
Explain all topics in detailed required for fmge exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
FMGE cardiology hypertension emergency urgency drugs RAS guidelines 2024
Reading File
Reading File
Searching the Web
hypertensive emergency urgency drugs of choice labetalol nicardipine nitroprusside FMGE notes
Reading Web Page
hypertensive emergency urgency drugs of choice RAS beaded appearance guidelines FMGE
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile a thorough FMGE-level cardiology guide covering all the topics visible in the image.
🫀 FMGE Cardiology — Comprehensive Notes (9–12 Questions)
1. HEART FAILURE (HF)
Definition
Heart failure is a clinical syndrome resulting from the inability of the heart to meet the metabolic requirements of the body at normal filling pressures. It arises from LV systolic dysfunction, diastolic dysfunction, or both.
Key: The term "heart failure" is preferred over "congestive heart failure" because pulmonary congestion may be absent.
HFrEF vs HFpEF
| Feature | HFrEF (Systolic HF) | HFpEF (Diastolic HF) |
|---|---|---|
| EF | < 45–50% | > 45–50% |
| LV function | Reduced contraction | Impaired relaxation/filling |
| Demographics | More common in men | More common in women, elderly |
| Common causes | CAD, MI, dilated CM | HTN, obesity, DM, AF |
| Treatment | ACEi/ARB + BB + MRA + SGLT2i | Diuretics for congestion; treat comorbidities |
ACC/AHA Staging (ABCD)
| Stage | Description |
|---|---|
| A | At risk — no symptoms, no structural disease (HTN, DM, CAD) |
| B | Structural disease but no symptoms (like NYHA I) |
| C | Structural disease with current/prior symptoms (NYHA II–III) |
| D | Refractory HF despite optimal therapy (NYHA IV) |
NYHA Functional Class
- I — No symptoms with ordinary activity
- II — Mild symptoms with ordinary activity
- III — Symptoms with less-than-ordinary activity
- IV — Symptoms at rest
Left-Sided vs Right-Sided HF
| Left-Sided HF | Right-Sided HF |
