Write answer oflong answer md level for inflammatory bowel diseases
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
I now have extensive, high-quality material from multiple authoritative textbooks. Let me compose the comprehensive MD-level long answer.
Inflammatory Bowel Disease (IBD)
1. Definition and Overview
Inflammatory bowel disease (IBD) is a group of idiopathic, chronic, relapsing and remitting inflammatory conditions of the gastrointestinal tract. The two principal entities are:
- Crohn Disease (CD) - transmural inflammation that can affect any segment of the GI tract from mouth to anus
- Ulcerative Colitis (UC) - mucosal/submucosal inflammation confined to the colon and rectum
A third category, indeterminate colitis, is used when it is not possible to establish a diagnosis of either CD or UC - occurring in up to 10% of IBD patients. These patients have colonic disease in a continuous pattern typical of UC but also features suggestive of CD, such as patchy histologic disease, family history of CD, or perianal lesions.
2. Epidemiology
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Peak age of onset | 15-30 years; 2nd peak in the 7th decade | 20-40 years; 2nd smaller peak beyond the 7th decade |
| Sex distribution (F:M) | 1.2:1 | 1:1 |
| Smoking | More common in active smokers | More common in nonsmokers and former smokers |
| Geographic distribution | Higher in developed, westernized nations; Northern > Southern latitudes | Similar |
IBD has increased in incidence globally, particularly in developing countries adopting Westernized lifestyles. Genetic factors, gut microbiome dysbiosis, environmental exposures, and altered immune responses all contribute.
3. Etiopathogenesis
3.1 Genetic Factors
IBD is polygenic. More than 200 susceptibility loci have been identified. Key genes include:
- NOD2 (CARD15) - most strongly associated with Crohn disease; encodes an intracellular pattern recognition receptor for bacterial muramyl dipeptide. NOD2 variants increase CD risk but are protective in UC.
- PTPN22 - increases CD risk, protective in UC
- ATG16L1 and IRGM - involved in autophagosome formation; autophagy defects impair clearance of intracellular pathogens
- IL10, IL10RA, IL10RB - mutations cause very early onset (infantile) monogenic IBD; IL-10 is a key anti-inflammatory cytokine
- HLA variants - associated with specific extraintestinal manifestations (arthropathy, uveitis, PSC)
Approximately 30% of IBD-associated polymorphisms have indistinguishable effect sizes in CD and UC, reflecting shared immunopathogenesis.
3.2 Immune Dysregulation
Both CD and UC are characterized by:
- Activation of Th17 and Th1 cells (predominant in CD)
- More limited Th2 activation (relatively more prominent in UC)
- Reduced regulatory T cell (Treg) function
- Defective mucosal barrier integrity allowing luminal bacteria to trigger abnormal immune responses
