Hypertension bp 200/110 management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertensive crisis" OR "hypertensive emergency" management treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
hypertensive emergency BP 200/110 management guidelines 2024 IV antihypertensives
Reading File
I now have comprehensive information from authoritative sources. Let me compile the full response.
Hypertension with BP 200/110 mmHg - Management
A BP of 200/110 mmHg is severely elevated and must be immediately classified as either a hypertensive emergency (with target organ damage) or hypertensive urgency (without target organ damage) - this distinction drives all management decisions.
Step 1: Immediate Classification
| Feature | Hypertensive Emergency | Hypertensive Urgency |
|---|---|---|
| BP threshold | >180/110 mmHg | >180/110 mmHg |
| Target organ damage | Present | Absent |
| Setting | ICU/HDU admission | Outpatient or ED |
| Route of drug | IV | Oral |
| Rate of BP reduction | Controlled, over minutes-hours | Gradual, over 24-48 h |
The 2024 ESC guidelines define hypertensive emergency as BP ≥180/110 mmHg with evidence of acute hypertensive mediated organ damage (HMOD). The 2024 AHA scientific statement uses >180/110-120 mmHg with new/worsening target organ damage.
Step 2: Assess for Target Organ Damage (TOD)
Evaluate all of these systems urgently:
| Organ | Signs/Symptoms to look for | Investigation |
|---|---|---|
| Brain | Altered mental status, headache, focal deficits, seizures, visual changes | CT head, MRI if PRES suspected |
| Heart | Chest pain, dyspnea, S3, pulmonary edema | ECG, troponin, CXR, echo |
| Kidneys | Oliguria, haematuria, rising creatinine | Urine dipstick, serum creatinine, urine protein |
| Eyes | Blurred vision, papilledema | Fundoscopy (mandatory for BP >180/110) |
| Aorta | Tearing chest/back pain, pulse asymmetry | CT aortogram |
| Eclampsia | Pregnancy, seizures, proteinuria | Urine protein, fetal monitoring |
Approximate incidence of TOD: Heart 27-49%, Brain 37-45%, Kidney 15%, Aortic dissection 1-2%, Eclampsia 2% (Rosen's Emergency Medicine).
Step 3: Management by Scenario
A. Hypertensive Emergency (TOD present) - IV Treatment Required
Admission to ICU/HDU with continuous BP monitoring is mandatory.
BP reduction goal:
- Reduce MAP by no more than 20-25% in the first 1-2 hours
- Then gradually to 160/100-110 mmHg over 2-6 hours
- Exception: Acute aortic dissection - target SBP <120 mmHg within minutes
Avoid rapid BP drops - too-fast reduction causes cerebral hypoperfusion and watershed ischemia. The British and Irish Hypertension Society advises maintaining DBP above 100 mmHg except in aortic syndromes.
IV Drug Choices by Target Organ Involved
| Clinical Scenario | Preferred IV Drug(s) | Drugs to Avoid |
|---|---|---|
| Hypertensive encephalopathy | Labetalol, nicardipine, clevidipine | Nitroprusside (increases ICP) |
| Ischemic stroke | Labetalol, nicardipine (only if BP >220/120 or thrombolysis planned) | Aggressive lowering in most ischemic strokes |
| Intracranial hemorrhage | Nicardipine, labetalol (target SBP <140 mmHg) | - |
| Acute coronary syndrome | Nitroglycerin, esmolol | Hydralazine, diazoxide |
| Acute pulmonary edema / heart failure | Nitroglycerin, clevidipine, nitroprusside | Beta-blockers |
| Aortic dissection | Labetalol or esmolol (heart rate control first), then nicardipine/nitroprusside | Direct vasodilators alone (cause reflex tachycardia) |
| Eclampsia/pre-eclampsia | Labetalol, hydralazine, nicardipine | ACE inhibitors, ARBs (teratogenic) |
| Acute kidney injury (hypertensive) | Nicardipine, fenoldopam, labetalol | NSAIDs |
| Sympathomimetic crisis / phaeochromocytoma | Phentolamine (alpha-blocker), nicardipine | Beta-blockers alone (worsen HTN via unopposed alpha) |
