St elivasion ecg
Reading File
Finding Sources
Finding Sources
Searching Images
ST elevation ECG STEMI pattern
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of ST-Segment Elevation (STE) on ECG.
ST-Segment Elevation on ECG
What Is It?
ST-segment elevation (STE) represents abnormal elevation of the ECG tracing between the end of the QRS complex (J point) and the start of the T wave. It reflects transmural myocardial injury current — the affected myocardium is depolarized/injured and cannot fully repolarize like normal tissue.
Diagnostic Criteria for STEMI
According to Goldman-Cecil Medicine (2024):
| Lead Group | Threshold for STE |
|---|---|
| V2–V3 in men | ≥ 2 mm (0.2 mV) at J point |
| V2–V3 in women | ≥ 1.5 mm (0.15 mV) at J point |
| All other contiguous limb/chest leads | ≥ 1 mm (0.1 mV) in ≥ 2 contiguous leads |
A 12-lead ECG must be obtained within 10 minutes of patient arrival. Emergency reperfusion (primary PCI or fibrinolysis) should be initiated immediately if criteria are met.
ECG Evolution of STEMI (Three Phases)
1. Early Acute (Hyperacute) Phase — minutes to hours
- T waves increase in amplitude and widen → hyperacute T waves
- ST segments evolve: concave → straightened → convex upward
- Blended ST-T complex may produce a "tombstone" morphology
- Reciprocal ST depression appears in leads opposite the injury zone (marker of larger infarct and worse prognosis)
2. Evolved Acute Phase — hours to days
- ST elevation begins to regress
- T waves invert in affected leads
- Pathologic Q waves develop (≥ 0.03 sec wide, ≥ 0.1 mV deep, in ≥ 2 contiguous leads)
3. Chronic (Stabilized) Phase — weeks to months
- ST may normalize or persist (persistent STE suggests ventricular aneurysm)
- Q waves may persist or resolve (complete normalization is uncommon)
Anterior STEMI — ECG Sequence
(Harrison's Principles of Internal Medicine, 22E)
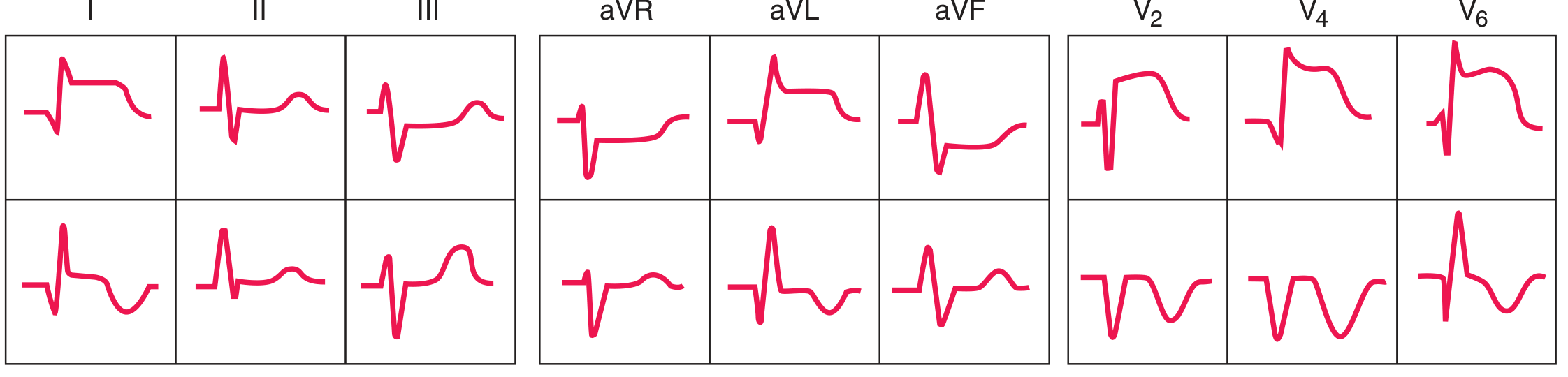
Top row = Acute phase (ST elevation in anterior leads). Bottom row = Evolving phase (T-wave inversion, Q waves developing in V2/V4).
