what is cardiac achalasia
Reading File
Finding Sources
Searching PubMed
achalasia cardia esophageal
Reading File
Reading File
Reading File
I now have comprehensive information from the textbook. Let me compile a thorough answer.
Achalasia Cardia (Cardiac Achalasia / Esophageal Achalasia)
"Cardiac achalasia" is a colloquial term for achalasia cardia (or esophageal achalasia). "Cardia" refers to the cardia of the stomach - the region at the gastroesophageal junction (GEJ) - not the heart. The word "achalasia" is Greek for "failure to relax."
Definition
Achalasia is a primary esophageal motility disorder characterized by two key physiologic abnormalities:
- Impaired lower esophageal sphincter (LES) relaxation with swallowing
- Aperistalsis (absent peristalsis) in the smooth muscle segment of the esophagus
If premature, spastic contractions are present in the esophageal body, it is called type III (spastic) achalasia.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Pathophysiology
The underlying mechanism involves progressive loss of ganglion cells in the myenteric (Auerbach's) plexus of the smooth muscle esophagus, including the LES:
- The degree of ganglion cell loss parallels disease duration
- Inflammatory cells (predominantly cytotoxic T cells) surround and destroy ganglion cells
- Inhibitory neurons (which use nitric oxide [NO] and vasoactive intestinal peptide [VIP]) are lost early - these normally mediate LES relaxation and peristalsis
- Excitatory (cholinergic) neurons may also be impaired
- Loss of NO synthase and VIP-staining neurons at the GEJ is well documented
Underlying cause: Likely an autoimmune process in genetically susceptible individuals, possibly triggered by latent HSV-1 infection. Antibodies against myenteric neurons are detectable in serum, and specific HLA alleles are associated.
Types (Chicago Classification / HRM Subtypes)
High-resolution manometry (HRM) distinguishes three subtypes:
| Type | Description | Treatment Response |
|---|---|---|
| Type I - Classic | Aperistalsis + failed LES relaxation; dilated esophagus | Moderate |
| Type II - Achalasia with compression | Pan-esophageal pressurization; early disease | Best (pneumatic dilation ~100% effective) |
| Type III - Spastic | Premature/spastic distal contractions | Poorer (Heller myotomy preferred) |
Clinical Features
| Symptom | Details |
|---|---|
| Dysphagia | ALL patients have solid food dysphagia; most also have liquid dysphagia. Onset is gradual, often present for years before diagnosis |
| Regurgitation | Nonacid, nonbilious; food eaten hours or days earlier; worsens with recumbency in advanced disease |
| Chest pain | ~2/3 of patients early in disease; similar in character to angina; may resolve spontaneously over time |
| Weight loss | From reduced food intake |
| Halitosis | From retained, fermenting food in esophagus |
| Aspiration pneumonia | Up to 10% of advanced cases develop bronchopulmonary complications |
| Hiccups | Less common |
| "Heartburn" | Paradoxically reported, but actually from bacterial fermentation of retained food - NOT true acid reflux |
Diagnosis
- Barium swallow: Classic "bird's beak" appearance at the GEJ; dilated esophagus
- High-resolution manometry (HRM): Gold standard - shows failed LES relaxation and aperistalsis; used for subtyping
- Upper endoscopy: Rules out pseudoachalasia (malignancy at GEJ); may show retained food/saliva
- Timed barium swallow: Useful for monitoring treatment response
Treatment
Since the underlying neuropathology cannot be corrected, treatment aims to reduce LES pressure and improve esophageal emptying:
1. Pharmacologic (temporizing only - not very effective)
- Calcium channel blockers (e.g., nifedipine)
- Nitrates (e.g., isosorbide dinitrate)
- Botulinum toxin (Botox) injection into the LES - useful in elderly/high surgical risk patients; effect lasts ~6-12 months
2. Pneumatic Dilation
- Endoscopic balloon dilation to forcefully disrupt LES fibers
- ~90% effective, especially for Type II achalasia (100% efficacy in European RCT)
- Risk of esophageal perforation ~1%
- Preferred first-line for Type I and II due to low cost vs. surgery
3. Surgical - Laparoscopic Heller Myotomy (LHM)
- Surgical cutting of the LES muscle fibers
- ~90% effective, preferred for Type III achalasia (86% vs. 40% with dilation)
- Usually combined with partial fundoplication to prevent post-op reflux
4. POEM (Per-Oral Endoscopic Myotomy)
- Endoscopic technique; increasingly preferred, especially for Type III
- Recent reviews (Provenza & Romanelli, 2025) highlight POEM as an important advance in achalasia management
Key Distinction: Pseudoachalasia
Secondary achalasia ("pseudoachalasia") can mimic idiopathic achalasia and is caused by:
- Malignancy at the GEJ (adenocarcinoma, gastric cancer) invading the myenteric plexus
- Chagas disease (Trypanosoma cruzi destroying ganglion cells)
- Other infiltrative processes
Always rule out with endoscopy, especially in older patients or those with rapid symptom onset and significant weight loss.