Key IV Antihypertensive Drugs - Summary Table
| Drug | Class | Dose | Onset | Notes |
|---|---|---|---|---|
| Nicardipine | CCB (dihydropyridine) | 5 mg/hr IV, up to 15 mg/hr | 5-10 min | Most widely used; safe in most emergencies |
| Labetalol | Alpha + Beta blocker | 20 mg IV bolus q10 min, or 1-2 mg/min infusion | 5 min | Avoid in acute HF, severe asthma |
| Clevidipine | CCB (ultra-short acting) | 1-2 mg/hr, titrate to 32 mg/hr | 2-4 min | Excellent BP control; use with caution in egg allergy |
| Esmolol | Beta-1 blocker (ultra-short) | 500 mcg/kg bolus, then 50-300 mcg/kg/min | 1 min | Aortic dissection, perioperative HTN |
| Nitroprusside | Nitric oxide vasodilator | 0.3-10 mcg/kg/min | Seconds | Cyanide toxicity risk with prolonged use |
| Nitroglycerin | Nitric oxide vasodilator | 5-100 mcg/min | 2-5 min | Best for ACS and pulmonary edema |
| Hydralazine | Vasodilator | 10-20 mg IV q4-6h | 10-20 min | Eclampsia; unpredictable; reflex tachycardia |
| Phentolamine | Alpha-blocker | 5-10 mg IV bolus | 1-2 min | Phaeo, cocaine/amphetamine overdose |
| Enalaprilat / Fenoldopam | ACE inhibitor / DA-1 agonist | Various | Variable | Renal protection (fenoldopam) |
(Lippincott Pharmacology; Rosen's Emergency Medicine; PMC systematic review [PMID: 11389756])
B. Hypertensive Urgency (No TOD) - Oral Treatment
- Restart or intensify oral antihypertensives
- Do NOT use sublingual nifedipine (causes unpredictable, rapid drops)
- Options: amlodipine, captopril, labetalol orally, clonidine
- Aim for gradual reduction over 24-48 hours
- Arrange close outpatient follow-up within 1-7 days
- Identify and address precipitating factors (non-adherence, dietary salt, drugs)
Step 4: Long-Term / Maintenance Antihypertensive Treatment
Once the acute crisis is managed and the patient is stable, transition to oral therapy targeting BP <130/80 mmHg (ACC/AHA 2017) or <130/80 mmHg (2024 ESC):
First-line drug classes (any two or three may be combined):
- Thiazide/thiazide-like diuretics (chlorthalidone, indapamide)
- ACE inhibitors / ARBs (especially with CKD, diabetes, proteinuria)
- Calcium channel blockers (amlodipine) - particularly in older adults and Afro-Caribbean patients
- Beta-blockers (if co-existent heart failure, post-MI, tachyarrhythmia)
Non-pharmacological measures (all patients):
- Sodium restriction to ~2 g/day (~5 g salt/day)
- DASH diet
- Weight reduction if overweight
- Aerobic exercise
- Alcohol reduction
- Smoking cessation
About two-thirds of patients with severe hypertension will need two or more drugs to reach target BP. Combination therapy allows lower individual doses and better tolerability. (Braunwald's Heart Disease)
Step 5: Investigate Secondary Causes
A BP of 200/110 - especially if resistant or onset in younger patients - warrants exclusion of:
- Renovascular hypertension (renal artery stenosis) - renal Doppler, CT/MR angiography
- Primary hyperaldosteronism - serum aldosterone:renin ratio
- Phaeochromocytoma - 24-h urine metanephrines
- Cushing syndrome - overnight dexamethasone suppression test
- Coarctation of aorta - BP difference between arms/legs, echo
- Sleep apnoea - Epworth Sleepiness Scale, polysomnography
- Hypothyroidism/hyperthyroidism - TFTs
- Drug-induced (NSAIDs, OCPs, sympathomimetics, steroids, cocaine)
Quick Reference: Hypertensive Emergency Algorithm
BP ≥180/110 mmHg
|
v
Assess for TOD (clinical + bloods + ECG + fundoscopy)
|
_____|_____
| |
TOD present No TOD
| |
EMERGENCY URGENCY
(ICU/HDU) (ED/Outpatient)
IV drugs Oral drugs
Max 25% MAP Reduce over 24-48h
drop in 1-2h
Key principle: The rate and target of BP reduction matter as much as the drug chosen. Never drop BP too fast - autoregulation must adjust.