|---|---|
| Dyspnea, orthopnea, PND | JVD (JVP elevation) |
| Pulmonary edema/rales | Hepatomegaly, ascites |
| S3 gallop | Peripheral pitting edema |
| Pink frothy sputum (acute) | Most common cause = left HF |
Pathophysiology
- Neurohormonal activation: RAAS (renin → angiotensin II → aldosterone) + SNS (catecholamines)
- Angiotensin II → myocyte apoptosis, hypertrophy, fibrosis
- Aldosterone → sodium retention, further fibrosis ("escapes" ACEi → need MRA)
- LV remodeling (dilation, weakening) is the central process — reversible with therapy
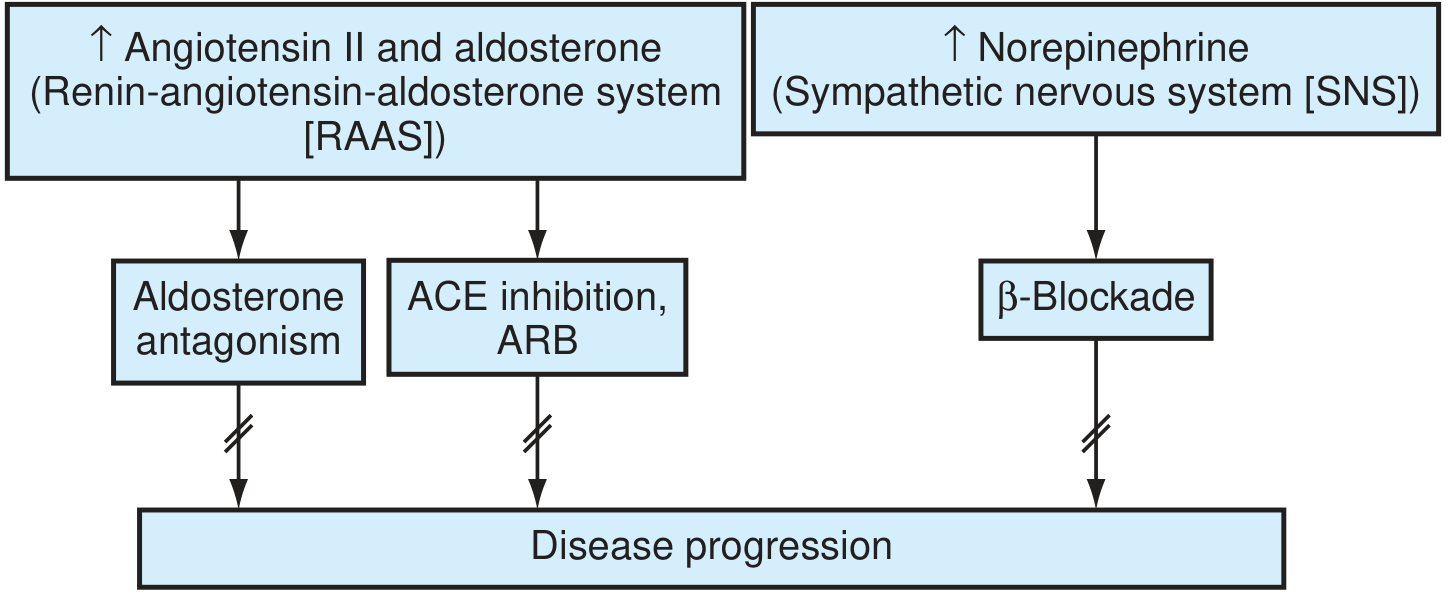
Pharmacological Management of HFrEF (FMGE High-Yield)
| Drug Class | Examples | Key Notes |
|---|---|---|
| ACE Inhibitors (DOC) | Enalapril, lisinopril, ramipril | Reduce mortality; use in all unless contraindicated |
| ARBs | Valsartan, losartan | If ACEi-intolerant (cough/angioedema) |
| Beta-blockers | Carvedilol, metoprolol succinate (XL), bisoprolol | Only FDA-approved 3; start low, titrate slowly |
| MRA (aldosterone antagonist) | Spironolactone, eplerenone | Add if EF <35%, NYHA II-IV |
| ARNI | Sacubitril/valsartan (Entresto) | Superior to ACEi in HFrEF (PARADIGM-HF trial) |
| SGLT2 inhibitors | Empagliflozin, dapagliflozin | Reduce HF hospitalization; now 1st-line |
| Diuretics | Furosemide (loop), spironolactone | Symptom relief (congestion); no mortality benefit alone |
| Digoxin | Digoxin | Reduce hospitalizations; NOT mortality benefit |
| Ivabradine | Ivabradine | HR reduction in sinus rhythm, EF ≤35% on max BB |
DOC in Acute HF: IV furosemide (loop diuretic) for decongestion
DOC for Cardiogenic Shock: Dobutamine (inotrope)
Non-pharmacologic: Salt restriction (2g/day Na), fluid restriction (1L/day), daily weight monitoring, exercise, smoking cessation, CPAP for OSA.
2. CARDIAC TAMPONADE
Definition
Accumulation of pericardial fluid that raises intrapericardial pressure → impairs cardiac filling → reduced CO → shock and death if untreated.
