Explain gastric emptying
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Gastric Emptying
Gastric emptying is the process by which the stomach delivers its contents into the duodenum in a controlled, regulated manner. It is a tightly coordinated motor event involving the fundus, antrum, pylorus, and duodenum working together.
1. Overview and Timing
After a meal, the stomach holds approximately 1.5 L of mixed content (solids, liquids, and gastric secretions). Complete emptying takes roughly 3 hours, though this varies with meal composition. The rate must be carefully regulated to:
-
Allow adequate time for neutralisation of gastric H+ by pancreatic HCO3- in the duodenum
-
Allow sufficient time for digestion and absorption of nutrients in the small intestine
-
Costanzo Physiology 7th Edition, p. 357
2. Mechanics: Propulsion, Grinding, and Retropulsion
The antrum, pylorus, and duodenum work as a functional unit:
Propulsion - Peristaltic waves sweep from the gastric body toward the antrum, pushing a bolus toward the pylorus.
Grinding - The bolus is trapped near the antrum while the pylorus contracts and closes. The antrum churns the trapped material to break down solid particles.
Retropulsion - Most gastric contents (particles >2 mm) are pushed back into the stomach body for further pulverisation and shearing. Only material containing particles <2 mm is propelled through the pylorus into the duodenum. These three steps cycle repeatedly until the stomach is emptied.
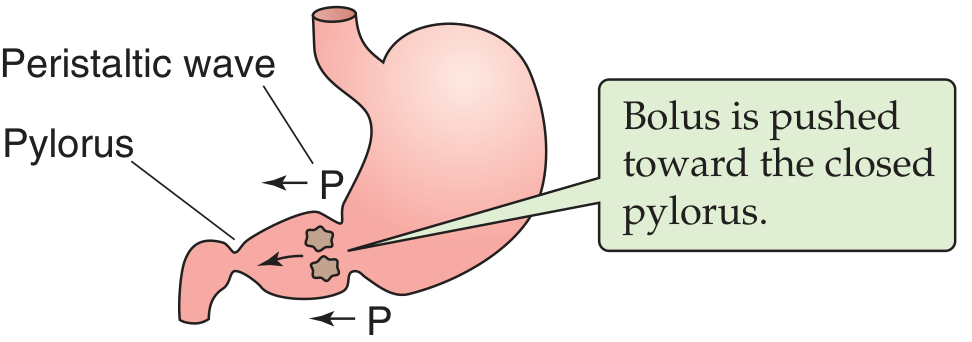
- Medical Physiology (Boron & Boulpaep), Fig. 42-15
3. Liquids vs. Solids
| Feature | Liquids | Solids |
|---|---|---|
| Emptying rate | Linear, rapid | Sigmoid curve with a lag phase |
| Mechanism | Primarily gastric-duodenal pressure gradient | Requires trituration to <2 mm particles first |
| Lag phase | Minimal | Present (time for fundal accommodation + trituration) |
Once solid particles are triturated and suspended in gastric liquid, both phases empty at similar rates. Isotonic solutions empty fastest; both hypotonic and hypertonic solutions empty more slowly.
- Yamada's Textbook of Gastroenterology, 7th ed.
4. Regulation - What Controls Emptying Rate?
The chart below shows how meal composition dramatically affects emptying speed. Fat (oleate) empties slowest; simple saline empties fastest:
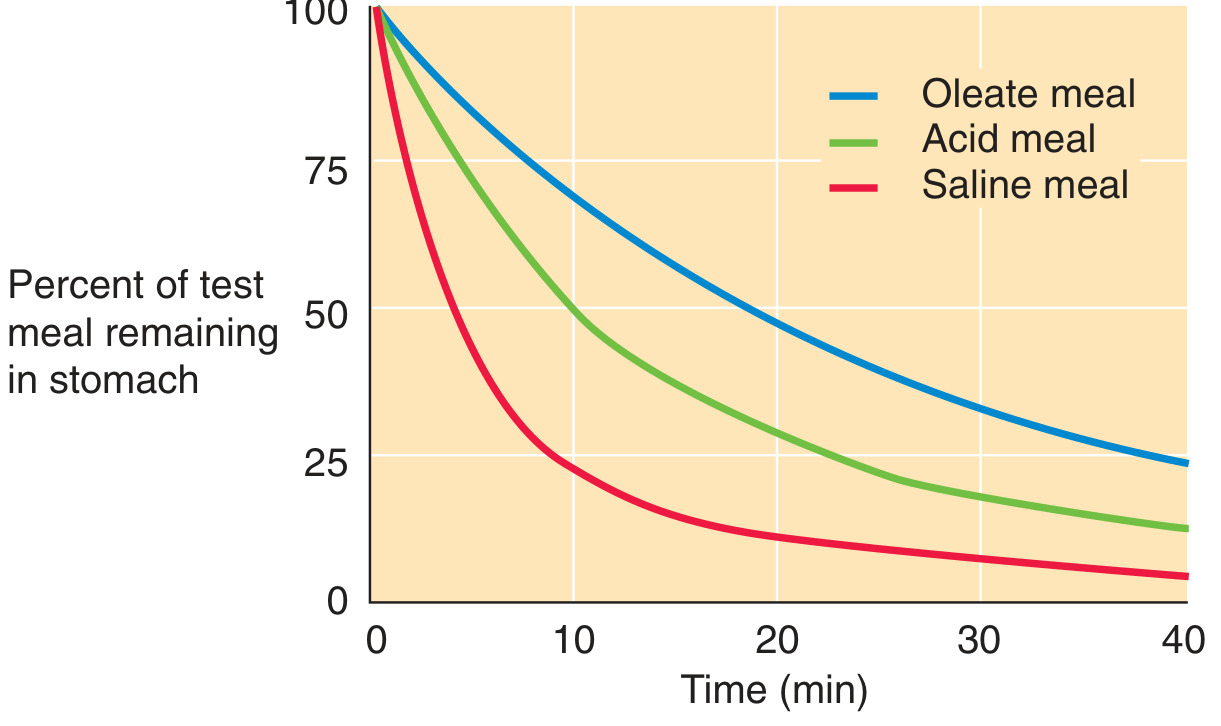
Figure: Percent of test meal remaining vs. time (min). Medical Physiology, Fig. 42-14
Factors that SLOW gastric emptying (most important):
| Factor | Mediator | Mechanism |
|---|---|---|
| Fat (fatty acids) in duodenum | CCK released from duodenal I-cells | CCK inhibits gastric contractions; ensures slow fat delivery for digestion |
| Low pH (H+ ions) in duodenum | Enteric nervous system reflexes | Duodenal H+ receptors relay signal via myenteric plexus interneurons to slow gastric smooth muscle |
| High osmolarity | Neural + hormonal (secretin, GIP) | Chemoreceptors in proximal small intestine trigger inhibitory reflexes |
| High caloric content / amino acids (tryptophan) | Vagus nerve, secretin, CCK, GIP | Ileal brake mechanism |
| Mechanical distension of duodenum | Duodenogastric reflex | Mechanoreceptors slow delivery to prevent duodenal overload |
