Kernohans notch phenomenon vs kernohan woltman sign
Reading File
Finding Sources
Searching the Web
Kernohan notch phenomenon vs Kernohan Woltman sign difference false localizing
Reading File
Reading File
Reading Web Page
https://litfl.com/kernohan-woltman-notch-phenomenon
Loading Image
Here is a thorough breakdown of both terms, sourced from Adams & Victor's Principles of Neurology, Localization in Clinical Neurology, and Plum & Posner.
Kernohan's Notch vs. Kernohan-Woltman Sign/Phenomenon
These two terms describe the same pathological event but from different vantage points - one anatomical, one clinical. They are often used interchangeably, which causes confusion.
The Core Mechanism (shared by both)
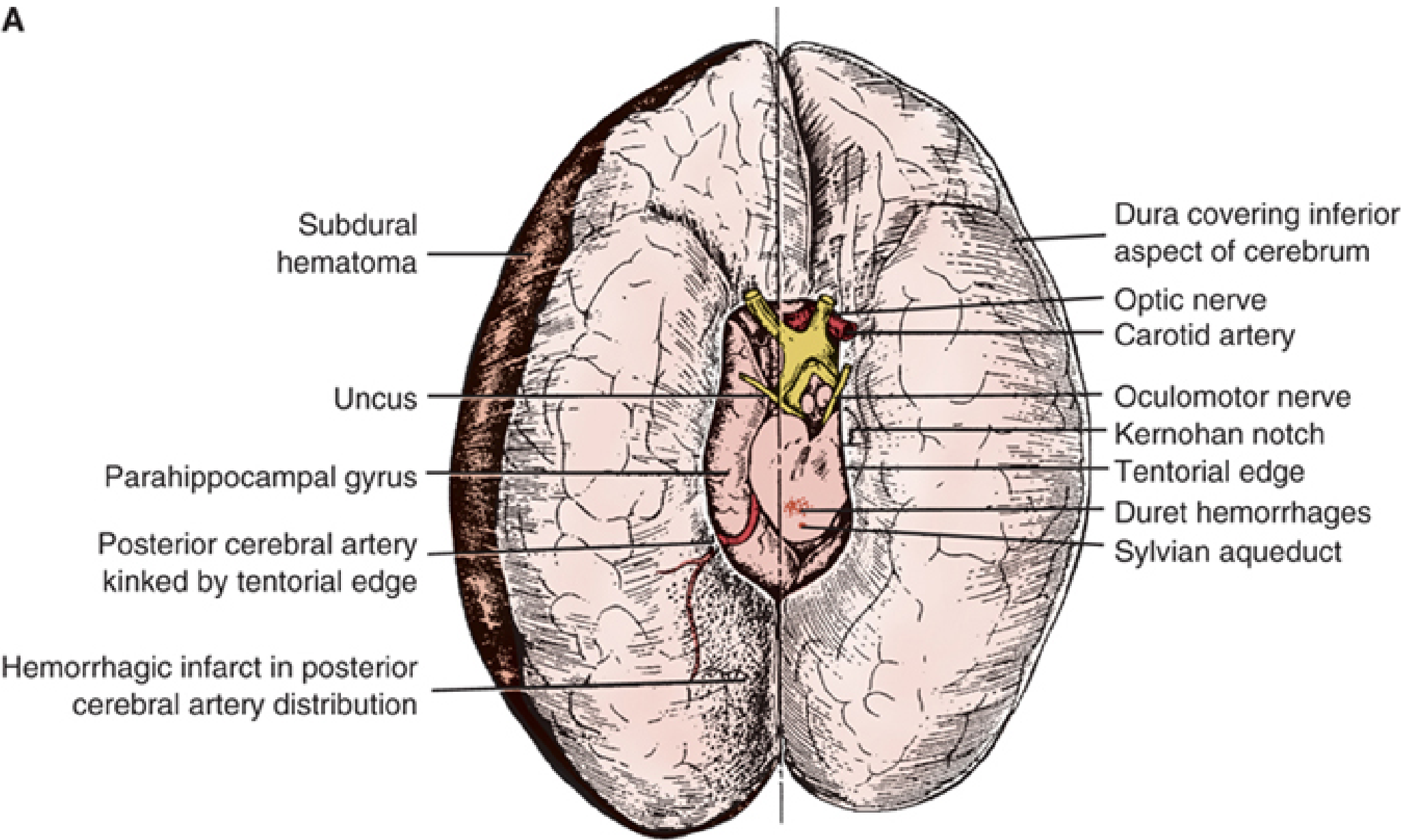
In uncal (lateral transtentorial) herniation, a supratentorial mass (e.g., subdural hematoma, temporal lobe tumor, ICH) pushes the medial temporal lobe (uncus + parahippocampal gyrus) medially and downward through the tentorial notch. This forces the midbrain laterally, so that the contralateral cerebral peduncle (crus cerebri) is pressed against the hard, unyielding free edge of the tentorium cerebelli on the opposite side.