The normal mucosal immune system maintains tolerance to commensal bacteria. In IBD, this homeostasis breaks down, leading to uncontrolled, perpetuated inflammation.
3.3 Environmental/Microbial Factors
- Intestinal dysbiosis: Reduced microbial diversity, decreased short-chain fatty acid (SCFA)-producing bacteria (e.g., Firmicutes), increased Proteobacteria
- Infectious trigger: Infectious enteritis may precede onset in some patients; it is hypothesized that enteritis triggers mucosal immune activation and microbial changes in susceptible individuals
- Antibiotics: Altered microbiome composition
- Appendectomy: Protective against UC
- Oral contraceptives and NSAIDs: May trigger flares
4. Pathology
4.1 Crohn Disease - Pathological Features
Macroscopic (Gross):
- Can involve any region from esophagus to anus
- Skip lesions: Diseased segments interspersed with normal mucosa
- Early lesions: Aphthous ulcers (small, superficial mucosal ulcers)
- Advanced lesions: Deep longitudinal and transverse ulcers creating a cobblestone appearance (normal mucosa = "stones", ulcers = "mortar")
- Transmural inflammation: Thickened bowel wall, narrowed lumen
- Creeping fat: Mesenteric fat wraps around the bowel wall (fat wrapping)
- Strictures and fistulae due to transmural disease
- "String sign" on barium studies due to strictures
Microscopic:
- Transmural inflammation extending through all layers of the bowel wall
- Non-caseating epithelioid granulomas (pathognomonic when present; found in ~50% of resected specimens)
- Lymphoid aggregates in all layers
- Focal crypt architectural irregularity
- Submucosal fibrosis and neural hyperplasia
4.2 Ulcerative Colitis - Pathological Features
Macroscopic (Gross):
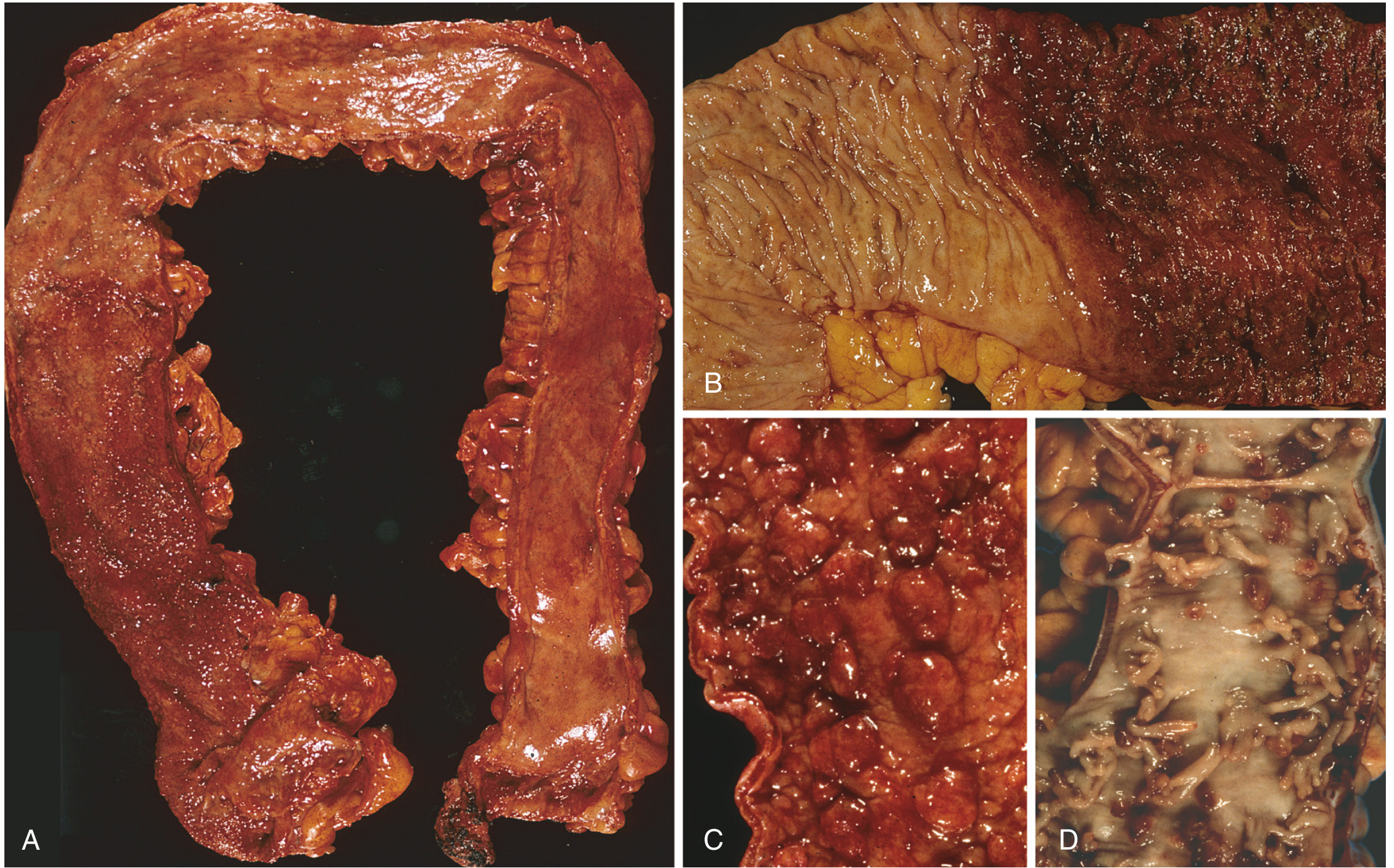
Fig. 1 - Gross pathology of ulcerative colitis. (A) Total colectomy with pancolitis showing active disease, with red, granular mucosa in the cecum (left) and smooth, atrophic mucosa distally (right). (B) Sharp demarcation between active UC (right) and normal mucosa (left). (C) Inflammatory polyps. (D) Mucosal bridges joining inflammatory polyps. - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Continuous involvement starting from the rectum extending proximally (rectum always involved)
- Disease is confluent - no skip lesions
- Granular, red, friable mucosa with contact bleeding
- Pseudopolyps (inflammatory polyps): Islands of regenerating mucosa surrounded by denuded areas
- Disease is limited to mucosa and submucosa (no transmural involvement)
- No fistulae, no strictures (in contrast to CD)
Microscopic:
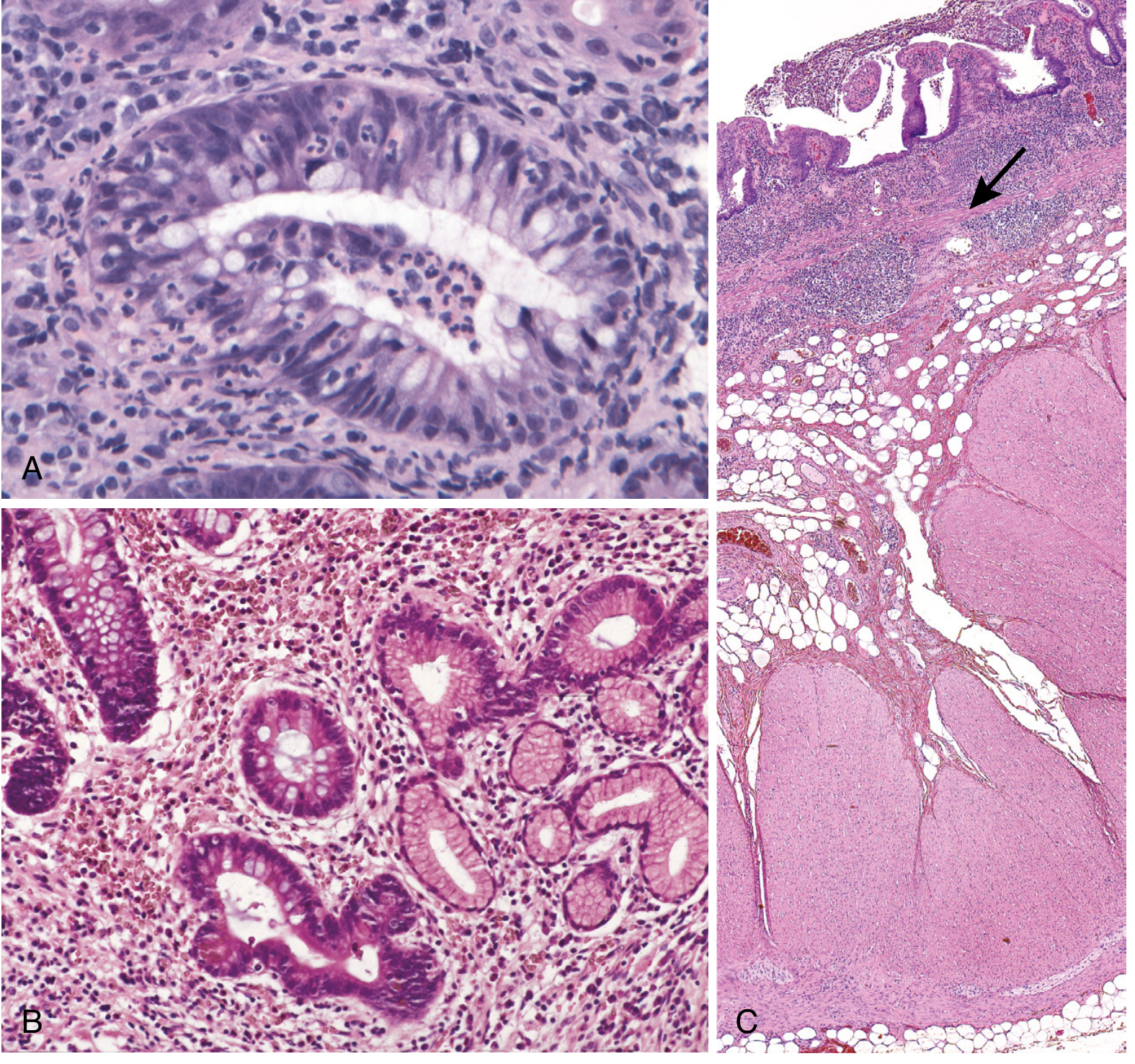
Fig. 2 - Histopathology of ulcerative colitis. (A) Crypt abscess (neutrophils within the crypt lumen). (B) Pseudopyloric metaplasia. (C) Inflammation is confined to the mucosa (above the arrow). - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Crypt abscesses: Neutrophils accumulate within crypt lumina - hallmark of active UC