Key Concept
- Rapidly accumulating effusion (trauma, aortic dissection): as little as 100–200 mL → tamponade
- Slowly accumulating (malignancy): liters without tamponade (pericardium stretches)
Classic Triad — Beck's Triad
- Hypotension (↓ CO)
- JVD (↑ venous pressure)
- Muffled/distant heart sounds
Other Key Signs
- Pulsus paradoxus > 10 mmHg (↓ SBP on inspiration >10 mmHg) — hallmark
- Tachycardia, narrow pulse pressure
- Kussmaul sign absent (present in constrictive pericarditis)
Tamponade vs Constrictive Pericarditis
| Feature | Cardiac Tamponade | Constrictive Pericarditis |
|---|---|---|
| Pulsus paradoxus | Present (>10 mmHg) | Usually absent |
| Kussmaul sign | Absent | Present |
| ECG | Low voltage + electrical alternans | Low voltage |
| X-ray | Globular enlarged heart (water bottle) | Calcification of pericardium |
| Echo | RA/RV collapse, IVC dilation | Septal bounce, pericardial thickening |
| Treatment | Pericardiocentesis (emergency) | Surgical pericardiectomy |
| y-descent | Absent | Prominent |
Investigations
- ECG: Low voltage QRS + electrical alternans (pathognomonic) — heart swings in effusion
- CXR: Globular "water bottle" cardiac silhouette (>300 mL); no pulmonary venous congestion
- Echo (KEY diagnostic test): Echo-free space around heart; RA/RV diastolic collapse; dilated IVC; respiratory variation in mitral E velocity
Treatment
- Emergency: Pericardiocentesis (subxiphoid approach)
- Avoid diuretics/vasodilators (worsen filling)
- Volume resuscitation as bridge only
3. ACUTE PERICARDITIS
Causes
- Idiopathic/viral (most common ~90%), autoimmune, TB, malignancy, uremia, post-MI (Dressler syndrome)
Diagnosis — ESC Criteria (≥2 of 4)
- Pleuritic chest pain (relieved by leaning forward)
- Pericardial friction rub
- New widespread ST elevation / PR depression on ECG
- Pericardial effusion on echo
Treatment
- DOC: NSAID (aspirin 750–1000 mg TID or ibuprofen 600 mg TID) + Colchicine (0.5 mg BD × 3 months) — reduces recurrence by 50%
- Avoid steroids initially (increases recurrence)
- Steroids only for: autoimmune, TB, uraemic, refractory (prednisone 0.2–0.5 mg/kg/day)
Constrictive Pericarditis
- Causes: TB (most common worldwide), prior surgery, radiation, viral
- Features: Chronic dyspnea, JVD, Kussmaul sign, pericardia knock (S3-like), Ewart sign (dullness left lower lobe)
- Treatment: Surgical pericardiectomy
4. PLEURAL & PERICARDIAL EFFUSION IN HEART FAILURE
| Type | Feature |
|---|---|
| Pleural effusion | More common right-sided in HF; Light's criteria (transudative if protein <0.5 ratio, LDH <0.6 ratio) |
| Pericardial effusion | Echo-free space; can progress to tamponade |
5. VALVULAR HEART DISEASE
5a. MITRAL STENOSIS (MS) ★★★ (100% FMGE)
Cause: Virtually always Rheumatic Heart Disease (RHD) in India/developing world
Pathology: Fusion of commissures → fish-mouth / button hole deformity → obstructed LA outflow
Hemodynamics:
- Normal mitral valve area (MVA): 4–6 cm²
- Mild MS: MVA 1.5–2 cm²
- Severe MS: MVA < 1 cm²
- ↑ LA pressure → pulmonary hypertension → RV failure ("reactive pulmonary HTN" = 2nd stenosis)
Symptoms: Dyspnea, orthopnea, PND, hemoptysis (pulmonary venous hypertension), AF, systemic embolism
Auscultation:
- Loud S1 (pliable leaflet)
- Opening snap (OS) after S2 — shorter A2-OS interval = more severe MS
- Low-pitched diastolic rumble at apex (best heard in left lateral position, with bell)
