Hi
Hey! How can I help you today?
Pelvic girdle pain
Reading File
Finding Sources
Searching PubMed
"pelvic girdle pain" AND treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
pelvic girdle pain diagnosis management clinical features 2025
Reading File
Reading File
Here is a thorough overview of pelvic girdle pain (PGP) based on authoritative medical textbooks:
Pelvic Girdle Pain (PGP)
Definition and Overview
Pelvic girdle pain refers to pain localized to the pelvic ring - involving the sacroiliac joints (SIJs), pubic symphysis, and associated ligamentous and muscular structures. It can occur in isolation or as part of a broader syndrome (e.g., pregnancy-related PGP or polymyalgia rheumatica). Distinguishing true PGP from low back pain remains clinically challenging, though a detailed structured approach helps.
Major Clinical Contexts
1. Pregnancy-Related PGP (Most Common)
As noted in Bradley and Daroff's Neurology in Clinical Practice, more than half of pregnant women report low back and/or pelvic girdle pain, with prevalence rising after the 5th month.
Contributing factors:
- Increasing lumbar lordosis
- Direct pressure from the enlarging uterus
- Postural stress
- Hormonally induced ligamentous laxity (progesterone/relaxin)
Women with severe pregnancy-related PGP (causing work absence) have high rates of recurrence in subsequent pregnancies and in the non-gravid state.
2. Sacroiliac Joint (SIJ) Syndrome
From Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e:
Pain pattern:
- In the region of the affected SIJ and medial buttock
- May radiate to the groin, posterior thigh, and occasionally below the knee
Physical examination findings:
- Tenderness over the sacroiliac sulcus
- Reduced joint mobility
- Reproduction of pain on provocative testing
Diagnostic tests:
| Test | Description |
|---|---|
| FABER / Patrick's | Flexion, Abduction, External Rotation |
| Gaenslen's | Hip extension stress on SIJ |
| Yeoman's | Prone hip extension with knee flexion |
| Iliac distraction (gapping) | Lateral compression stress |
| Thigh thrust (posterior shear) | Posterior force through hip |
| Sacral thrust | Direct sacral pressure |
| Gillet (stork) test | Single-leg stance assessment |
Diagnosis is confirmed by: symptoms + pain on ≥3 provocative tests + positive response to SIJ injection.
3. PGP in Polymyalgia Rheumatica (PMR)
PMR classically presents with symmetric shoulder and pelvic girdle pain plus prominent morning stiffness, typically in patients over 50. As described in Rheumatology (2022, Elsevier), the pelvic girdle is one of the two characteristic pain distributions in PMR.
Labs: Elevated ESR (≥40 mm/hr) and CRP are typical. IL-6 is the most sensitive activity marker.
Management
Pregnancy-Related PGP
| Approach | Evidence |
|---|---|
| Tailored strengthening exercises | Beneficial effect reported |
| Pelvic tilt exercises | Helpful |
| Water gymnastics | Beneficial |
| Acupuncture | Better results than physiotherapy in some studies (Elden et al., 2005) |
| Physiotherapy | Small but positive benefit |
| Pelvic support belts | A 2025 systematic review (PMID 40716213) evaluated pelvic belts for low back and pelvic pain during pregnancy |
A 2025 systematic review (PMID 39922568) confirmed that exercise in the postpartum period reduces musculoskeletal pain and disability.
SIJ Syndrome
| Treatment | Notes |
|---|---|
| Physical therapy / chiropractic manipulation | Widely used; limited large RCT data |
| Intra-articular steroid injection | Methylprednisolone 40-60 mg; relief up to 2-3 months; fluoroscopy guidance preferred |
| Combined intra- and extra-articular injection | More effective than intra-articular alone |
| Radiofrequency ablation (RFA) | Option for refractory cases |
| Surgical fusion | Reserved for severe, refractory SIJ dysfunction |
Cranial spread on dye study improves short-term efficacy; 2-3 injections per year can provide relief lasting up to 9 months.