- Crypt architectural distortion: Branching, shortening, and irregular spacing of crypts
- Diffuse lymphoplasmacytic infiltrate in the lamina propria
- Goblet cell depletion
- Pseudopyloric and Paneth cell metaplasia in chronic disease
- No granulomas (unless a complication is present)
- Inflammation confined to mucosa and superficial submucosa
4.3 Comparison Table: CD vs. UC
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Mouth to anus (most common: terminal ileum + right colon) | Colon and rectum only |
| Rectal involvement | 60% | Always (100%) |
| Pattern | Skip lesions | Continuous (from rectum proximally) |
| Depth of inflammation | Transmural | Mucosal/submucosal only |
| Ulceration | Discrete, serpiginous, cobblestone | Continuous, superficial |
| Granulomas | Yes (non-caseating, ~50%) | No |
| Fistulae | Yes (20-40%) | No |
| Strictures | Yes | Rare |
| Perianal disease | Yes (30%) | No |
| Goblet cell depletion | Less prominent | Prominent |
| Crypt abscesses | Less common | Common |
5. Clinical Features
5.1 Crohn Disease
Symptoms depend on location and severity:
- Terminal ileum disease (70%) - most common; right lower quadrant pain, diarrhea (usually non-bloody), weight loss, fatigue
- Ileocolonic disease (40%)
- Primary ileal disease (30%)
- Perianal disease (30%): Fissures, fistulae, skin tags, abscesses
- Colonic disease (25%): Diarrhea, hematochezia (less frequent than UC)
- Upper GI disease (~5%): Dysphagia, odynophagia, heartburn, epigastric pain
Fistulae develop in 20-40% of patients and include:
- Enteroenteric
- Rectovaginal
- Enterovesicular (pneumaturia, fecaluria)
- Enterocutaneous
- Perianal
Systemic features: Fever, weight loss, anemia, malnutrition (especially with small bowel involvement)
Obstructive symptoms: Crampy abdominal pain, distension, nausea - due to strictures
5.2 Ulcerative Colitis
Symptoms depend on extent and severity:
- Proctitis (limited to rectum): Tenesmus, rectal urgency, bloody discharge; systemic symptoms uncommon
- Left-sided colitis (to splenic flexure): Bloody diarrhea, lower abdominal cramps
- Pancolitis: Profuse bloody diarrhea, severe abdominal pain, fever, weight loss
At diagnosis:
- 14-37% have pancolitis
- 36-41% have disease up to the splenic flexure
- Remaining have proctitis or proctosigmoiditis
Severity Classification (Truelove & Witts):
| Severity | Stools/day | Blood | Pulse | Temperature | ESR | Hb |
|---|---|---|---|---|---|---|
| Mild | <4 | Small | Normal | Normal | <30 | >11 g/dL |
| Moderate | 4-6 | Moderate | ≤90 | ≤37.8°C | ≤30 | ≥10.5 g/dL |
| Severe | >6 | Large | >90 | >37.8°C | >30 | <10.5 g/dL |
More than half of patients have clinically mild disease, though almost all experience at least one relapse over a 10-year period.
6. Extraintestinal Manifestations