- Presystolic accentuation (if sinus rhythm)
ECG: Left atrial enlargement (P mitrale — broad notched P), RVH if pulmonary HTN, AF
CXR: Left atrial enlargement → straightening of left heart border, double-density right border; Kerley B lines (pulmonary septal thickening); beaded appearance of pulmonary veins
Echo: DOC for diagnosis; mitral valve area by planimetry or pressure half-time; hockey-stick deformity of anterior leaflet
Treatment:
| Situation | Management |
|---|---|
| Asymptomatic, mild MS | No intervention; antibiotic prophylaxis |
| Symptoms or PAP >50 mmHg, MVA <1.5 cm² | Mechanical intervention |
| Pliable valve, no calcification, no MR ≤2+ | PMBC (Percutaneous Mitral Balloon Commissurotomy) — DOC |
| Unsuitable for PMBC | Surgical commissurotomy / MVR |
| AF + MS | Warfarin (INR 2.5–3.5); NOT DOACs |
High-yield: DOAC NOT recommended in rheumatic MS with AF — only vitamin K antagonist (warfarin)
5b. MITRAL REGURGITATION (MR) ★★★ (100% FMGE)
Causes: Rheumatic HD, MVP (commonest in West), IHD (papillary muscle dysfunction), IE, dilated CM
Acute MR (papillary muscle rupture post-MI): Medical emergency — pulmonary edema, hypotension
→ DOC: Vasodilator (nitroprusside/nitrates) + IABP → urgent surgical repair
→ DOC: Vasodilator (nitroprusside/nitrates) + IABP → urgent surgical repair
Chronic MR:
- Auscultation: Pansystolic murmur at apex, radiates to axilla; soft S1, S3 present
- ECG: LA enlargement, LV hypertrophy
- CXR: LA + LV enlargement; pulmonary congestion
- Treatment: Vasodilators (ACEi/ARBs) to reduce afterload; surgery (repair > replacement) when EF <60% or LV end-systolic dimension >40 mm
5c. AORTIC STENOSIS (AS) ★★
Causes: Senile calcification (most common >65y), bicuspid aortic valve (<65y), RHD
Symptoms: Classic triad — Angina, Syncope, Dyspnea (SAD — worst prognosis = dyspnea/HF, 1–2 yr survival)
Auscultation: Ejection systolic murmur, radiates to carotids; soft/absent A2; slow rising (parvus et tardus) pulse; reverse split S2; S4 gallop
Severe AS criteria: AVA < 1 cm², mean gradient > 40 mmHg, peak velocity > 4 m/s
Treatment:
- Symptomatic AS: Surgical aortic valve replacement (SAVR) or TAVR (transcatheter — elderly/high surgical risk)
- No vasodilators (risk of syncope)
- No prophylactic antibiotics now (except prosthetic valves)
5d. RHEUMATIC HEART DISEASE (RHD) ★★★ (100% FMGE)
Pathogenesis: Group A β-hemolytic Streptococcus pharyngitis → molecular mimicry → autoimmune cross-reaction on cardiac tissue
Jones Criteria (Major):
- Carditis (pancarditis — pericarditis, myocarditis, endocarditis)
- Polyarthritis (migratory, large joints)
- Chorea (Sydenham's)
- Erythema marginatum
- Subcutaneous nodules
Jones Criteria (Minor): Fever, raised ESR/CRP, prolonged PR, previous RHD
Diagnosis: 2 major OR 1 major + 2 minor + evidence of streptococcal infection (ASO titer, throat culture, recent scarlet fever)
Pathology of Valves:
- MS most common lesion of chronic RHD
- Aschoff bodies (granulomas with Anitschkow cells = "caterpillar cells") — pathognomonic of RHD
- Verrucae (small vegetation along line of closure)
Prophylaxis: Benzathine penicillin G 1.2 million units IM every 3–4 weeks
| Risk group | Duration |
|---|---|
| RHD without carditis | 5 years or until 21 years (whichever longer) |
| RHD with carditis but no residual HD | 10 years or until 21 years |
