Lab diagnosis of TB refer microbiology book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have all the key content I need. Let me compile the comprehensive answer from Jawetz Medical Microbiology.
Laboratory Diagnosis of Tuberculosis
Source: Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition
Key Principle
A positive tuberculin test does not prove active disease caused by tubercle bacilli. Isolation of the organism provides definitive proof.
1. Specimens
Specimens collected depend on the site of disease:
- Pulmonary TB: Fresh sputum (3 consecutive morning samples preferred), gastric washings (especially in children who cannot produce sputum)
- Extrapulmonary TB: Pleural fluid, CSF, urine, joint fluid, biopsy material, blood
- Disseminated/miliary TB: Blood cultures
2. Decontamination and Concentration
Sputum and specimens from non-sterile sites must be:
- Liquefied with N-acetyl-L-cysteine (NALC)
- Decontaminated with NaOH (kills contaminating bacteria and fungi)
- Neutralized with buffer
- Concentrated by centrifugation
Specimens from sterile sites (e.g., CSF) need only direct centrifugation - no decontamination required.
3. Smear Microscopy (Acid-Fast Staining)
A. Ziehl-Neelsen (ZN) Stain
- Classic carbolfuchsin stain - mycobacteria appear red against a blue background
- Based on the acid-fast property: once stained, organisms resist decolorization with acid-alcohol due to high mycolic acid content in cell wall
- Sensitivity ~30-40% for smear-positive TB
B. Fluorochrome Stain (Preferred)
- Auramine-rhodamine stain - mycobacteria fluoresce yellow-orange
- More sensitive than ZN stain and is the preferred method for clinical material
- LED fluorescence microscopes (some battery-powered) have extended this method to resource-limited settings
Note: Gastric washings and urine smears are generally not recommended because saprophytic mycobacteria may be present and give false positives.
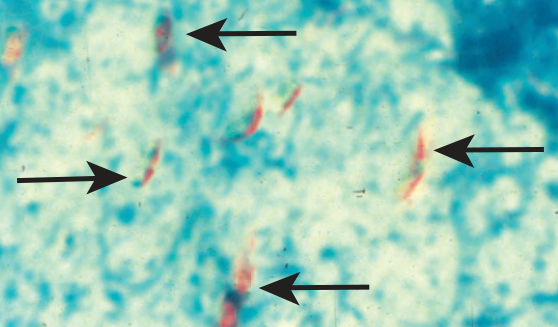
Figure 23-1 A: ZN-stained sputum showing M. tuberculosis (arrows) as red rods on blue background. B: Auramine O fluorescence staining showing two fluorescent M. tuberculosis. (Courtesy of G Cunningham.)
4. Culture
A. Media
| Type | Examples | Features |
|---|---|---|
| Semisynthetic agar | Middlebrook 7H10, 7H11 | Defined salts, oleic acid, albumin, glycerol; 7H11 also has casein hydrolysate |
| Egg-based agar | Lowenstein-Jensen (LJ) | Whole egg, glycerol, malachite green (inhibits contaminants); standard nonselective medium |
| Liquid broth | Middlebrook 7H9, BACTEC MGIT | Fastest recovery; most sensitive |
- Both selective (with antibiotics to prevent overgrowth) and nonselective media should be used
- Incubation at 35-37°C in 5-10% CO2 for up to 8 weeks
- If results are negative with a positive smear, or if slowly-growing NTM is suspected: incubate a set at a lower temperature (24-33°C) for 12 weeks
B. Colony Characteristics of M. tuberculosis
- Slow-growing: doubling time ~18 hours; colonies appear in 2-8 weeks
- Buff/cream-coloured, rough, wrinkled ("breadcrumb" or "cauliflower" colonies) on LJ
- Non-pigmented (nonchromogen)
- Produces niacin and catalase (heat-labile catalase) - important biochemical tests
C. Runyon Classification (Traditional)
| Group | Pigment | Growth | Examples |
|---|---|---|---|
| Photochromogens (I) | Only in light | Slow | M. kansasii, M. marinum |
| Scotochromogens (II) | In light & dark | Slow | M. scrofulaceum, M. gordonae |
| Nonchromogens (III) | None | Slow | M. avium complex, M. tuberculosis |
| Rapid growers (IV) | Variable | Fast (≤7 days) | M. fortuitum, M. chelonae |
D. Identification Methods
Conventional (now largely historical):
- Rate of growth, colony morphology, pigmentation, biochemical profiles (niacin, nitrate reduction, catalase, urease)
- Requires 6-8 weeks
Modern/Molecular:
- DNA probes - species-level ID within days of a positive culture
- HPLC (High-Performance Liquid Chromatography): mycolic acid profiling - available in reference labs
- MALDI-TOF MS (Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry): species-level ID
