Low bp in 1 st trimester of pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypotension first trimester pregnancy
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Here is a comprehensive overview of low blood pressure (hypotension) in the first trimester of pregnancy:
Low Blood Pressure in the First Trimester of Pregnancy
Why It Happens: Physiological Basis
Low BP in the first trimester is largely normal and expected. Beginning as early as week 5–6 of gestation, a cascade of hormonal and vascular changes causes a significant drop in blood pressure:
-
Decrease in Systemic Vascular Resistance (SVR)
- Progesterone and prostaglandins cause vasodilation of peripheral blood vessels.
- Increased production of nitric oxide (an endothelium-derived relaxant factor) further lowers vascular tone.
- SVR drops progressively, reaching a nadir around 14–24 weeks (mid-second trimester), then gradually rises toward term.
-
Compensatory cardiac changes (which are not always sufficient to fully correct BP early on):
- Heart rate increases by ~20%
- Stroke volume increases by ~30%
- Cardiac output rises by 40–50%
-
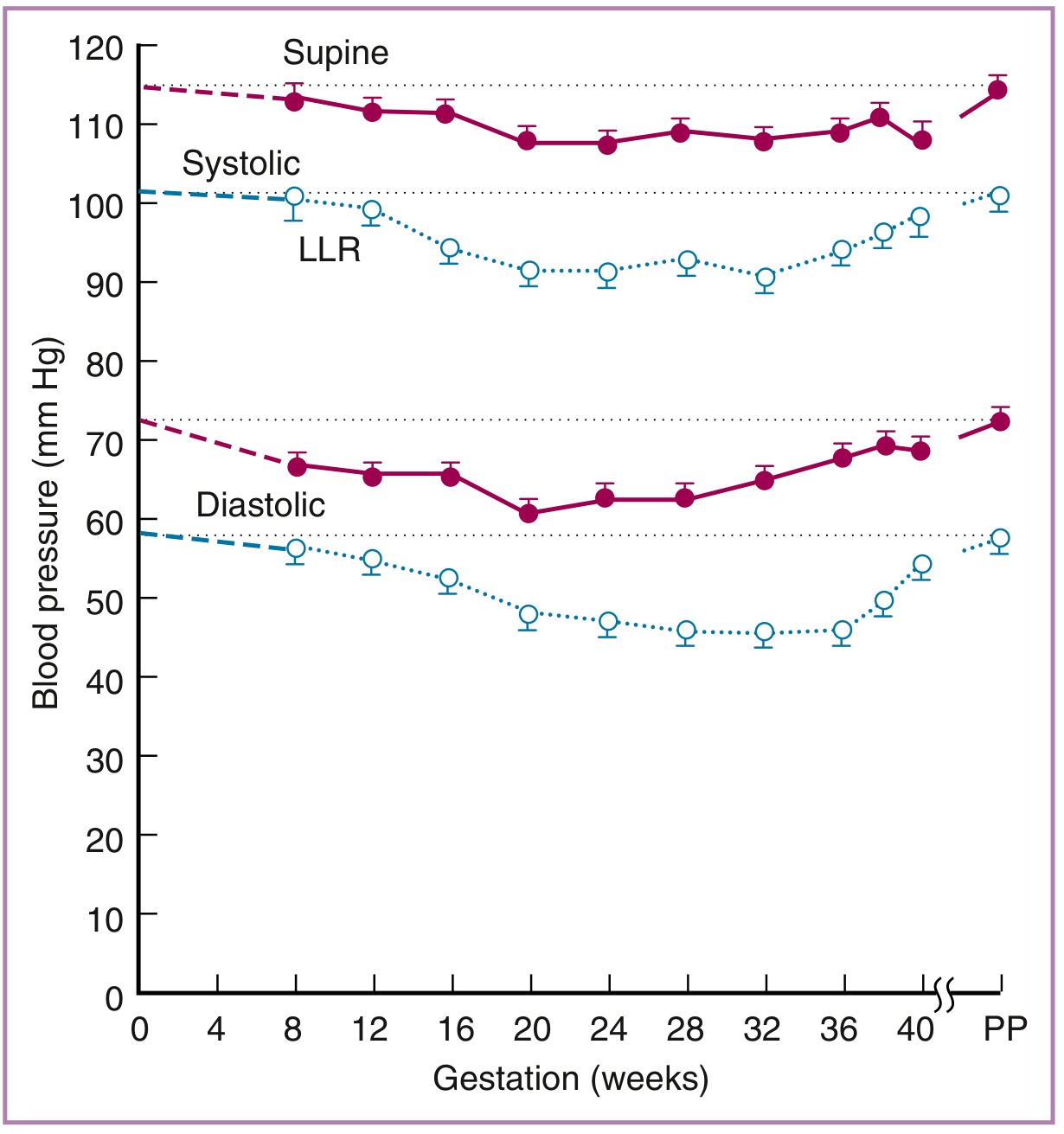
Net result: Blood pressure typically falls by 5–10 mmHg below pre-pregnancy baseline during the first and second trimesters, then returns to baseline by the third trimester.