| RHD with persistent valvular disease | Lifelong |
ATRIAL FIBRILLATION (AF) in Valvular Disease ★★★
Mechanism in MS: LA enlargement → atrial remodeling → AF; tachycardia reduces diastolic filling → acute decompensation
Rate control (chronic AF in MS):
- Beta-blocker (metoprolol) or non-DHP calcium-channel blocker (diltiazem)
- Digoxin (elderly, low activity)
Rhythm control (recent onset AF): DC cardioversion after ≥3 weeks of anticoagulation or TEE to exclude LA thrombus
Anticoagulation in AF + MS: Warfarin (INR 2.5–3.5) — NOT dabigatran/rivaroxaban (DOACs contraindicated in rheumatic MS)
CHA₂DS₂-VASc scoring (non-valvular AF):
- CHF (1), HTN (1), Age ≥75 (2), DM (1), Stroke/TIA (2), Vascular disease (1), Age 65–74 (1), Sex (female = 1)
- ≥2 in males / ≥3 in females → oral anticoagulation
Treatment of AF (key drugs):
- Rate control: Metoprolol, diltiazem, digoxin
- Rhythm control: Amiodarone (DOC for AF + HF), flecainide (no structural HD)
- Anticoagulation: Warfarin (valvular AF) or DOACs (non-valvular AF; apixaban preferred)
- Cardioversion: DCCV or pharmacological (amiodarone, flecainide)
6. HYPERTENSION (HTN)
Classification (JNC 8 / ACC/AHA 2017)
| Category | Systolic | Diastolic |
|---|---|---|
| Normal | <120 | <80 |
| Elevated (pre-HTN) | 120–129 | <80 |
| Stage 1 HTN | 130–139 | 80–89 |
| Stage 2 HTN | ≥140 | ≥90 |
| Hypertensive crisis | ≥180 | ≥120 |
2024 ESC Guidelines: Target BP <130/80 mmHg for high-cardiovascular-risk patients
Secondary Hypertension — Renal Artery Stenosis (RAS) ★★
Causes:
- Atherosclerosis (older patients, smokers, DM)
- Fibromuscular Dysplasia (FMD) — young women, most common non-atherosclerotic cause
CXR/Angiography: "Beaded appearance" (string of beads) = characteristic of fibromuscular dysplasia of renal artery — alternating areas of stenosis and dilation in the mid-distal renal artery
Signs of RAS:
- Resistant HTN or newly worsening HTN
- Abdominal bruit
- Asymmetric kidney size on ultrasound
- ↑ Creatinine after ACEi/ARB (bilateral RAS or solitary kidney)
- Hypokalemia (↑ aldosterone secondary to ↑ renin)
Investigation: Renal Doppler ultrasound (screening); CT/MR angiography (gold standard non-invasive); Renal arteriography (gold standard invasive)
Treatment:
- Atherosclerotic RAS: Medical therapy (ACEi/ARBs, statins) preferred
- FMD: Percutaneous Transluminal Angioplasty (PTA) — DOC (without stenting)
- Severe/bilateral atherosclerotic RAS: Renal artery stenting + medical therapy
Hypertensive Urgency vs Emergency ★★★
| Feature | Hypertensive Urgency | Hypertensive Emergency |
|---|---|---|
| BP | ≥180/120 mmHg | ≥180/120 mmHg |
| Acute end-organ damage | ABSENT | PRESENT |
| Symptoms | Headache, anxiety | Chest pain, dyspnea, focal neuro deficits, oliguria |
| Management | Oral antihypertensives, reduce BP over 24–48 hours | IV antihypertensives in ICU; reduce MAP by 25% in first hour |
End organs in emergency: Brain (hypertensive encephalopathy, stroke), Heart (ACS, acute HF), Kidney (AKI), Eyes (papilledema, retinal hemorrhage), Aorta (dissection)
IV Drugs for Hypertensive Emergency ★★★
| Drug | Indication/Notes |
|---|---|
| Labetalol | DOC for most emergencies; also aortic dissection |
| Sodium Nitroprusside | Fastest acting; risk of cyanide toxicity; avoid in renal failure |
| Nicardipine | IV calcium channel blocker; safe in most situations |