Summary: Achalasia cardia is a progressive neurodegenerative esophageal motility disorder caused by autoimmune destruction of myenteric plexus neurons at the GEJ, resulting in failure of LES relaxation and absent peristalsis. The cardinal symptom is dysphagia to both solids and liquids, and treatment is directed at mechanically reducing LES pressure.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Recent review: Provenza & Romanelli, Surg Clin North Am, 2025 (PMID 39523069)
and what is pyloric stenosis
Finding Sources
Searching PubMed
pyloric stenosis hypertrophic infantile
Reading File
Reading File
Reading File
Loading Image
Excellent - I have comprehensive textbook content and imaging. Here is the full answer.
Pyloric Stenosis
Pyloric stenosis is a narrowing of the pyloric canal - the outlet of the stomach that connects to the duodenum. It occurs in two main forms: congenital (infantile) and acquired (adult).
1. Infantile Hypertrophic Pyloric Stenosis (IHPS)
This is by far the most common and clinically important form.
Definition
A condition where the circular (and to a lesser degree longitudinal) muscle of the pylorus hypertrophies and hyperplasias, causing progressive obstruction of the gastric outlet. Importantly, it is not a congenital defect present at birth - the muscle thickening develops postnatally.
Epidemiology
- Incidence: ~1 in 300-900 live births (~0.2% general population)
- Male:female ratio: 4-5:1 (much more common in males)
- Higher risk in: firstborn child, premature infants, young maternal age, siblings of affected patients (~6%), monozygotic twins (high concordance)
- Associated conditions: Turner syndrome, trisomy 18
- Risk factor: Erythromycin or azithromycin exposure (oral or via breast milk) in the first 2 weeks of life
Pathology
Hyperplasia of the pyloric muscularis propria causes outflow tract obstruction, worsened by mucosal and submucosal edema and inflammation. The hypertrophied pylorus forms a firm, palpable mass.
Clinical Features
| Feature | Details |
|---|---|
| Age at presentation | 3-6 weeks of life (range 2-10 weeks); rare after 12 weeks |
| Vomiting | Progressively worsening, forceful projectile, non-bilious vomiting after feeds (non-bilious because obstruction is proximal to the ampulla of Vater) |
| Hunger after vomiting | Infant demands feeding again immediately - "hungry vomiter" |
| Visible peristalsis | Left-to-right peristaltic waves across upper abdomen just before vomiting |
| Palpable "olive" | Firm, ovoid, 1-2 cm epigastric mass present in up to 90% of cases - nearly pathognomonic |
| Dehydration | Sunken fontanelles, dry mucous membranes, decreased wet diapers |
| Weight loss/failure to thrive | From persistent vomiting and inability to absorb feeds |
Metabolic Consequences
Loss of gastric acid (HCl) and fluid through vomiting leads to a classic triad:
Hypochloremic, Hypokalemic, Metabolic Alkalosis
- Vomiting loses H⁺ and Cl⁻ → metabolic alkalosis + hypochloremia