Sources:
- Rosen's Emergency Medicine, Chapter 70 - Hypertensive Emergencies
- Lippincott Illustrated Reviews: Pharmacology, Section XV - Hypertensive Emergency
- Braunwald's Heart Disease - Hypertension Management in Older Adults
- 2024 ESC Hypertension Guidelines - acute management of hypertensive emergencies
- 2024 AHA Scientific Statement on Elevated BP in Acute Care (PMID: 38560900)
- Systematic review: Management Strategies for Hypertensive Crisis - IV drug preferences
Emergency hypertension management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertensive emergency" management treatment
Searching the Web
hypertensive emergency management 2024 guidelines IV drugs organ-specific treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
I have all the content I need for a comprehensive, well-illustrated answer. The algorithm image is excellent. Now I'll compose the full response.
Hypertensive Emergency - Emergency Management
Definition & Classification
Hypertensive emergency = BP ≥180/110 mmHg with new or worsening target organ damage (TOD)
Hypertensive urgency = BP ≥180/110 mmHg without TOD
This distinction is the single most important decision point - it determines where, how fast, and with what you treat.
Step 1: Clinical Algorithm
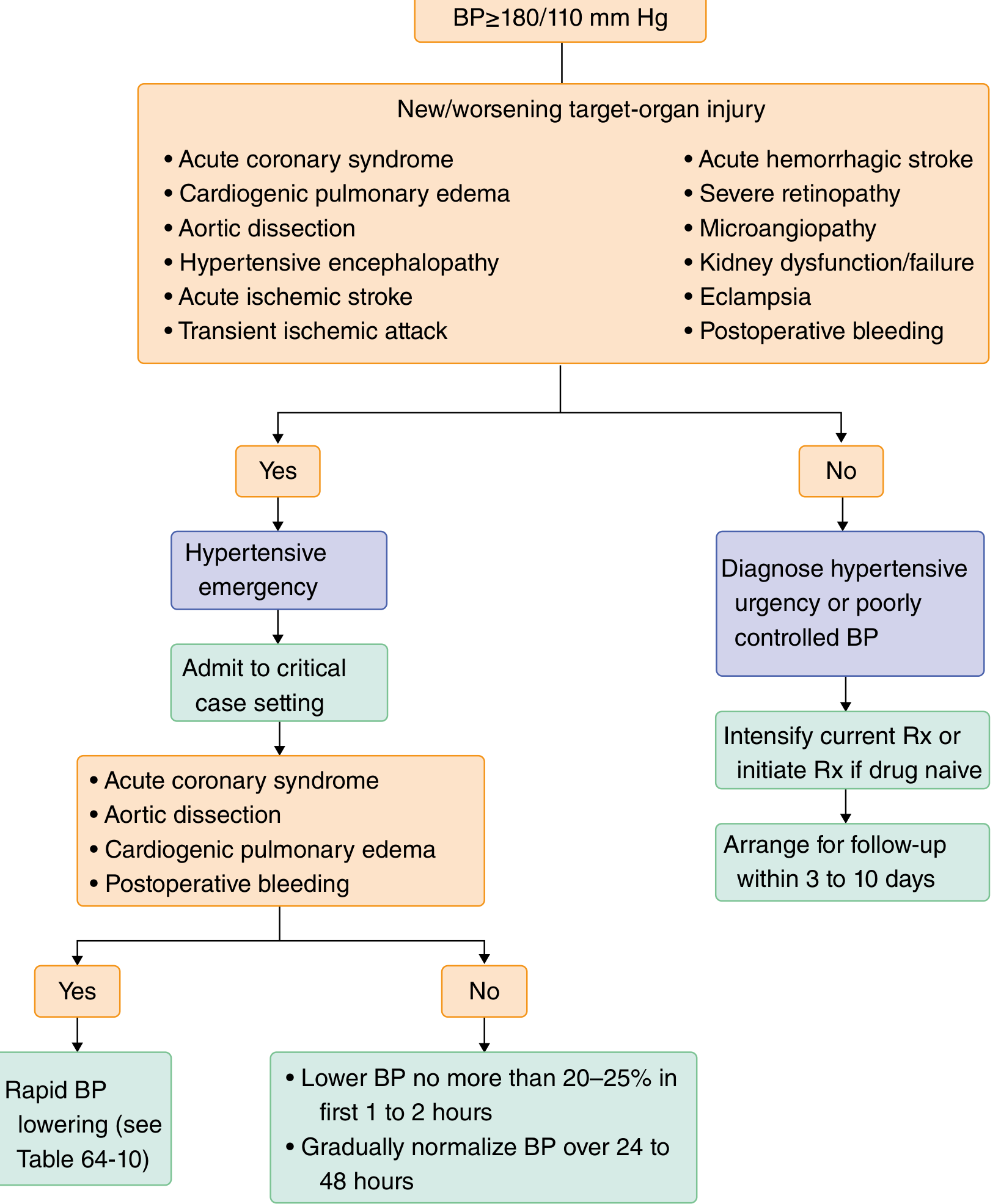
(Goldman-Cecil Medicine, Fig 4.5 - Algorithm for diagnosing and treating hypertensive emergency)
Step 2: Immediate Assessment
Do all of these simultaneously:
| Assessment | What to Look For |
|---|---|