| Esmolol | Aortic dissection; ultra-short acting |
| Nitroglycerine (NTG) | ACS + HTN emergency; pulmonary edema |
| Fenoldopam | Renal protective; renal failure |
| Hydralazine | Hypertensive emergency in pregnancy |
Special situations:
| Situation | Drug of Choice |
|---|---|
| Aortic dissection | Esmolol/labetalol → HR <60 bpm, SBP <120 mmHg in 5–10 min |
| Hypertensive encephalopathy | Labetalol or nicardipine |
| Acute pulmonary edema + HTN | IV nitroglycerine + loop diuretic |
| Eclampsia/HELLP | IV labetalol or hydralazine; MgSO₄ to prevent seizures |
| Acute MI + HTN | IV nitroglycerine, beta-blocker |
| Pheochromocytoma crisis | IV phentolamine (alpha-blocker) — never give BB alone first |
Oral Antihypertensives (Chronic HTN)
First-line agents (JNC 8):
- Thiazide diuretics (HCTZ, chlorthalidone)
- ACE inhibitors (especially DM/CKD)
- ARBs
- Long-acting CCBs (amlodipine)
Compelling indications:
| Comorbidity | Drug |
|---|---|
| DM / CKD (proteinuria) | ACEi or ARB |
| HFrEF | ACEi + BB + MRA + SGLT2i |
| Post-MI | ACEi + BB |
| BPH + HTN | Alpha-1 blocker (doxazosin) |
| HTN in pregnancy | Methyldopa (DOC), labetalol, nifedipine |
| Pheochromocytoma | Phenoxybenzamine (alpha-blocker, non-selective) |
Contraindications (FMGE high-yield):
- ACEi/ARBs → contraindicated in pregnancy, bilateral RAS, hyperkalemia
- Beta-blockers → asthma, COPD, heart block, Raynaud's
- Thiazides → gout (raise uric acid), hypokalemia
7. QUICK SUMMARY TABLE — FMGE High-Yield Points
| Topic | High-Yield Fact |
|---|---|
| HFrEF DOC | ACEi + BB + MRA + SGLT2i (Sacubitril/valsartan > ACEi alone) |
| HFpEF treatment | Diuretics for congestion; no mortality drug proven |
| Acute HF DOC | IV furosemide; CPAP for pulmonary edema |
| Tamponade triad | Hypotension + JVD + muffled heart sounds (Beck's) |
| Tamponade ECG | Electrical alternans + low voltage |
| Tamponade treatment | Pericardiocentesis (emergency) |
| Pericarditis DOC | Aspirin/Ibuprofen + Colchicine |
| MS DOC (intervention) | PMBC (Percutaneous Mitral Balloon Commissurotomy) |
| MS + AF anticoagulation | Warfarin (NOT DOACs) |
| RHD prophylaxis | Benzathine penicillin IM q3–4 weeks |
| Beaded appearance on angiography | Fibromuscular dysplasia (FMD) of renal artery |
| Hypertensive emergency DOC | IV Labetalol / Nitroprusside / Nicardipine |
| Aortic dissection DOC | IV Esmolol → target SBP <120, HR <60 |
| Pheochromocytoma crisis | IV Phentolamine (alpha-blocker first) |
| AF + HF rhythm control | Amiodarone |
| ARNI in HF | Sacubitril/Valsartan — superior to ACEi (PARADIGM-HF) |
8. KEY IMAGES TO RECOGNIZE
- Electrical alternans on ECG → Cardiac tamponade
- Globular water-bottle heart on CXR → Large pericardial effusion
- Kerley B lines on CXR → Pulmonary venous HTN (e.g., in MS)
- Double density right heart border on CXR → LA enlargement (MS)
- Beaded/string-of-beads renal artery → Fibromuscular dysplasia
- Hockey-stick deformity on echo → Anterior mitral leaflet in MS
- Aschoff bodies on histology → Rheumatic carditis
Sources: Textbook of Family Medicine 9e; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22e; Fuster and Hurst's The Heart 15e; Braunwald's Heart Disease; 2024 ESC Hypertension Guidelines — Braunwald's Heart Disease, p. 1022; Goldman-Cecil, p. 717–868; Harrison's, p. 2094
This is a shared conversation. Sign in to Orris to start your own chat.