- Pyrosequencing
E. Blood Cultures (for MAC/disseminated)
- Two methods: lysis centrifugation system OR commercially available broth media for blood cultures
5. Susceptibility Testing
- Standardized broth culture technique for first-line drugs
- Agar-based technique (reference labs) for first- and second-line drugs
- MODS assay (Microscopic Observation Drug Susceptibility): multi-well plate, examines for M. tuberculosis "cording" - used widely outside the US
- First-line drugs: INH, rifampicin, pyrazinamide, ethambutol
- Second-line drugs: kanamycin, capreomycin, ethionamide, cycloserine, fluoroquinolones
6. Nucleic Acid Amplification Tests (NAATs)
- Permit rapid, direct detection of M. tuberculosis in clinical specimens
- GeneXpert MTB/RIF (Cepheid): Real-time multiplex PCR
- Detects M. tuberculosis complex AND rifampin resistance mutations simultaneously
- Sensitivity: 98.2% for smear-positive specimens; 72.5% for smear-negative
- Specificity: 99.2%
- Faster than culture (results in ~2 hours vs. weeks)
- Earlier FDA-cleared commercial assays (Amplified MTD test, Amplicor) also available
7. Tuberculin Skin Test (TST / Mantoux)
Material
- PPD (Purified Protein Derivative) - chemically fractionated from old tuberculin
- Standardized in Tuberculin Units (TU): 1 TU (first strength), 5 TU (standard/intermediate), 250 TU (second strength)
Technique
- 0.1 mL injected intracutaneously (Mantoux method), volar aspect of forearm
- Read at 48-72 hours - measure induration (not erythema)
Interpretation (CDC cut-points)
| Induration | Positive for |
|---|---|
| ≥ 5 mm | HIV-infected persons; recent contacts of active TB; fibrotic changes on CXR consistent with old TB; immunosuppressed patients |
| ≥ 10 mm | Recent immigrants from high-prevalence countries; injection drug users; residents of high-risk congregate settings; healthcare workers; children <4 years old |
| ≥ 15 mm | Low-risk persons |
- Becomes positive within 4-6 weeks after infection
- BCG vaccination may cause false-positive TST
8. Interferon-Gamma Release Assays (IGRAs)
More specific than TST, especially in BCG-vaccinated individuals.
Mechanism
- Detect interferon-γ released by sensitized CD4 T cells in response to M. tuberculosis-specific antigens:
- ESAT-6 (Early Secretory Antigenic Target-6)
- CFP-10 (Culture Filtrate Protein-10)
- TB7.7
- These antigens are absent from BCG and most NTM - hence higher specificity
Available Assays
| Assay | Method | Specimen |
|---|---|---|
| QuantiFERON-TB Gold In-Tube (QFT-GIT) | ELISA - detects IFN-γ | Whole blood |
| T-SPOT.TB | ELISpot - counts IFN-γ producing T cells | Peripheral blood mononuclear cells (PBMCs) |
- Results reported as positive, negative, or indeterminate
- Not recommended in severely immunocompromised hosts or children < 5 years
- Comparable to TST for detecting latent TB infection
- Advantage over TST: Not affected by BCG vaccination
9. Molecular Typing / Genotyping (Epidemiological)
Used for outbreak investigation, tracking transmission, distinguishing reactivation from reinfection:
- IS6110 RFLP (Restriction Fragment Length Polymorphism): Gold standard historically; based on variable positions of insertion sequence IS6110 in M. tuberculosis chromosome
- Spoligotyping: PCR-based, targets direct repeat locus
- MIRU-VNTR (Mycobacterial Interspersed Repetitive Units - Variable Number Tandem Repeats): Replacing IS6110 typing; faster
- Done at CDC, state health labs, and research labs
Summary Algorithm
Suspect TB
|
Collect appropriate specimen
|
├── Smear (ZN / Auramine-rhodamine) → Rapid, cheap, but ~50-80% sensitive
|
├── Culture (LJ / BACTEC MGIT) → Gold standard; 2-8 weeks
|
├── NAAT (GeneXpert MTB/RIF) → Rapid (<2h), detects rifampin resistance
|
├── Tuberculin skin test (TST/PPD) → Latent TB screening
|
└── IGRA (QFT-GIT / T-SPOT.TB) → Latent TB; better in BCG-vaccinated
Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed., Chapter 23 - Mycobacteria
This is a shared conversation. Sign in to Orris to start your own chat.