| History | Duration, missed meds, cocaine/sympathomimetics, pregnancy, previous BP |
| Vitals | Confirm BP in both arms (difference >20 mmHg suggests aortic dissection) |
| Neuro exam | Altered consciousness, focal deficits, papilledema, visual loss |
| Cardiac exam | S3/S4, pulmonary crackles, JVD (heart failure) |
| Fundoscopy | Papilledema, flame hemorrhages, cotton-wool spots, exudates (mandatory if BP >180/110) |
| ECG | LVH, ischemia, strain pattern |
| Labs | FBC, creatinine, electrolytes, urinalysis (casts/proteinuria), troponin |
| Imaging | CXR (pulmonary edema), CT head (hemorrhage/stroke), CT aorta if dissection suspected |
Target organs involved (approximate frequency):
- Brain: 37-45% (ischemic stroke 6-25%, intracranial hemorrhage 5-23%, encephalopathy 8-16%)
- Heart: 27-49% (acute pulmonary edema 14-37%, ACS 11-12%)
- Kidneys: 15% (AKI 8%)
- Aortic dissection: 1-2%
- Eclampsia: 2%
(Rosen's Emergency Medicine, Ch. 70)
Step 3: Hypertensive EMERGENCY Management
Where to Treat
ICU or High Dependency Unit (HDU) - mandatory for continuous hemodynamic monitoring and titratable IV therapy.
BP Reduction Goals - Core Principle
The goal is NOT to normalize BP rapidly. Reduce MAP by no more than 20-25% in the first 1-2 hours, then gradually to 160/100-110 mmHg over 2-6 hours, then normalize over 24-48 hours.
Rationale: Chronic hypertension shifts the autoregulation curve to the right. Rapid BP drops cause cerebral, coronary, and renal hypoperfusion. Sublingual nifedipine is explicitly contraindicated for this reason. (Comprehensive Clinical Nephrology, 7th Ed.)