Kernohan's Notch (the anatomical finding)
| Feature | Detail |
|---|---|
| What it is | A physical groove/indentation carved into the lateral midbrain (cerebral peduncle) by the rigid tentorial edge |
| Location | On the side opposite the primary lesion (contralateral peduncle compressed against ipsilateral tentorial edge) |
| How seen | At autopsy or on MRI (T2 signal change / focal deformity in the cerebral peduncle contralateral to mass) |
| Nature | Purely structural/pathological - an indentation in neural tissue |
As Adams & Victor's states: "the upper midbrain is pushed against the opposite edge of the tentorium (the Kernohan notch or, more properly, the Kernohan-Woltman phenomenon)" - note this textbook itself acknowledges "Kernohan notch" is the loosely used but less precise term.
Kernohan-Woltman Sign / Phenomenon (the clinical finding)
| Feature | Detail |
|---|---|
| What it is | Ipsilateral hemiparesis (weakness on the same side as the primary lesion) |
| Mechanism | The notch disrupts the corticospinal tract in the contralateral peduncle. Because corticospinal fibers decussate in the medulla, damaging the contralateral peduncle produces weakness ipsilateral to the original lesion |
| Why it matters | It is a false localizing sign - the weakness appears on the wrong side, misleading clinicians into thinking the lesion is contralateral to the hemiparesis |
| Classic triad | Ipsilateral dilated pupil (CN III compression) + ipsilateral hemiparesis (Kernohan-Woltman) + decreased consciousness |
| Associated signs | Ipsilateral Babinski sign; later, extensor posturing on the ipsilateral side |
| Nature | Purely clinical |
From Localization in Clinical Neurology: "This rigid structure carves out a notch (Kernohan notch) in the lateral aspect of the midbrain, interrupting the cerebral peduncle... This results in hemiparesis ipsilateral to the original lesion (Kernohan notch phenomenon). If misinterpreted, such hemiparesis may prove to be a false localizing sign."
Side-by-Side Comparison
| Kernohan's Notch | Kernohan-Woltman Sign/Phenomenon | |
|---|---|---|
| Domain | Pathoanatomy / Radiology | Clinical neurology |
| What is described | The physical indentation in the cerebral peduncle | The clinical symptom (ipsilateral hemiparesis) |
| Detected by | Autopsy or MRI | Neurological examination |
| Side | Contralateral peduncle is notched | Ipsilateral weakness relative to the mass |
| Historical name | "Incisura of the crus" (Kernohan & Woltman, 1929) | Kernohan-Woltman phenomenon |
| Term precision | Less precise when used alone | More precise, preferred in neurology literature |
A Word on Terminology Confusion
The LITFL eponymous review highlights that "Kernohan's notch" is used in two completely separate contexts:
- Neurological (the one above) - indentation of the cerebral peduncle from tentorial edge in uncal herniation.
- Ophthalmological - a distinct 1953 finding by Rucker & Kernohan describing indentation of the optic chiasm by overlying arteries in pituitary tumors, with no associated motor symptoms.
Key Clinical Pearl
When you see ipsilateral pupil dilation + ipsilateral hemiparesis, the lesion is on the side of the abnormal pupil - not the opposite side. The pupil tells the truth (CN III is compressed directly by the herniating uncus ipsilaterally), while the hemiparesis is the false localizer. This is the bedside lesson of the Kernohan-Woltman phenomenon.
Sources: Localization in Clinical Neurology, 8e, p. 1453 | Adams and Victor's Principles of Neurology, 12e, p. 384 | LITFL - KWNP
This is a shared conversation. Sign in to Orris to start your own chat.