitamin D deficiency, secondary hyperparathyroidism |
| Erythropoietin | Anemia |
| Complement factor B, C3 | Impaired opsonization |
| Transcortin, thyroid-binding globulin | Altered drug/hormone levels |
- Brenner and Rector's The Kidney, Box 31.2, p. 1340
Procoagulant factors are simultaneously increased: fibrinogen, factors II, V, VII, VIII, X, XIII, β-thromboglobulin, α₂-macroglobulins - Brenner and Rector's The Kidney, Box 31.3.
Renal vein thrombosis is particularly associated with membranous nephropathy and amyloidosis, and is more likely when proteinuria >10 g/day and albumin <2 g/dL.
Major Diseases - Distinguishing Features
1. Minimal Change Disease (MCD)
- Epidemiology: 70-90% of childhood NS; ~15% of adult NS
- Associations: NSAIDs, thymoma, Hodgkin lymphoma (suggesting T-cell lymphokine mechanism)
- Histology:
- Light microscopy: normal ("minimal changes")
- Immunofluorescence: negative (no immune deposits); occasionally low mesangial IgM
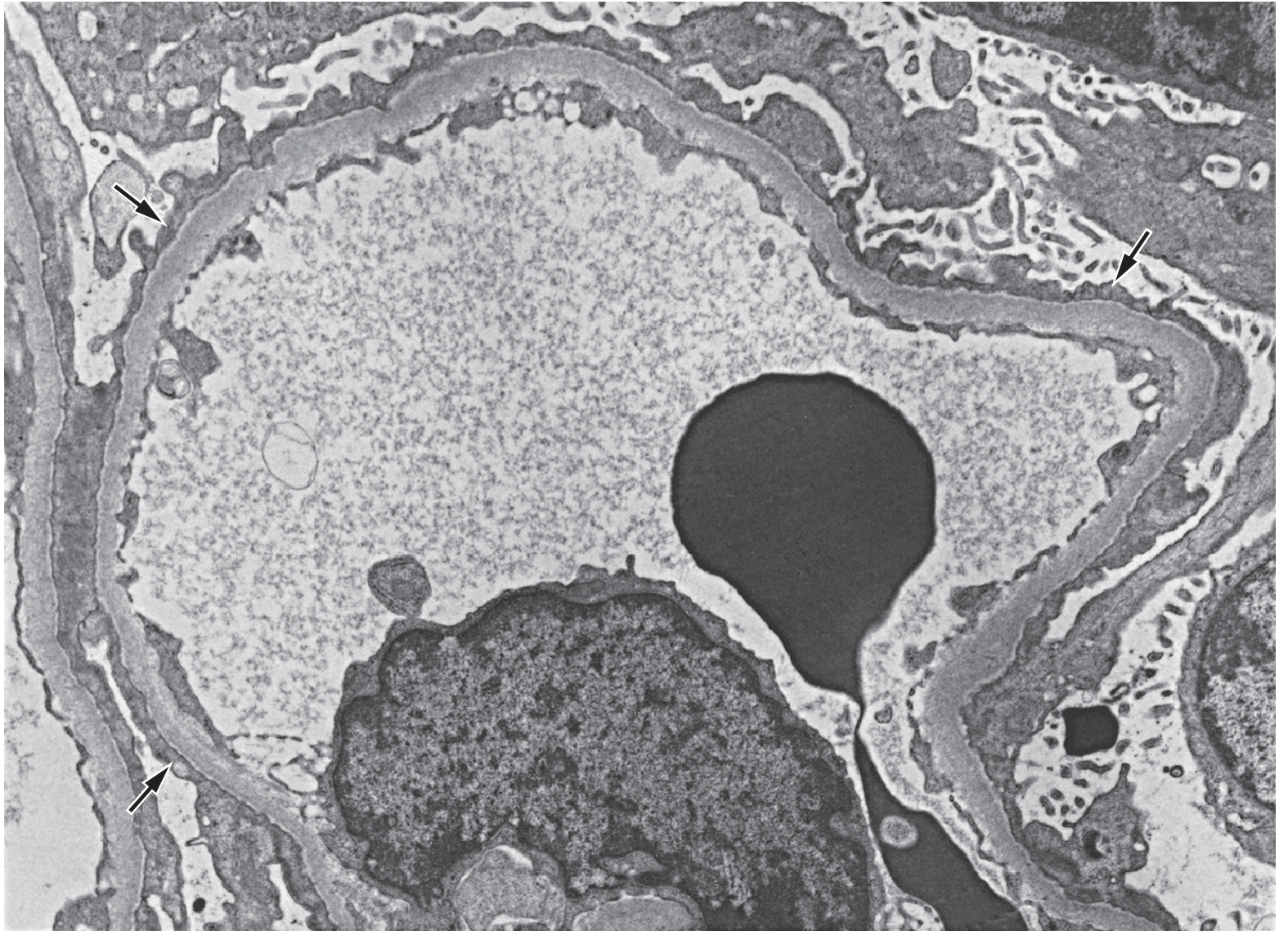
- Electron microscopy: extensive podocyte foot process effacement (the hallmark)
- Management: Corticosteroids (prednisone) are first-line. Children often diagnosed empirically (no biopsy) and treated. Anti-CD20 agents (rituximab) used for steroid-dependent/resistant cases.
- Prognosis: Generally excellent; most children achieve complete remission, though relapses are common.
2. Focal Segmental Glomerulosclerosis (FSGS)
- Epidemiology: <15% of childhood NS; ~25% of adult NS; most common idiopathic NS in African Americans
- Classification:
- Primary (idiopathic): Circulating podocyte permeability factor (as yet unidentified); presents with nephrotic syndrome + >80% foot process effacement on EM
- Secondary:
- Viral: HIV nephropathy (collapsing variant), parvovirus B19, CMV, COVID-19
- Drugs: heroin, interferon, pamidronate, sirolimus, anabolic steroids
- Maladaptive/hyperfiltration: obesity, solitary kidney, sickle cell, reflux nephropathy
- Genetic: NPHS2 (podocin) mutations
- Histology: Focal (some glomeruli affected) and segmental (part of the tuft) areas of sclerosis with hyalinosis on light microscopy; foot process effacement on EM
- Management: Steroids for primary FSGS; calcineurin inhibitors (tacrolimus/cyclosporine) or mycophenolate for steroid-resistant disease; treat underlying cause for secondary FSGS