Key Differentials
- Low back pain (discogenic, muscular)
- Piriformis syndrome
- Hip pathology (OA, labral tears)
- Polymyalgia rheumatica
- Spondyloarthropathy (ankylosing spondylitis, psoriatic arthritis)
- Sciatica / lumbar radiculopathy
Recent Evidence (2024-2026)
- Pelvic belts in pregnancy (2025) - Systematic review on pelvic belt efficacy for low back and pelvic pain during pregnancy
- Postpartum exercise (2025) - Exercise reduces musculoskeletal pain in the postpartum period
- Flares in pelvic girdle pain (2026) - Scoping review on understanding flare patterns in spinal and pelvic girdle pain
Summary: PGP is a common, multifactorial condition. In pregnancy, conservative management (exercise, acupuncture, pelvic belts, physiotherapy) is the mainstay. In SIJ syndrome, a stepwise approach from physical therapy to injections to RFA/surgery is used. PMR-related PGP responds dramatically to glucocorticoids. Accurate diagnosis depends on structured physical examination and targeted provocative testing.
Diagrams
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here are all the key diagrams from the medical library related to pelvic girdle pain:
Diagram 1 - Pelvic Girdle Anatomy (Anterosuperior View)
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
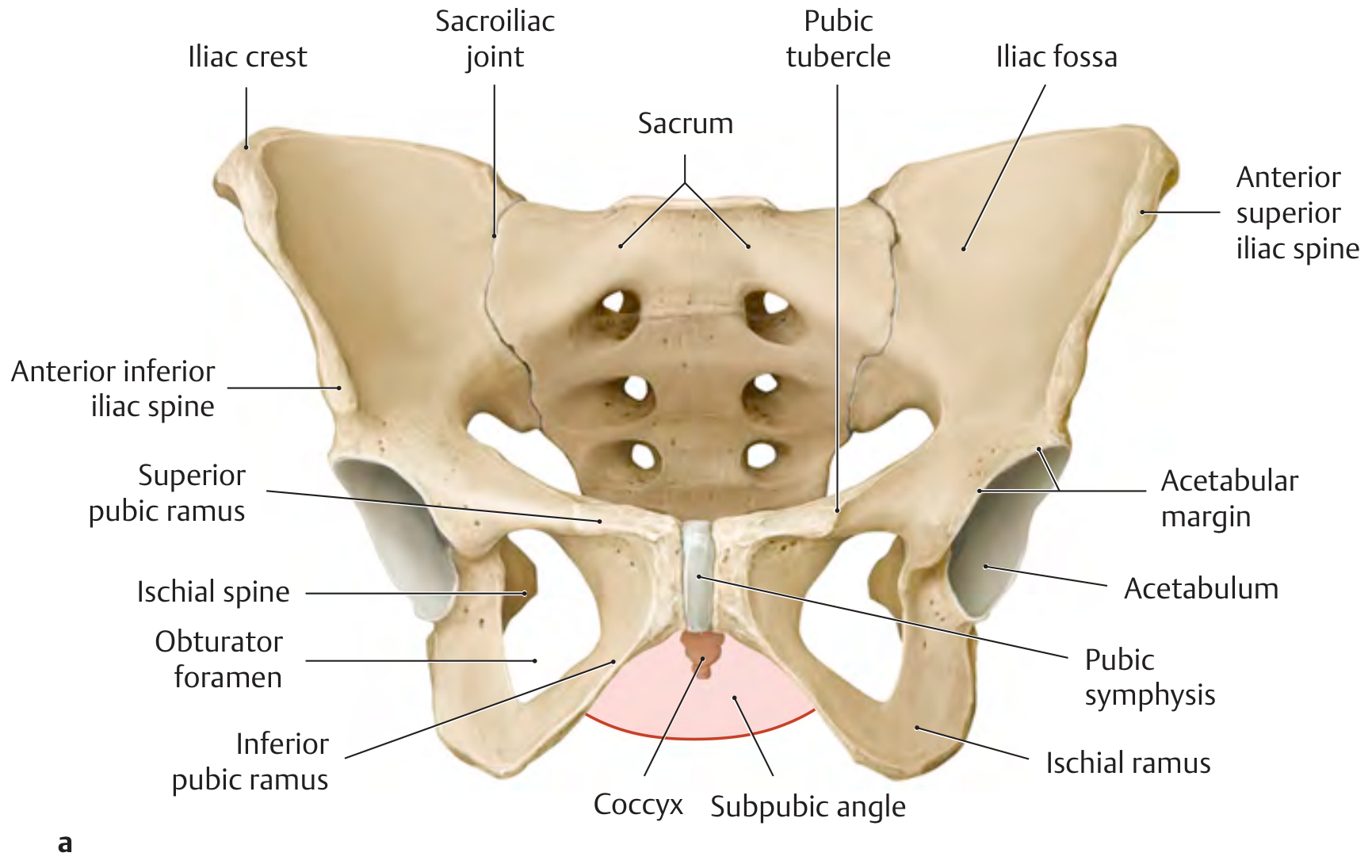
This labeled diagram shows all key bony landmarks: iliac crest, sacroiliac joints, sacrum, pubic symphysis, acetabulum, obturator foramen, coccyx, and subpubic angle. The pubic symphysis and sacroiliac joints are the two sites most commonly affected in PGP.