Exceptions requiring faster/deeper reduction:
| Condition | Target BP | Timeframe |
|---|---|---|
| Aortic dissection | SBP <120 mmHg | Within minutes |
| Eclampsia / severe pre-eclampsia | SBP <140 mmHg | Within 1 hour |
| Phaeochromocytoma crisis | SBP <140 mmHg | Within 1 hour |
| ACS / acute pulmonary edema | SBP <140 mmHg | Within 1 hour |
| ICH (SBP >220) | SBP 140-180 mmHg | Within 1 hour |
| Ischemic stroke (thrombolysis candidate) | BP <185/110 | Before tPA |
| Ischemic stroke (non-thrombolysis, BP >220/120) | 15% reduction | First 24 h |
IV Drug Pharmacology Table
(Comprehensive Clinical Nephrology 7th Ed., Table 38.1 | Lippincott Pharmacology)
| Drug | Class | Dose | Onset | Duration | Key Notes |
|---|---|---|---|---|---|
| Nicardipine | CCB (DHP) | 5 mg/hr IV; increase by 2.5 mg/hr q5-15 min; max 15 mg/hr | 5-10 min | 15-30 min after stop | Most widely used; safe across most emergencies; preserves cerebral flow |
| Clevidipine | CCB (ultra-short DHP) | 1-2 mg/hr; double q90 sec; max 32 mg/hr | 2-4 min | 5-15 min | Excellent titratability; avoid in egg/soy allergy or severe aortic stenosis |
| Labetalol | α1 + β1/β2 blocker | 20 mg IV bolus q10 min; or 0.5-2 mg/min infusion | 5-10 min | 3-6 h | Favored in stroke (preserves cerebral flow); delayed offset makes it harder to titrate; avoid in acute HF/asthma |
| Esmolol | β1 blocker (ultra-short) | 500 mcg/kg bolus; 50-300 mcg/kg/min infusion | 1-2 min | 10-30 min | Ideal for aortic dissection (HR control); perioperative HTN |
| Sodium nitroprusside | NO donor (arterial + venous) | 0.3-10 mcg/kg/min | Seconds | 1-2 min | Near-instant titration; risk of cyanide toxicity >24-48h or renal failure; increases ICP - avoid in stroke/encephalopathy |
| Nitroglycerin | NO donor (venous > arterial) | 5-100 mcg/min | 2-5 min | 3-5 min | Best for ACS + pulmonary edema; tolerance develops at >48h |
| Phentolamine | Non-selective α-blocker | 5-10 mg IV bolus | 1-2 min | 10-30 min | Drug of choice: phaeochromocytoma, cocaine/amphetamine crisis |
| Hydralazine | Direct arteriolar vasodilator | 10-20 mg IV q4-6h | 10-20 min | 3-8 h | Eclampsia; unpredictable; causes reflex tachycardia; avoid in ACS/dissection |
| Fenoldopam | DA-1 agonist | 0.1-0.3 mcg/kg/min | 5-10 min | 30-60 min | Renal protective; useful with AKI |
| Enalaprilat | IV ACE inhibitor | 1.25 mg q6h IV | 15-30 min | 6-12 h | Avoid in bilateral RAS or AKI; useful for scleroderma renal crisis |
| Magnesium sulfate | NMDA antagonist | 4-6 g IV over 15-20 min, then 1-2 g/hr | Minutes | Hours | Eclampsia - seizure prophylaxis and BP control |
Organ-Specific IV Drug Selection
(Comprehensive Clinical Nephrology 7th Ed., Table 38.2 | 2024 AHA Scientific Statement | PMC systematic review)
| Emergency Type | Preferred Drug(s) | Drugs to AVOID |
|---|---|---|
| Hypertensive encephalopathy | Nicardipine, labetalol, clevidipine | Nitroprusside (raises ICP), hydralazine |
| Acute ischemic stroke | Labetalol, nicardipine, clevidipine | Nitroprusside; avoid aggressive lowering unless thrombolysis planned |
| Intracranial hemorrhage | Nicardipine, labetalol (target SBP 140-180) | Nitroprusside |
| Acute coronary syndrome | Nitroglycerin, esmolol, labetalol | Hydralazine (reflex tachycardia), diazoxide |
| Acute pulmonary edema / LVF | Nitroglycerin, clevidipine, nitroprusside | Beta-blockers |
| Aortic dissection | Esmolol or labetalol (rate control first), THEN nicardipine or nitroprusside | Direct vasodilators alone (cause reflex tachycardia, increase aortic wall stress) |