- Prognosis: Less favorable than MCD; significant risk of progression to ESKD
3. Membranous Nephropathy (MN)
- Epidemiology: Most common cause of primary NS in adults over 40 years; slight male predominance
- Pathogenesis:
- Primary MN: autoantibodies against PLA2R (phospholipase A2 receptor, ~70-80% of primary cases), THSD7A, NELL-1, EXT1/2, Semaphorin 3b
- Secondary MN: associated with autoimmunity (lupus), infection (HBV, HCV), malignancy, drugs (gold, penicillamine, NSAIDs)
- Histology:
- Light microscopy: thickened GBM with "spike and dome" pattern on silver stain
- Immunofluorescence: granular IgG + C3 along GBM (subepithelial)
- EM: subepithelial electron-dense deposits with intervening spikes
- Management: Anti-proteinuric therapy (ACEi/ARB) for all; immunosuppression (cyclophosphamide + steroids, or rituximab) for persistent nephrotic syndrome; rituximab has become a preferred first-line option
- Monitoring: PLA2R antibody titers guide treatment response
- Prognosis: "Rule of thirds" - 1/3 spontaneous remission, 1/3 persistent proteinuria, 1/3 progress to ESKD
Clinical Approach and Investigations
History: Duration and rate of onset; systemic symptoms (rash, joint pain, fever); drug exposures; family history; infections
Examination: Pitting edema (periorbital, dependent), ascites, pleural effusions, anasarca; BP (hypertension more common in FSGS/MN than MCD)
Initial workup:
| Test | Purpose |
|---|---|
| 24-hr urine protein (or spot urine PCR) | Quantify proteinuria |
| Serum albumin, total protein | Confirm hypoalbuminemia |
| Lipid panel | Confirm hyperlipidemia |
| Serum creatinine, eGFR | Assess renal function |
| Urinalysis with microscopy | Lipid bodies, oval fat bodies, fatty casts ("Maltese cross" appearance) |
| CBC | Anemia, infection |
| Complement (C3, C4, CH50) | Low in lupus, MPGN, post-infectious GN |
| ANA, anti-dsDNA, ANCA | Autoimmune causes |
| Hepatitis B, C serology; HIV | Infectious causes |
| Serum and urine protein electrophoresis | Amyloid, multiple myeloma |
| PLA2R antibodies | Primary membranous nephropathy |
| Fasting glucose, HbA1c | Diabetic nephropathy |
Kidney biopsy: Mandatory in adults with new NS (to distinguish cause and guide therapy). In children <12 years with typical MCD presentation, empiric steroid treatment without biopsy is standard.