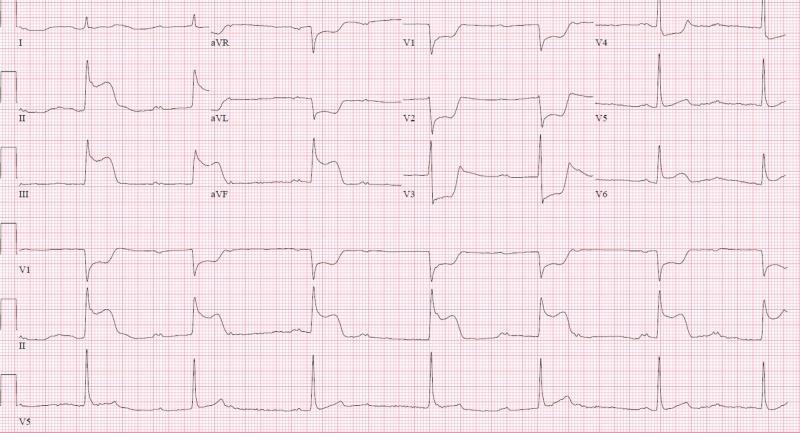
Anterolateral STEMI (LAD Occlusion)

Convex ST elevation in V1–V6 + leads I and aVL. Reciprocal ST depression in II, III, aVF. Hyperacute peaked T waves in V2–V4. Suggests proximal LAD occlusion.
Inferior STEMI (RCA or LCx Occlusion)
Coved (convex) ST elevation in II, III, aVF. Reciprocal depression in V1–V6, I, aVL. Suggests RCA or LCx occlusion. Always order right-sided leads (V3R/V4R) to exclude RV infarction.
Localizing the Infarct by Leads
| Leads with STE | Territory | Likely Artery |
|---|---|---|
| V1–V4 | Anterior / Septal | LAD (proximal) |
| V1–V6 + I, aVL | Anterolateral | LAD (proximal) |
| I, aVL (±V5–V6) | Lateral | LCx or Diagonal |
| II, III, aVF | Inferior | RCA (80%) or LCx (20%) |
| ST ↓ in V1–V3 (reciprocal) | Posterior | LCx or PDA |
| V1 + STE in inferior leads | RV infarction | Proximal RCA |
Differential Diagnosis of ST Elevation (Non-STEMI Causes)
(Washington Manual of Medical Therapeutics)
Cardiac:
- Acute pericarditis — diffuse STE, concave ("saddle-shaped"), PR depression, no reciprocal changes
- Myocarditis
- Brugada syndrome — coved STE in V1–V2
- LV aneurysm — persistent STE weeks after MI
- Hypertrophic cardiomyopathy
- Coronary vasospasm (Prinzmetal's angina, cocaine)
- Early repolarization (normal variant) — concave STE, J-point notching, common in young males
Non-cardiac:
- Pulmonary embolism — may produce STE in V1, aVR
- Hyperkalemia — peaked T waves + wide QRS
Distinguishing STEMI from Pericarditis
| Feature | STEMI | Pericarditis |
|---|---|---|
| STE shape | Convex / tombstone | Concave (saddle-shaped) |
| Distribution | Regional (≥2 contiguous leads) | Diffuse (all leads except aVR/V1) |
| PR segment | Normal | PR depression |
| Reciprocal changes | Yes | No (except in aVR/V1) |
| Q waves | Develop over time | Absent |
⚠️ Fibrinolysis is contraindicated in pericarditis and can be hazardous — always exclude it before treating as STEMI.
ECG Pitfalls and Masking
- LBBB — can mask ST changes; new LBBB in appropriate clinical context = STEMI equivalent
- Ventricular pacing — obscures ST analysis
- WPW preexcitation — can simulate ST changes
- Posterior MI — appears as ST depression in V1–V3 (reciprocal); extend leads to V7–V9 to reveal posterior STE
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.