This is illustrated in the graph below — both systolic and diastolic BP decline from conception, reaching their lowest point around 20–24 weeks, then recovering by term (PP = postpartum):
Symptoms of Low BP in Pregnancy
These may all be features of normal pregnancy but can be more pronounced when BP is low:
- Dizziness / light-headedness
- Fatigue
- Nausea and vomiting (also common with morning sickness)
- Palpitations
- Syncope or near-syncope (fainting)
- Pallor, sweating
Braunwald's Heart Disease notes: "Fatigue, dyspnea, light-headedness, and palpitations are symptoms that can be associated with normal pregnancy."
When Is It Pathological?
Low BP in the first trimester is not always benign. Red flags requiring investigation include:
| Concern | Possible Cause |
|---|---|
| Severe hypotension + vaginal bleeding | Ectopic pregnancy or threatened miscarriage |
| Hypotension + tachycardia + abdominal pain | Ruptured ectopic (surgical emergency) |
| Hypotension + vomiting + dehydration | Hyperemesis gravidarum |
| Pre-existing cardiac disease | Hemodynamic compromise |
| BP persistently < 90/60 mmHg with symptoms | Requires evaluation |
Causes of Hypotension in First Trimester
| Physiological (Normal) | Pathological |
|---|---|
| Progesterone-mediated vasodilation | Ectopic pregnancy with hemorrhage |
| Increased venous compliance | Dehydration from hyperemesis gravidarum |
| Low-resistance uteroplacental circulation | Sepsis |
| Dilutional effects of plasma volume expansion | Cardiac disease |
| Adrenal insufficiency (rare) |
Management
For physiological low BP (most first trimester cases):
- Reassurance — mild BP drop is normal and expected
- Adequate hydration — drink 8–10 glasses of water/day
- Dietary measures — small, frequent meals; increase salt intake slightly if not contraindicated
- Posture advice — rise slowly from lying/sitting (avoid orthostatic drops)
- Avoid prolonged standing — venous pooling worsens symptoms
- Compression stockings may help reduce venous pooling
- Rest in the left lateral position improves venous return
Pharmacological treatment is rarely needed in the first trimester for physiological hypotension.
For pathological causes:
- Ectopic pregnancy → urgent surgical/medical management
- Dehydration/hyperemesis → IV fluid resuscitation, antiemetics
- Cardiac causes → specialist cardiology + obstetric co-management
Key Points
- A drop of 5–10 mmHg in both systolic and diastolic BP is normal from the first trimester onward.
- It is primarily driven by progesterone-induced vasodilation and reduced SVR, starting as early as week 5.
- Symptoms like dizziness and fatigue are common but should prompt exclusion of ectopic pregnancy if accompanied by pain or bleeding.
- BP returns to pre-pregnancy baseline by the third trimester.
- The supine hypotension syndrome (aortocaval compression) is more relevant from >20 weeks, not the first trimester.
Sources: Braunwald's Heart Disease 12e, p. 1062 | Creasy & Resnik's Maternal-Fetal Medicine | Morgan & Mikhail's Clinical Anesthesiology 7e, p. 1575 | Tintinalli's Emergency Medicine
Is it harmful to the baby or mother
Finding Sources
Finding Sources
Searching PubMed
hypotension pregnancy fetal outcome
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Based on the textbook evidence gathered, here is a clear answer:
Is Low BP in the First Trimester Harmful to the Baby or Mother?
The short answer:
Mild, physiological low BP (the normal drop of 5–10 mmHg) is generally NOT harmful to either the mother or the baby. However, severe or pathological hypotension CAN be harmful, particularly to the baby.
Effect on the Baby
The key principle from the textbooks is:
"Uterine blood flow is not autoregulated but is directly proportional to the maternal mean arterial pressure." — Tintinalli's Emergency Medicine
"Maternal hypotension leads to a reduction in uterine blood flow and thus fetal hypoxia." — Barash's Clinical Anesthesia
This means:
| Type of Low BP | Effect on Baby |
|---|---|
| Mild physiological drop (5–10 mmHg, first trimester) | No significant harm — cardiac output simultaneously increases to compensate; uteroplacental circulation is maintained |
| Severe/acute hypotension | ↓ Uterine blood flow → Fetal hypoxia / asphyxia |
| Prolonged severe hypotension | Risk of fetal distress, growth restriction, fetal acidosis |
The uterine arteries are maximally dilated during pregnancy, meaning blood flow to the baby is almost entirely pressure-dependent — the baby cannot compensate on its own if the mother's BP drops severely. In the first trimester, the fetus is very small and metabolically less demanding, so mild drops are usually well tolerated.