Diagram 2 - The Pelvic Ring (Anterior View)
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
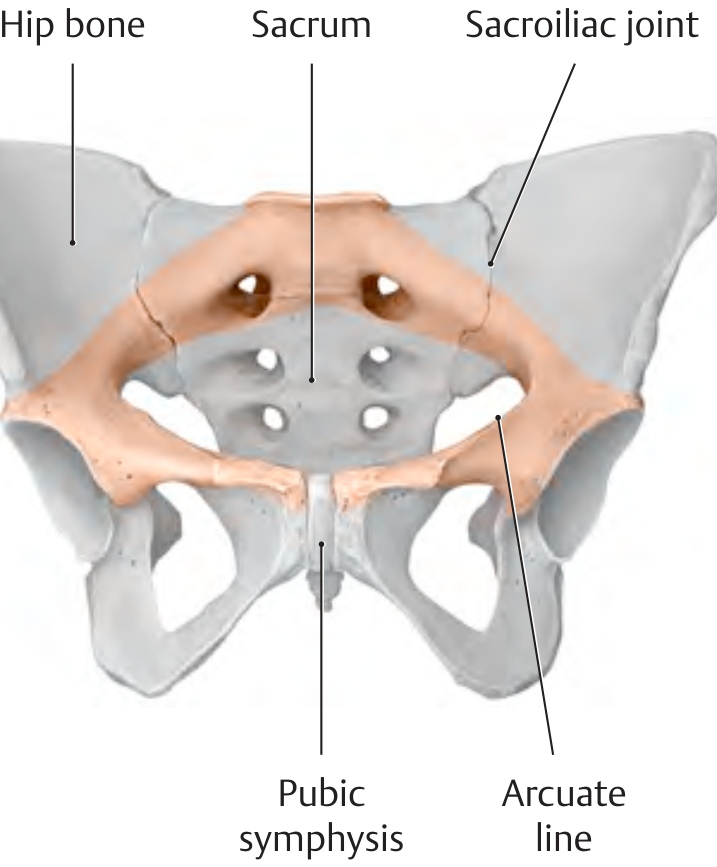
Shows the pelvic ring (highlighted in orange) formed by the two hip bones, sacrum, sacroiliac joints, and pubic symphysis. The ring transmits trunk load to the lower limbs - instability here is the root cause of PGP.