- Kidneys initially excrete K⁺ and Na⁺ to retain H⁺ (paradoxical aciduria) → hypokalemia
Diagnosis
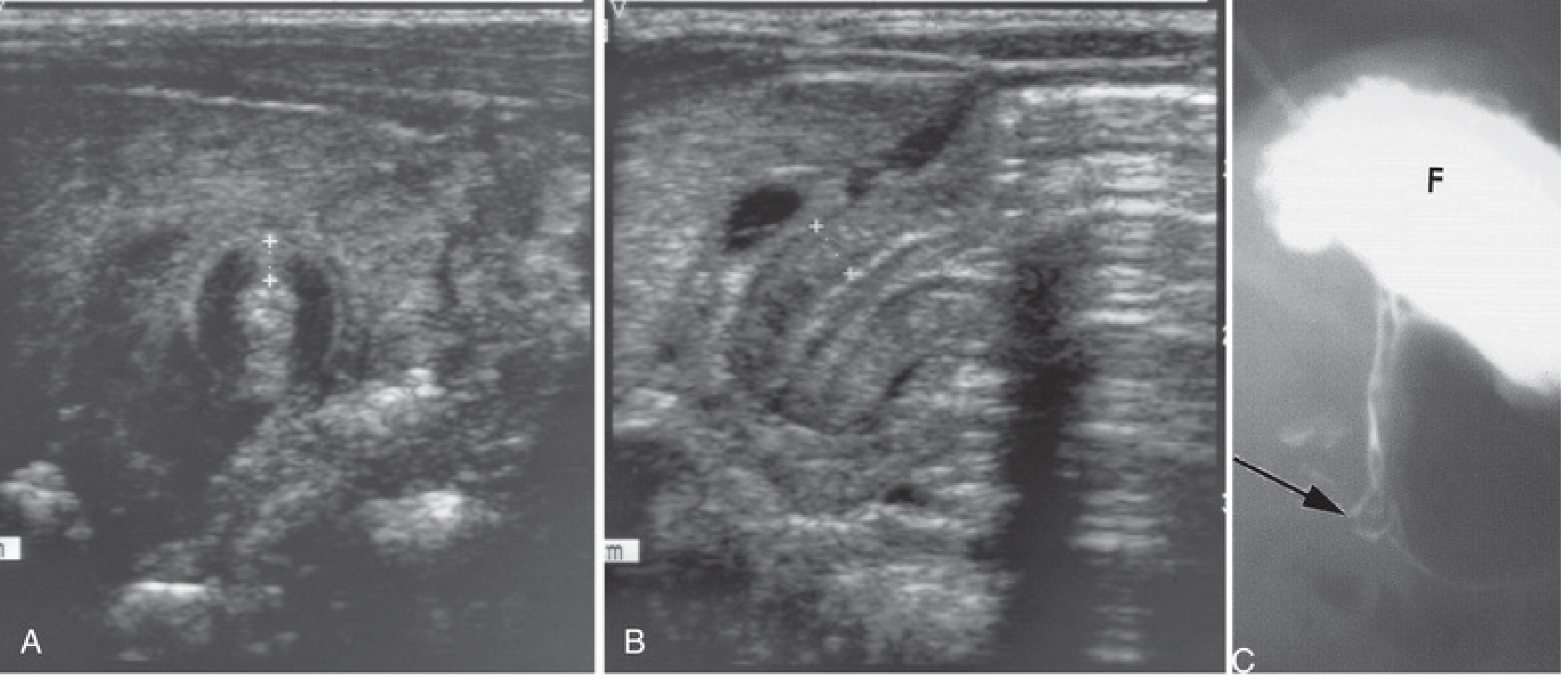
Ultrasound is the gold standard. Diagnostic criteria:
- Pyloric muscle wall thickness ≥ 4 mm
- Pyloric channel length ≥ 16 mm
- No fluid passage through pylorus observed during exam
Upper GI (barium study) used when ultrasound is equivocal - shows elongated, narrow pyloric channel ("string sign" or "railroad track sign").
Treatment
Surgery is NOT an emergency - resuscitation must come first.
Step 1 - Preoperative resuscitation:
- IV fluids: 1-2 boluses of 20 mL/kg normal saline + 1.5× maintenance D5/NS
- Correct electrolytes every 6-12 hours
- Target: chloride 90-100 mEq/L, bicarbonate ≤30 mEq/L
- Do not give anesthesia until metabolic alkalosis is corrected (bicarbonate >30 mEq/L impairs respiratory drive → risk of post-op apnea/arrest)
Step 2 - Pyloromyotomy (Ramstedt procedure):
- A longitudinal incision through the anterior wall of the pyloric muscle, splitting it down to (but not through) the mucosa
- Laparoscopic pyloromyotomy is now the operation of choice (3 small incisions)
- Open approaches (right upper quadrant or periumbilical) are also used
- A "leak test" with 30-60 mL air via OGT confirms mucosal integrity
- Most infants discharged within 36 hours after tolerating feeds
Complications of pyloromyotomy:
- Incomplete myotomy - ongoing projectile vomiting; requires return to OR
- Mucosal perforation - repair and rotate pylorus for repeat myotomy
Recent evidence (Al-Ansari et al., 2025, PMID 41283384) confirms laparoscopic pyloromyotomy has equivalent outcomes to open surgery with shorter hospital stay.
2. Acquired (Adult) Pyloric Stenosis
Adult pyloric stenosis is almost always secondary to another pathology:
| Cause | Mechanism |
|---|---|
| Peptic ulcer disease | Antral gastritis or ulcers near the pylorus → fibrosis and scarring |
| Gastric carcinoma | Malignant infiltration and fibrosis of the distal stomach |
| Pancreatic carcinoma | External compression + infiltration of the pyloric channel |
Symptoms in adults include postprandial vomiting (non-projectile, often bilious or containing old food), weight loss, and early satiety. Management is directed at the underlying cause.
Summary Comparison
| Feature | Infantile (IHPS) | Adult (Acquired) |
|---|---|---|
| Cause | Idiopathic muscle hypertrophy | PUD, carcinoma, inflammation |
| Age | 3-6 weeks | Any adult age |
| Vomiting | Projectile, non-bilious | Less projectile, may be bilious |
| Metabolic effect | Hypochloremic hypokalemic alkalosis | Variable |
| Diagnosis | Ultrasound | Endoscopy, CT, barium |
| Treatment | Pyloromyotomy | Treat underlying cause |
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Current Surgical Therapy, 14e
- The Developing Human: Clinically Oriented Embryology
whats pleomorphism?
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
This is a shared conversation. Sign in to Orris to start your own chat.