About one third of IBD patients develop extraintestinal manifestations (EIMs). These can be classified as disease-activity-related or independent.
| Manifestation | Description | Prevalence | Correlation with Bowel Activity | Treatment |
|---|---|---|---|---|
| Erythema nodosum | Painful, tender, raised red nodules on anterior lower legs | 1-9% UC; 6-15% CD; 5:1 F:M | 90% associated with active disease | Resolves with treatment of bowel disease |
| Pyoderma gangrenosum | Painful ulcers on lower limbs, trunk, near stomas | 0.5-2% IBD | Not associated with active bowel disease | Immunosuppressive therapy |
| Aphthous oral ulcers | Ulcerations in buccal mucosa | 20-30% CD; 20% UC | Associated with active disease | Resolves with treatment |
| Uveitis | Eye pain, redness, loss of visual acuity, floaters | Less common; 3:1 F:M | Anterior uveitis: 30% with erythema nodosum; Posterior uveitis: 90% with ankylosing spondylitis | Topical/systemic corticosteroids |
| Episcleritis | Eye redness, irritation, watering | 5-8% IBD; 3:1 F:M | Associated with active disease | Resolves with treatment or topical steroids |
| Primary sclerosing cholangitis (PSC) | Recurrent biliary sepsis, pruritus, portal hypertension | 3-5% UC; male preponderance | NOT associated with bowel activity; associated with colorectal cancer | Supportive; management of complications |
| Peripheral arthritis | Large or small joint arthritis | Common | Often parallels bowel activity | Treat underlying disease; NSAIDs (use with caution) |
| Ankylosing spondylitis | Axial arthropathy, sacroiliitis | Less common; HLA-B27 associated | Independent of bowel activity | NSAIDs, anti-TNF agents |
| Venous thromboembolism | DVT, PE | Increased risk; may be underdiagnosed | Related to disease activity (hypercoagulable state) | Anticoagulation |
7. Investigations
7.1 Laboratory Tests
- CBC: Anemia (from blood loss, chronic disease, or B12/folate deficiency), leukocytosis in active disease/abscess
- CRP and ESR: Elevated in active disease; useful for monitoring
- Fecal calprotectin: Elevated in active disease, lower in remission - useful marker of mucosal inflammation
- Albumin: Low in severe/prolonged disease - indicates malnutrition
- Serum B12: Low with >100 cm distal ileum disease or resection (CD)
- Iron studies: Iron deficiency from blood loss
7.2 Serologic Markers
Useful to support diagnosis but not independent diagnostic criteria:
| Marker | CD | UC |
|---|---|---|
| ASCA (anti-Saccharomyces cerevisiae antibodies) | 40-70% | <15% |
| pANCA (perinuclear antineutrophil cytoplasmic antibody) | 20% (colon-predominant) | 55% |
| Anti-OmpC (E. coli outer membrane porin C) | Positive | Negative |
| Anti-CBir1 (flagellin) | Positive | Negative |
ASCA-positive + pANCA-negative: Sensitivity 55%, Specificity 93% for Crohn disease
7.3 Endoscopy
Colonoscopy with biopsy is essential - diagnosis of IBD is contingent upon accurate histopathologic results.