| Hyperglycemia | Direct inhibition of gastric smooth muscle | Blood glucose >275 mg/dL significantly delays emptying |
| Female sex hormones (progesterone) | Reduced gastric muscle contractility | Explains slower emptying in females and in the luteal phase |
- Costanzo Physiology 7th Edition; Medical Physiology (Boron & Boulpaep)
5. Interdigestive Phase - The MMC
Between meals, the stomach is cleared of any residue by the migrating myoelectric complex (MMC), which occurs at ~90-minute intervals. Large particles (>2 mm) that were retained during the digestive period are eventually swept into the duodenum during the interdigestive MMC that begins ~2 hours or more after eating.
6. Disorders of Gastric Emptying
A. Delayed Gastric Emptying - Gastroparesis
Definition: Chronic motility disorder with symptoms of delayed emptying in the absence of mechanical obstruction.
Symptoms: Nausea (92%), vomiting (84%), abdominal bloating (75%), early satiety (60%), abdominal pain (46%). Late postprandial vomiting of undigested food is characteristic.
Common causes:
- Diabetic autonomic neuropathy (most common identifiable cause)
- Idiopathic (largest group overall)
- Post-surgical (post-vagotomy, post-gastrectomy)
- Hypothyroidism, connective tissue disease
- Medications: opioids, anticholinergics, TPN-related hyperglycemia
Diagnosis: 4-hour gastric emptying scintigraphy using a radiolabelled solid meal is the gold standard. Other options include wireless motility capsule and 13C breath test. Medications that affect emptying (opioids, anticholinergics, prokinetics) must be stopped 72 hours before testing.
B. Rapid Gastric Emptying - Dumping Syndrome
Definition: >70% emptying at 1 hour post-meal (using a standardised low-fat meal).
Classically seen after: Gastrectomy, truncal vagotomy with drainage procedure (affects up to 20% of patients). Mechanisms include loss of fundic accommodation, reduced gastric capacity, loss of pyloric control, and bypass of duodenal feedback.
Early dumping (within 1 hour): Rapid delivery of hyperosmolar content to the small intestine causes fluid shifts into the gut lumen - bloating, crampy pain, explosive diarrhea. Reduced plasma volume triggers release of vasoactive substances - lightheadedness, sweating, flushing, tachycardia.
Late dumping (1-3 hours): Rapid carbohydrate delivery triggers an excessive insulin response, leading to reactive hypoglycemia - weakness, palpitations, diaphoresis.
Other causes of rapid emptying: Cyclic vomiting syndrome, autonomic dysfunction, early type 2 diabetes, some patients with functional dyspepsia.
- Yamada's Textbook of Gastroenterology, 7th ed.
Summary
| Concept | Key Point |
|---|---|
| Normal emptying time | ~3 hours for a mixed meal |
| Particle size threshold | <2 mm to pass through pylorus |
| Fastest emptying | Isotonic saline (liquid) |
| Slowest emptying | Fat-rich meal |
| Main braking hormones | CCK (fat), Secretin (acid), GIP |
| Delayed emptying disorder | Gastroparesis (nausea, vomiting, early satiety) |
| Rapid emptying disorder | Dumping syndrome (post-surgical) |
| Interdigestive clearance | MMC every ~90 minutes |
This is a shared conversation. Sign in to Orris to start your own chat.