Management
Non-Disease-Specific (All Causes)
| Intervention | Details |
|---|---|
| Dietary sodium restriction | <2 g/day to limit edema |
| Protein restriction | 0.8-1 g/kg/day (high protein worsens proteinuria) |
| ACE inhibitor or ARB | Reduces proteinuria by lowering intraglomerular pressure; cornerstone of anti-proteinuric therapy |
| Loop diuretics | Furosemide for edema; spironolactone can be added for resistant edema. Note: hypoalbuminemia reduces furosemide protein binding, enlarging its volume of distribution |
| Statins | For hyperlipidemia (LDL usually markedly elevated) |
| Anticoagulation | For high thrombotic risk: albumin <2 g/dL, serum creatinine >3 mg/dL, obesity, or prior thrombosis (especially in MN) |
| Vaccinations | Pneumococcal, influenza (given susceptibility from IgG loss and steroid use) |
Diuretic resistance note: Furosemide combined with ACE inhibitor/ARB reduces proteinuria further but may raise serum creatinine. Albumin infusions do not reliably enhance diuresis and are not routinely recommended.
Disease-Specific (Immunosuppressive)
| Disease | First-line | Second-line / Resistant |
|---|---|---|
| MCD | Prednisone (1 mg/kg/day) | Rituximab, cyclophosphamide, calcineurin inhibitors |
| Primary FSGS | High-dose prednisone | Calcineurin inhibitors (tacrolimus), mycophenolate |
| Primary MN | ACEi/ARB (watchful waiting 6 mo) then cyclophosphamide + steroids or rituximab | Calcineurin inhibitors |
| Lupus class V | Mycophenolate + low-dose steroids | Rituximab |
| Diabetic NS | ACEi/ARB, SGLT2 inhibitors | Disease-specific management |
Complications Summary
- Edema / Anasarca - pleural effusions, ascites, peripheral edema
- Thromboembolism - DVT, PE, renal vein thrombosis (especially MN, albumin <2 g/dL)
- Infections - bacterial peritonitis (SBP in children), cellulitis, pneumococcal sepsis (from IgG/complement loss and steroid immunosuppression)
- AKI - from low effective circulating volume, diuretic overuse, or renal vein thrombosis
- Hyperlipidemia and cardiovascular disease - accelerated atherosclerosis
- Nutritional deficiencies - vitamin D deficiency (loss of VD-binding protein), iron deficiency, zinc deficiency
- Drug interactions - altered binding/distribution of highly albumin-bound drugs (e.g., phenytoin, warfarin)
- CKD progression - risk varies by underlying cause; FSGS and diabetic nephropathy carry the highest risk
Recent Evidence (2025)
A 2025 Cochrane meta-analysis (PMID 40337980) reviewed interventions for idiopathic steroid-resistant nephrotic syndrome in children, providing updated evidence on calcineurin inhibitors and other agents in this challenging population.
Sources: NKF Primer on Kidney Diseases, 8th Edition; Brenner and Rector's The Kidney, 10th Edition; Swanson's Family Medicine Review; Comprehensive Clinical Nephrology, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.