Diagram 3 - Pelvic Ligaments (Anterior + Posterior Views)
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
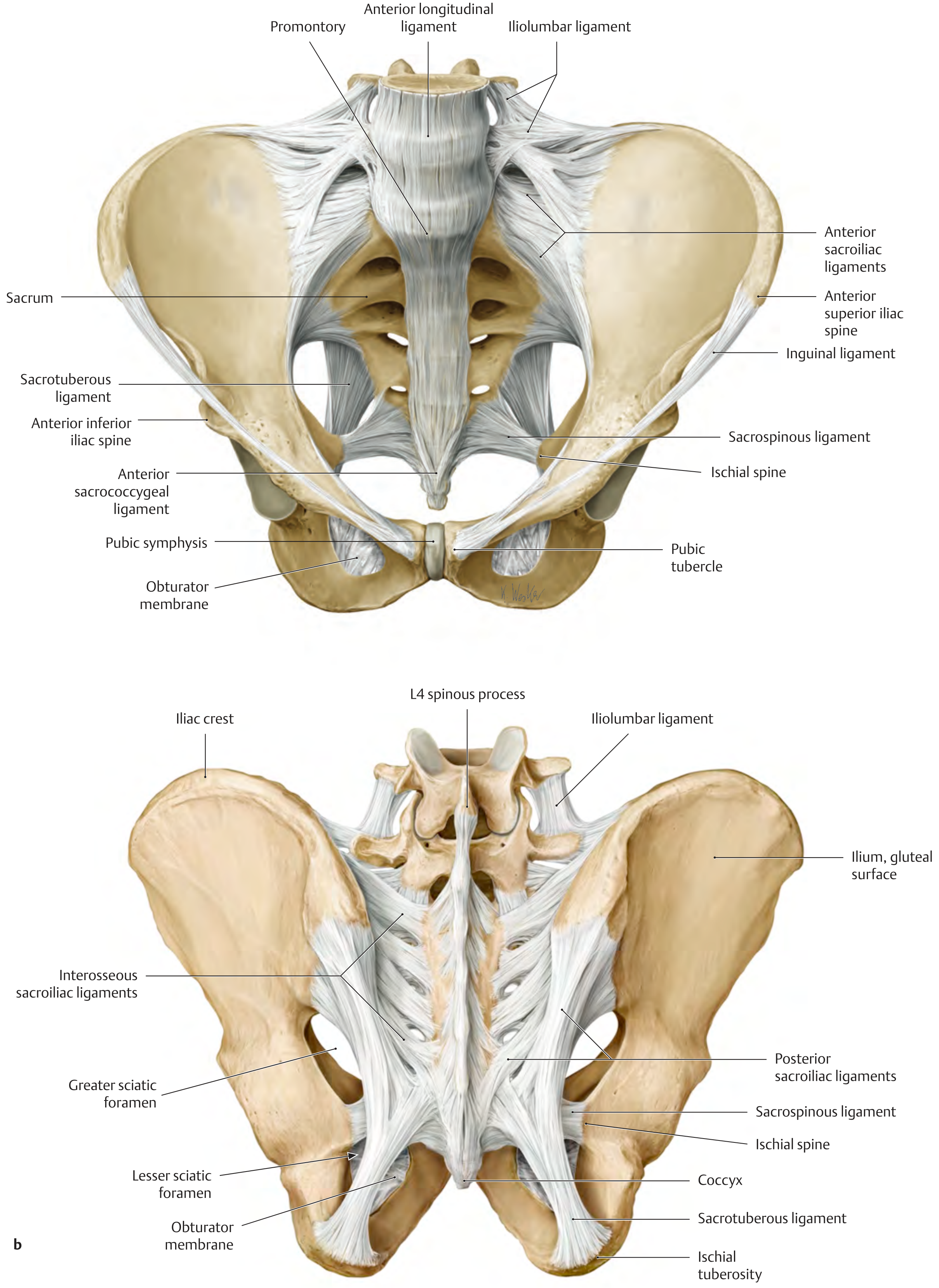
These detailed views show the ligaments critical to pelvic girdle stability:
- Anterior: Anterior sacroiliac ligaments, iliolumbar ligament, sacrospinous ligament, sacrotuberous ligament, inguinal ligament
- Posterior: Posterior sacroiliac ligaments, interosseous sacroiliac ligaments, iliolumbar ligament
Laxity of these ligaments (especially in pregnancy due to relaxin) is a major contributor to PGP.