| Finding | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Pattern | Skip lesions; ileocecal region most common | Continuous from rectum proximally |
| Mucosa | Cobblestoning, serpiginous/linear ulcers, aphthous ulcers | Granular, friable, continuous erosions |
| Terminal ileum | Often involved | Backwash ileitis only (in pancolitis) |
| Strictures | Common | Rare (suggests malignancy) |
| Histology | Non-caseating granulomas; focal crypt changes | Crypt abscesses; diffuse lamina propria infiltrate |
Endoscopic view of Crohn disease cobblestoning:
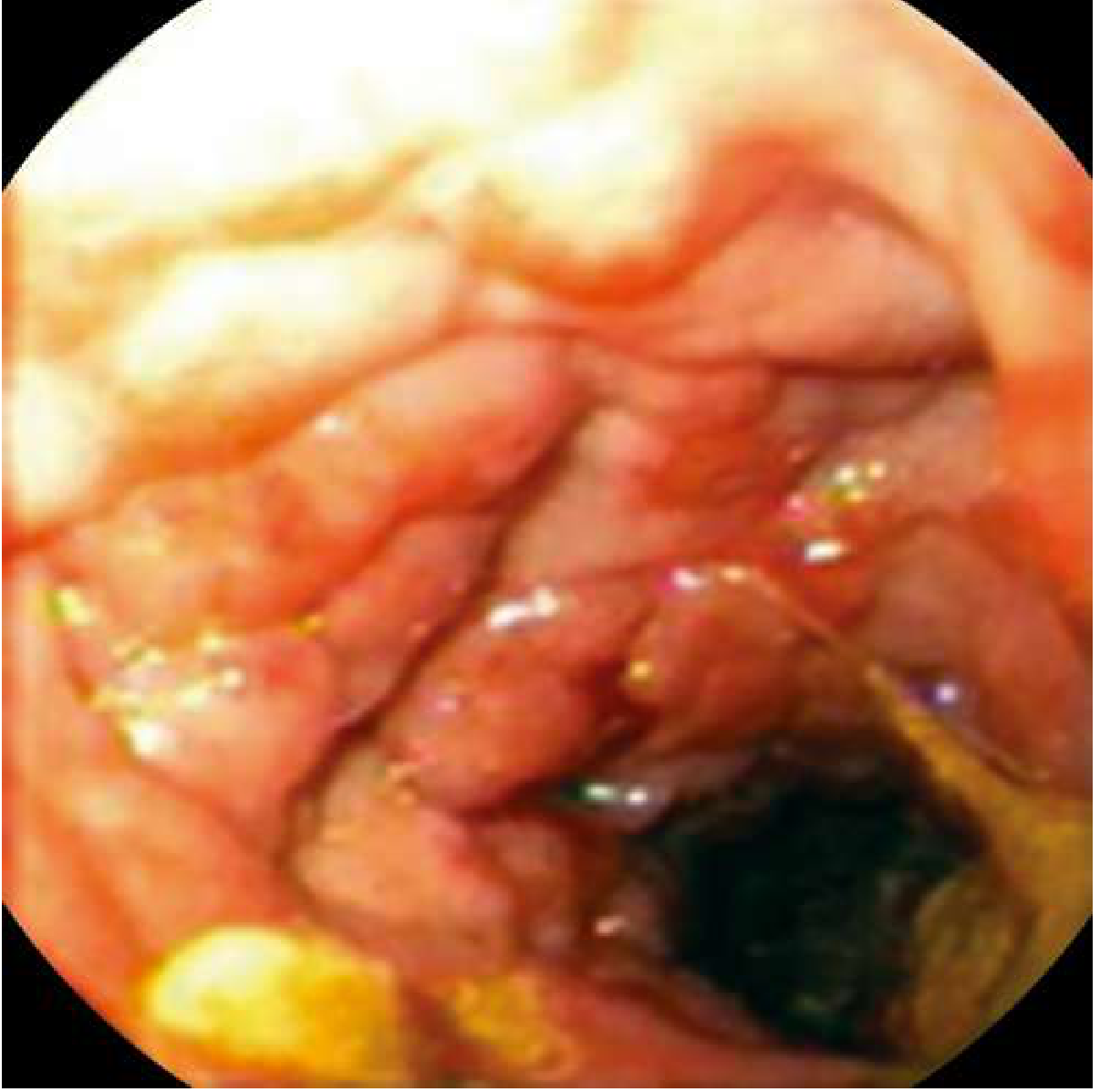
Fig. 3 - Endoscopic appearance of Crohn disease with cobblestoning. The intersecting ulcers leave islands of normal mucosa resembling cobblestones. - Goldman-Cecil Medicine
7.4 Imaging
- CT/MR Enterography: Best for evaluating small bowel extent, fistulae, abscesses, and complications in CD
- Barium follow-through: "String sign" (severe luminal narrowing) in CD strictures
- Abdominal X-ray: Used in acute settings; detects toxic megacolon (transverse colon diameter >6 cm with systemic toxicity)
- MRCP/ERCP: For PSC evaluation
- Capsule endoscopy: For small bowel CD (contraindicated with known strictures)
- Pelvic MRI: Gold standard for perianal fistula mapping in CD
8. Complications
8.1 Crohn Disease Complications
- Fistulae: Enterocutaneous, enterovesicular, rectovaginal, enteroenteric
- Intra-abdominal abscesses: From penetrating disease or blind-ending fistulae
- Strictures leading to bowel obstruction
- Perianal disease: Fissures, abscesses, skin tags
- Malabsorption and nutritional deficiencies (B12, fat-soluble vitamins, zinc, iron)
- Gallstones: Impaired bile acid reabsorption from terminal ileum disease
- Oxalate renal stones: Increased colonic oxalate absorption
- Short bowel syndrome: Following extensive resections
- Colorectal carcinoma: Risk 4-20x general population; often mucinous type, commonly in bypassed/strictured colon segments
8.2 Ulcerative Colitis Complications
- Toxic megacolon: Occurs in up to 10% of UC patients. Defined as total or segmental colonic dilatation (>6 cm on AXR) with systemic toxicity (fever >38.6°C, HR >120, leukocytosis, anemia). Medical emergency - antidiarrheal and anticholinergic medications are contraindicated. Requires IV corticosteroids; surgery if not responsive