| Eclampsia / severe pre-eclampsia | Labetalol, hydralazine IV, nicardipine; magnesium for seizures | ACE inhibitors, ARBs (teratogenic) |
| Hypertensive AKI / renal crisis | Nicardipine, fenoldopam, labetalol | Diuretics (most are volume depleted); NSAIDs |
| Phaeochromocytoma | Phentolamine (alpha-block first), then esmolol for HR | Beta-blockers alone (unopposed alpha causes BP surge) |
| Cocaine/sympathomimetic | Benzodiazepines + phentolamine or nicardipine | Beta-blockers alone |
| Scleroderma renal crisis | ACE inhibitor (captopril/enalaprilat) | - |
Volume Status - Critical Point
Many patients in hypertensive emergency are volume depleted due to pressure natriuresis. Avoid diuretics unless pulmonary edema is present. IV fluid may be needed to restore perfusion and prevent a precipitous BP fall. Catecholamine-excess states (phaeo, cocaine) are particularly volume depleted. (Comprehensive Clinical Nephrology 7th Ed.)
Step 4: Hypertensive URGENCY Management (No TOD)
- No IV drugs needed
- Restart missed oral medications or intensify existing regimen
- Oral options: amlodipine, captopril 12.5-25 mg, labetalol 200 mg, clonidine 0.1 mg
- Do NOT use sublingual nifedipine - unpredictable BP drop, can cause stroke
- Target: reduce BP over 24-48 hours (not minutes)
- Arrange follow-up within 3-10 days
- If drug-naive: initiate two-drug therapy (thiazide or CCB + ACEi or ARB)
Step 5: Transition from IV to Oral Therapy
Once BP is stable in target range for 12-24 hours (allows autoregulation to re-establish):
- Gradually wean IV drug
- Start oral antihypertensive combination (CCB + ACEi/ARB ± thiazide)
- IV furosemide 20-40 mg may help when IV saline infusions or vasodilation have expanded plasma volume and blunt oral drug response (Goldman-Cecil Medicine)
- Transfer out of ICU when hemodynamically stable on oral therapy
Step 6: Investigate Secondary Causes (All Severe HTN)
| Cause | Screening Test |
|---|---|
| Renal artery stenosis | Renal Doppler, CT/MR angiography |
| Primary hyperaldosteronism | Aldosterone:renin ratio |
| Phaeochromocytoma | 24-h urine metanephrines |
| Cushing syndrome | Overnight dexamethasone suppression |
| Coarctation of aorta | BP in both arms and legs, CXR, echo |
| Drug-induced (NSAIDs, OCP, cocaine, steroids) | Medication history |
| Obstructive sleep apnoea | Epworth score, polysomnography |
Key Principles - Summary
- Classify first - emergency (TOD present) vs urgency (no TOD)
- IV drugs for emergency, oral for urgency
- Never drop BP >20-25% in first 1-2 h (except aortic dissection, eclampsia)
- Drug choice is organ-specific - no single drug fits all
- Check volume status before starting IV antihypertensives
- Never use sublingual nifedipine
- ICU/HDU admission mandatory for true emergencies
- Transition to oral after 12-24 h of stability
- Investigate secondary causes in all patients
Sources:
- Rosen's Emergency Medicine, Ch. 70 - Hypertensive Emergency
- Comprehensive Clinical Nephrology, 7th Ed., Ch. 38 - Tables 38.1 & 38.2
- Goldman-Cecil Medicine - Intravenous Medications for Hypertensive Emergencies
- Lippincott Pharmacology, Section XV - Hypertensive Emergency
- 2024 ESC Guidelines - Elevated BP and Hypertension
- 2024 AHA Scientific Statement on Elevated BP in Acute Care (PMID: 38560900, Ann Intern Med 2024)
- StatPearls - Hypertensive Emergency
This is a shared conversation. Sign in to Orris to start your own chat.