Diagram 4 - Pain Distribution in Polymyalgia Rheumatica (PMR)
Source: Rheumatology, 2-Volume Set (2022, Elsevier)
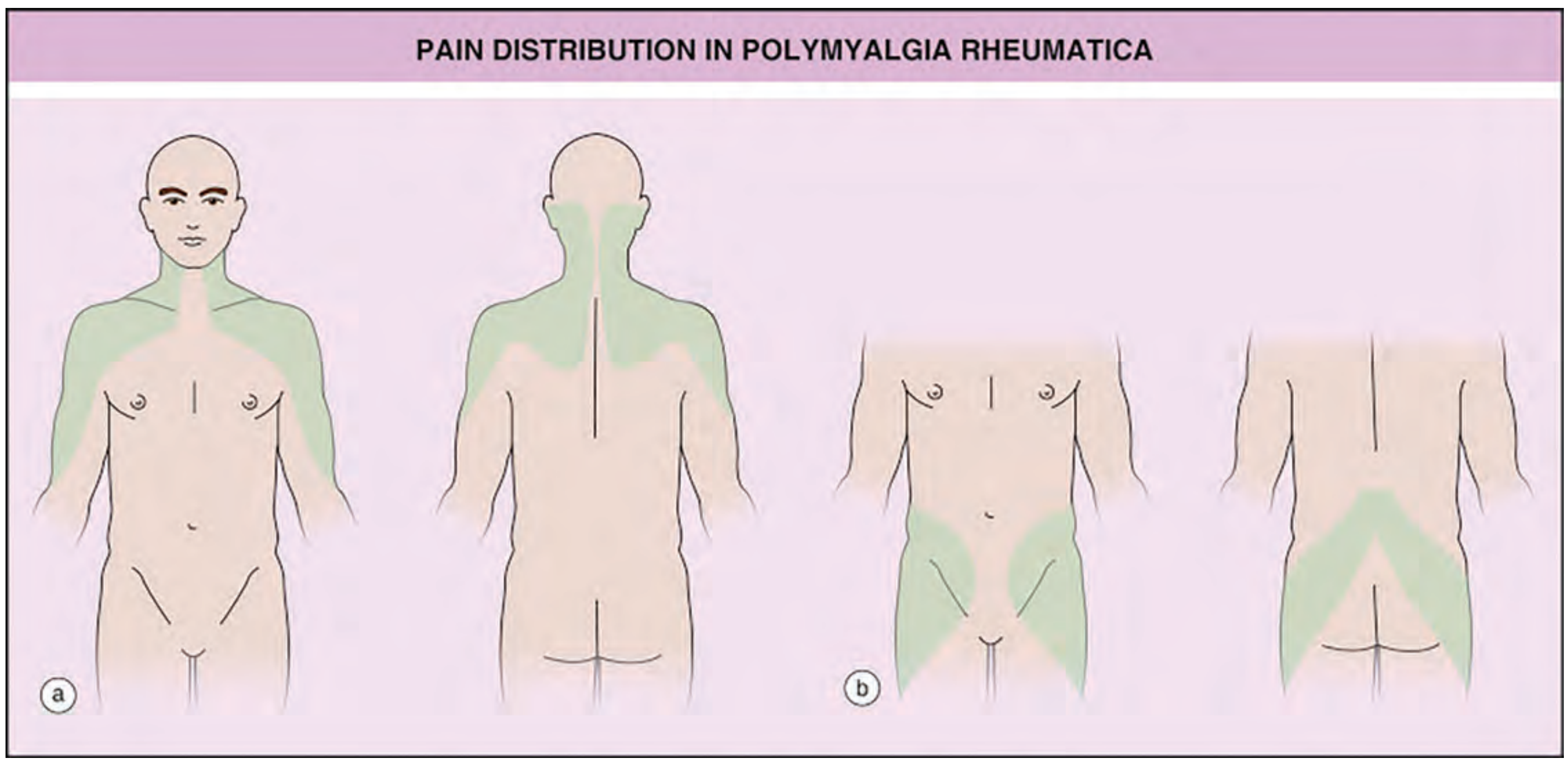
(a) Shoulder girdle and neck pain distribution; (b) Pelvic girdle pain distribution - showing the anterior and posterior shading over the hips, groins, and buttocks. This is the classic bilateral, symmetric pattern of PMR-related PGP.