- Massive hemorrhage: From sustained blood loss
- Bowel perforation: Often at the site of deepest ulceration
- Colorectal carcinoma (CRC): Major long-term complication
- Risk begins after 7 years of disease duration
- Rises approximately 10% per decade
- Reaches as high as 34% at 30 years (in some series; population-based data suggests 15-18% at 30 years)
- Greatest risk with pancolitis (universal colitis)
- Left-sided disease: Risk begins ~10 years later than pancolitis
- Proctitis alone: Minimal increased risk
- Dysplasia is the precursor lesion - graded as low-grade or high-grade
- Colonoscopic surveillance programs recommended starting 8-10 years after diagnosis
9. Treatment
The aim of medical therapy is to induce clinical remission and maintain remission while simultaneously healing the mucosa (mucosal healing is the modern therapeutic target).
9.1 Categories of Medical Therapy
A. 5-Aminosalicylates (5-ASA)
Mechanism: Topical anti-inflammatory within the intestinal lumen; inhibits NF-κB and arachidonic acid metabolism
Agents:
- Sulfasalazine: Combination of sulfapyridine (carrier) + 5-ASA (active component). Active moiety released in the colon by bacterial action. Dose: 3-6 g/day. Side effects: Headache, nausea, oligospermia, hemolytic anemia, agranulocytosis.
- Mesalamine (5-ASA): pH-dependent release in the small intestine/colon. Fewer systemic side effects.
- Olsalazine, Balsalazide: Azo-bonded prodrugs, colon-specific delivery
Role:
- First-line for mild-to-moderate UC (induction and maintenance)
- Effective for ileocolonic and colonic CD (sulfasalazine: 45-55% response rate for mild-moderate disease)
- Not effective for small bowel CD alone
B. Corticosteroids
Mechanism: Broad anti-inflammatory and immunosuppressive effects
Agents:
- Oral prednisone: 40-60 mg/day for moderate-severe active IBD
- Enteric-coated budesonide (9 mg/day): For distal ileal/right colonic CD; ~70% response rate at 8 weeks; lower systemic side effects due to high first-pass metabolism. Significantly more effective than mesalamine for distal ileal/right colonic CD.