Diagram 5 - Sacroiliac Joint Injection (Fluoroscopy)
Source: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
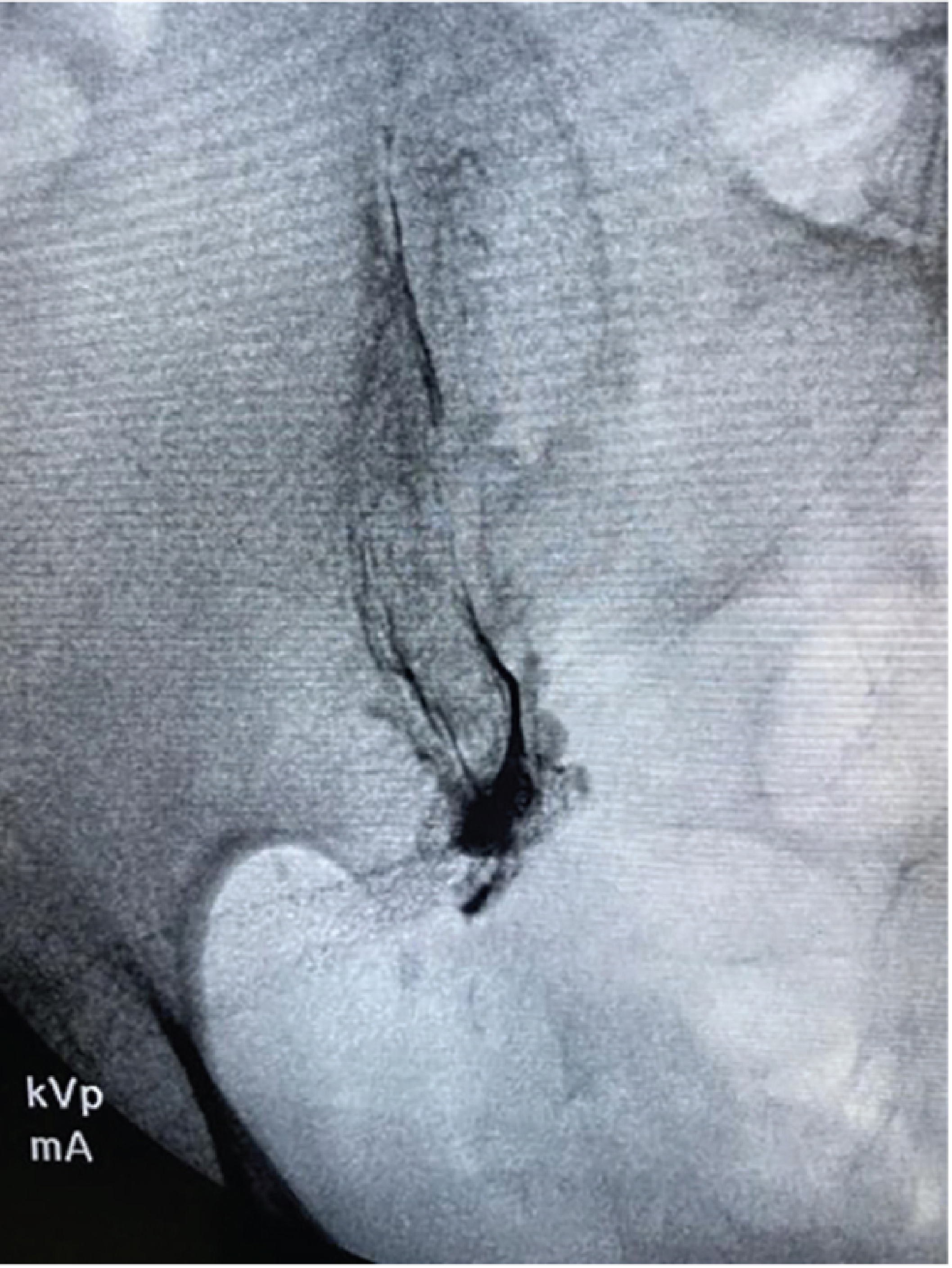
Fluoroscopic image showing SIJ injection with needle entry at the inferior joint margin and cranial spread of contrast dye. Cranial spread is associated with improved short-term efficacy.
Diagram 6 - Radiofrequency Denervation Target Points for SIJ Pain
Source: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
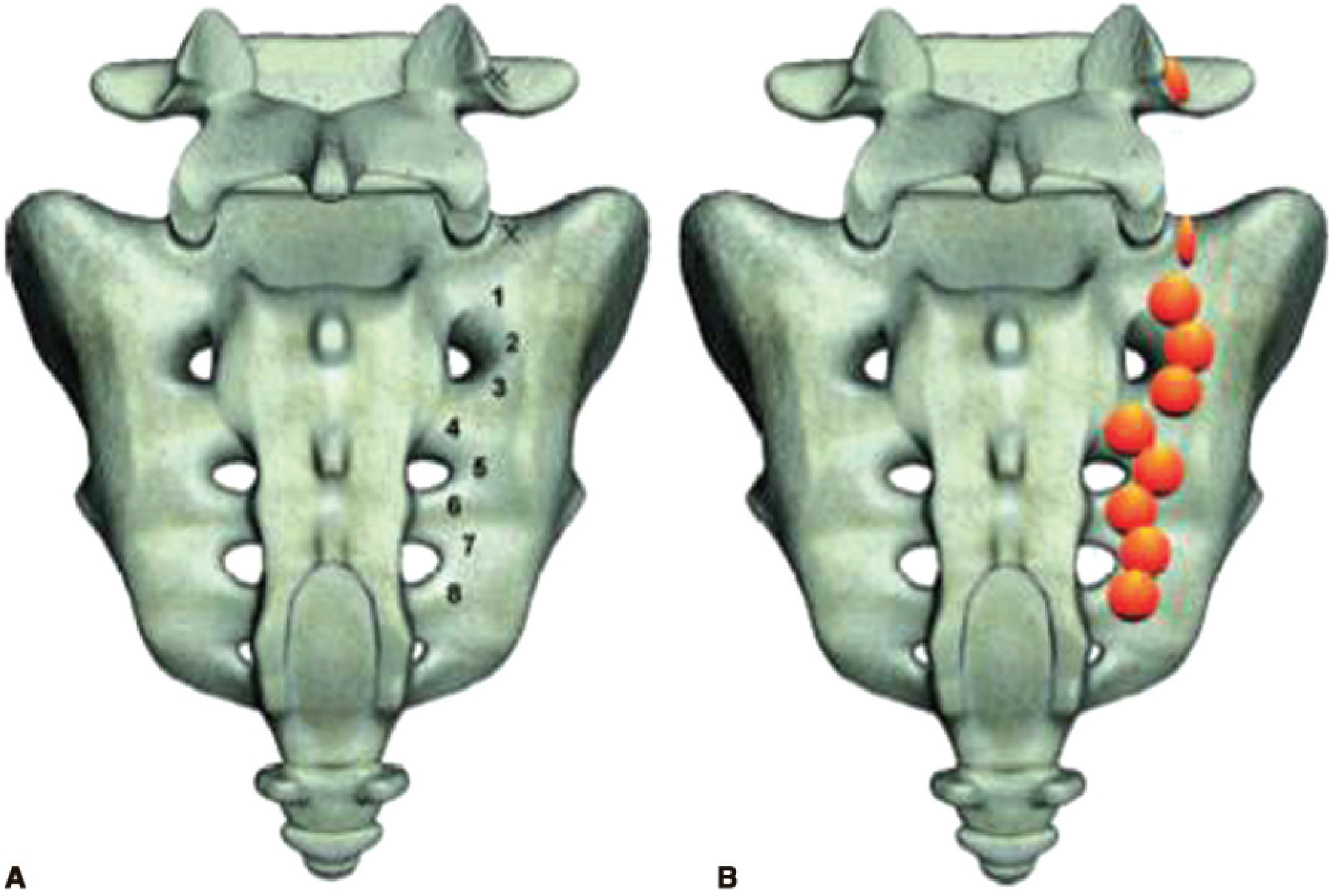
(A) Numbered target points along the right SIJ for water-cooled radiofrequency denervation at the L5 medial branch and S1-S3 lateral branches. (B) Expected lesion distribution (orange spheres). Used in refractory SIJ pain when injections provide only temporary relief.
This is a shared conversation. Sign in to Orris to start your own chat.