- IV hydrocortisone: For severe/fulminant disease requiring hospitalization
Key points:
- Not for maintenance therapy - cause significant side effects with prolonged use (osteoporosis, hyperglycemia, adrenal suppression, Cushingoid features)
- Used for induction only
C. Immunomodulators (Thiopurines and Methotrexate)
-
Azathioprine (2-2.5 mg/kg/day) and 6-mercaptopurine (6-MP, 1-1.5 mg/kg/day):
- Purine antimetabolites - inhibit lymphocyte proliferation
- Used for maintenance of remission and steroid-sparing
- Slow onset of action (3-6 months to full effect)
- Side effects: Pancreatitis, hepatotoxicity, myelosuppression, increased risk of lymphoma (especially in males <35 years with thiopurines)
- Check TPMT enzyme activity before starting (enzyme deficiency increases toxicity risk)
-
Methotrexate (15-25 mg/week IM):
- Alternative immunomodulator, especially in patients intolerant of thiopurines
- Preferred in males <35 years in place of azathioprine (lower lymphoma risk)
- Side effects: Hepatotoxicity, pulmonary toxicity, teratogenicity - requires folate supplementation and contraception
-
Ozanimod: Sphingosine-1-phosphate (S1P) receptor modulator - prevents lymphocyte egress from lymph nodes; newer oral small molecule for UC
D. Biologics
Anti-TNF-α agents:
| Agent | Administration | Indication |
|---|---|---|
| Infliximab (chimeric) | IV: 5 mg/kg at 0, 2, 6 weeks, then every 8 weeks | CD and UC |
| Adalimumab (fully human) | SC: 160 mg, 80 mg, then 40 mg every 2 weeks | CD and UC |
| Certolizumab pegol | SC: 400 mg at 0, 2, 4 weeks, then every 4 weeks | CD (US approval) |
| Golimumab | SC | UC |
- Combined infliximab + azathioprine is superior to monotherapy for both induction and maintenance
- Up to 50% of patients eventually lose response to anti-TNF therapy
- Meta-analysis: Adalimumab, infliximab + azathioprine, or ustekinumab are the three most effective therapies for induction and maintenance in CD
Anti-integrin agents (gut-selective):
-
Vedolizumab: Humanized monoclonal antibody targeting the α4β7 integrin. Blocks binding of lymphocytes to MAdCAM-1 (mucosal addressin cell adhesion molecule-1) on gut venular endothelium - preventing lymphocyte recruitment to intestinal mucosa. Gut-selective mechanism means lower systemic immunosuppression.
- Dose: 300 mg IV at 0, 2, 6 weeks, then every 8 weeks
- Approved for moderate-severe CD and UC
- Side effects: Headache, arthralgia, nasopharyngitis, hypersensitivity reactions
-
Natalizumab: Chimeric anti-α4 integrin antibody. Blocks both gut and CNS lymphocyte trafficking. Restricted use due to risk of Progressive Multifocal Leukoencephalopathy (PML) from JC virus reactivation. Only for CD patients negative for JC virus antibody.
Anti-IL-12/23 agents:
- Ustekinumab: Fully humanized monoclonal antibody targeting the p40 subunit shared by IL-12 and IL-23. Prevents activation of IL-12Rβ1 and IL-23 receptors on CD4+ T cells and NK cells, suppressing Th1 and Th17 responses.
- Induction: IV 260-520 mg (weight-based), then SC 90 mg every 8 weeks for maintenance
- T½ up to 120 days - discontinue 15 weeks before live vaccines
- Approved for moderate-severe CD and UC
- Side effects: Upper respiratory infections, headache, arthralgia
Anti-IL-23 agents:
- Risankizumab (targets IL-23 p19 subunit only): Approved for moderate-severe CD; used for upper GI and systemic CD
JAK inhibitors (small molecules):
- Tofacitinib (JAK1/3 inhibitor): Oral agent for moderate-severe UC; blocks cytokine signaling
- Side effects: Increased risk of infections, VTE, cardiovascular events - use with caution in patients >50 years with cardiovascular risk factors
E. Antibiotics
- Metronidazole and ciprofloxacin: Used for perianal fistulae, intra-abdominal abscesses, and bacterial overgrowth in CD
- Not recommended as primary therapy for UC
9.2 Treatment Strategy by Severity and Disease
UC Treatment Algorithm
Mild-Moderate UC:
- First-line: Oral + rectal 5-ASA (combined is more effective than oral alone)
- Add oral corticosteroids if no response after 2-4 weeks
Moderate-Severe UC:
- Oral corticosteroids (prednisone 40-60 mg/day) ± 5-ASA
- If steroid-dependent/refractory: Add immunomodulator (azathioprine/6-MP) or escalate to biologics
- Biologics (infliximab, adalimumab, vedolizumab, ustekinumab) for moderate-severe disease refractory to conventional therapy
Severe/Fulminant UC (hospitalization required):
- IV corticosteroids (hydrocortisone 300-400 mg/day or methylprednisolone 60 mg/day)
- Cyclosporine IV (2-4 mg/kg/day) or infliximab (5 mg/kg) as rescue therapy for steroid-refractory disease
- Evaluate for toxic megacolon - strict avoidance of antidiarrheal/anticholinergic agents
- Surgery if no response to 3-5 days of IV steroids or complications arise
CD Treatment Algorithm
Mild-Moderate Ileocolonic/Colonic CD:
- Budesonide (9 mg/day) for distal ileal/right colonic disease
- Sulfasalazine for colonic/ileocolonic disease (limited efficacy)
Moderate-Severe CD:
- Systemic corticosteroids (prednisone 40-60 mg/day) for induction
- Add immunomodulator (azathioprine or methotrexate) for maintenance
- Biologics: Infliximab, adalimumab (± azathioprine), ustekinumab for high-risk/severe disease
- Early combined immunosuppression (anti-TNF + antimetabolite) is more effective than conventional stepwise therapy
Severe/Hospitalized CD:
- NPO, IV fluid resuscitation
- IV corticosteroids
- Surgical consultation for abscesses, obstruction, perforation
Fistulizing CD:
- Metronidazole + ciprofloxacin (symptomatic relief)
- Infliximab or adalimumab (60-80% closure rates for perianal fistulae)
- Drainage of abscesses before biologic therapy
9.3 Surgical Treatment
Ulcerative Colitis
Surgery (colectomy) is curative for intestinal disease in UC (unlike CD). Indications:
- Fulminant colitis/toxic megacolon not responding to medical therapy
- Massive hemorrhage
- Perforation
- Colonic dysplasia or carcinoma
- Chronic refractory disease
Procedure of choice: Total proctocolectomy with ileal pouch-anal anastomosis (IPAA/J-pouch) - restores intestinal continuity, avoids permanent stoma. Note: Extraintestinal manifestations may persist after colectomy.
Crohn Disease
Surgery is not curative - recurrence is common after resection. Indications:
- Bowel obstruction from strictures
- Intra-abdominal abscesses
- Fistulae not responding to medical therapy
- Malignancy
- Growth retardation (pediatric)
Principle: Bowel-conserving surgery - resect as little bowel as possible to prevent short bowel syndrome. Strictureplasty preferred over resection for multiple short strictures.
10. Surveillance for Colorectal Carcinoma
- Colonoscopic surveillance should begin 8-10 years after diagnosis of UC and IBD-associated colitis
- Annual or biennial colonoscopy with multiple random biopsies
- Dysplasia (low-grade or high-grade) is the target lesion; high-grade dysplasia = indication for colectomy
- Chromosomal alterations (p53 overexpression, 18q LOH), high MSI, and specific miRNA methylation may precede histologic dysplasia
- CRC in UC is associated with a similar survival to sporadic CRC when matched controls are used
- PSC co-existing with UC significantly increases CRC risk
11. Key Differentiating Points: CD vs. UC (Summary)
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Mouth to anus | Colon only |
| Rectal sparing | Often (except 60% with colonic CD) | Never (rectum always involved) |
| Skip lesions | Yes | No (continuous) |
| Transmural inflammation | Yes | No (mucosal/submucosal) |
| Granulomas | Yes (~50%) | No |
| Fistulae/sinuses | Yes | No |
| Strictures | Yes | Rare |
| Perianal disease | Yes (30%) | No |
| Cobblestone appearance | Yes | No |
| Crypt abscesses | Less prominent | Hallmark |
| Cancer risk | Increased (4-20x; especially ileocolitis) | Increased (cumulative 15-34% at 30 yrs) |
| Surgery curative | No | Yes (colectomy) |
| Smoking relationship | More common in smokers | Protective (disease worsens with cessation) |
| ASCA | Positive (40-70%) | <15% |
| pANCA | 20% | 55% |
| NOD2 mutations | Yes | Protective |
12. Special Situations
Pregnancy
- IBD does not significantly impair fertility when in remission
- Active disease increases risk of preterm birth, low birth weight, miscarriage
- 5-ASA agents are generally safe
- Methotrexate: Absolutely contraindicated (teratogen) - must discontinue ≥3 months before conception
- Azathioprine/6-MP: Generally continued if benefits outweigh risks
- Anti-TNF agents: Held after 24-32 weeks to reduce neonatal immunosuppression (certolizumab pegol has minimal placental transfer)
- Corticosteroids: Used when essential
Pediatric IBD (Very Early Onset IBD)
- Can be monogenic - mutations in IL10, IL10RA, IL10RB
- More than 100 genes encode monogenic IBD
- Standard treatments often less effective; genetic testing warranted
13. Prognosis
- UC: Relapsing-remitting course; >50% have mild disease; colectomy rate has fallen sharply with modern biologics; surgery is curative for intestinal disease
- CD: Chronic progressive disease with risk of bowel damage and surgical resection accumulating over time; surgery is not curative; average of 2-3 bowel resections over a lifetime in severe cases
- Both: Significantly reduced quality of life during active disease; extraintestinal manifestations and psychological comorbidities (anxiety, depression) are common
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Goldman-Cecil Medicine | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Goodman & Gilman's The Pharmacological Basis of Therapeutics | Rheumatology (2022, Elsevier)
This is a shared conversation. Sign in to Orris to start your own chat.