Effect on the Mother
| Consequence | Detail |
|---|---|
| Dizziness / fainting | Most common risk — can lead to falls and injury |
| Falls | A fall in early pregnancy is a physical risk (though the uterus is still well-protected inside the pelvis in the first trimester) |
| Dehydration | Low BP from vomiting/dehydration creates a cycle that worsens both |
| Orthostatic hypotension | Sudden standing can trigger blackouts |
The mother's circulation has multiple compensatory mechanisms (increased heart rate, increased cardiac output), so the physiological BP drop is usually well-tolerated.
When It Becomes a Real Risk
Severe or symptomatic low BP in the first trimester is a warning sign that something else may be wrong:
- Ectopic pregnancy — a rupture causes sudden catastrophic hypotension that is life-threatening to the mother and fatal to the pregnancy
- Severe dehydration from hyperemesis gravidarum — can compromise both mother and baby
- Syncope (fainting) — risk of falls and injury to the mother
Important: "Volume must be adequately replaced before considering vasopressors, especially in pregnancy, because the uterine arteries are maximally dilated and blood flow is pressure dependent." — Tintinalli's Emergency Medicine
Summary
| Mild Physiological Low BP | Severe / Pathological Low BP | |
|---|---|---|
| Harmful to mother? | No (may cause dizziness/fainting) | Yes — syncope, shock |
| Harmful to baby? | No | Yes — fetal hypoxia, distress |
| Action needed? | Lifestyle measures, reassurance | Urgent medical evaluation |
The bottom line: The mild BP drop that naturally occurs in the first trimester is a normal pregnancy change and does not harm the baby or the mother. The body compensates by increasing cardiac output. The risk arises only if BP drops severely — particularly if there is an underlying cause like ectopic pregnancy or significant dehydration — in which case both mother and baby can be at risk.
Sources: Barash's Clinical Anesthesia 9e | Tintinalli's Emergency Medicine | Morgan & Mikhail's Clinical Anesthesiology 7e | Creasy & Resnik's Maternal-Fetal Medicine
Mother has always bp 90/60 mm of hg
Finding Sources
Finding Sources
Searching PubMed
chronic hypotension pregnancy maternal fetal outcomes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
This is a really important and specific scenario. Here is a thorough answer:
Mother Whose Baseline BP Is Always 90/60 mmHg — What Happens in Pregnancy?
First, Is 90/60 mmHg "Low"?
A BP of 90/60 mmHg is at the lower boundary of normal — often called constitutional (or chronic) hypotension. Many lean, young women naturally run at this BP their whole lives without any symptoms or organ damage. This is different from pathological hypotension.
What Happens During the First Trimester?
This is where it gets important. As explained previously, pregnancy itself causes BP to drop a further 5–10 mmHg (systolic) and 10–15 mmHg (diastolic) starting from week 7, reaching a nadir around 24–32 weeks.
"When measured in the left lateral recumbent position, both systolic and diastolic blood pressures decrease by 5 to 10 mmHg and 10 to 15 mmHg, respectively, below nonpregnant values." — Creasy & Resnik's Maternal-Fetal Medicine
So for this mother:
| Systolic | Diastolic | |
|---|---|---|
| Her baseline (before pregnancy) | 90 mmHg | 60 mmHg |
| Expected pregnancy drop | −5 to −10 mmHg | −10 to −15 mmHg |
| Possible BP in mid-pregnancy | ~80–85 mmHg | ~45–50 mmHg |
This means her BP could dip to quite low levels — lower than average pregnant women — especially in the second trimester.
Is This Dangerous?
For the Mother:
| Risk | Explanation |
|---|---|
| Dizziness & fainting (syncope) | More likely due to already low baseline — even mild positional changes can trigger blackouts |
| Falls | Risk of injury from fainting spells |
| Fatigue and weakness | More pronounced |
| Orthostatic hypotension | Rising quickly from bed or a chair can cause sudden BP drop → blackout |
| Nausea | Worsened by low BP combined with pregnancy nausea |
For the Baby:
Since uterine blood flow is directly pressure-dependent (not autoregulated):
"Uterine blood flow is not autoregulated but is directly proportional to the maternal mean arterial pressure." — Tintinalli's Emergency Medicine
"Maternal hypotension leads to a reduction in uterine blood flow and thus fetal hypoxia." — Barash's Clinical Anesthesia
However — in the first trimester specifically, the fetus is very small and has low oxygen demands, and the uteroplacental circulation is still being established. The risk to the baby from chronic mild hypotension in the first trimester is generally low, but if BP drops to very low levels (e.g., systolic < 80 mmHg), it could:
- Reduce placental perfusion
- Cause fetal growth restriction (more of a concern later in pregnancy)
- Worsen if she develops dehydration from morning sickness
What Should Be Done?
Since her BP was already 90/60 before pregnancy, there is no medication needed — treating it with drugs could make it worse. Management is lifestyle-based:
Practical Steps:
- Stay well-hydrated — aim for 8–10 glasses of water/day; dehydration quickly worsens BP
- Small, frequent meals — large meals divert blood to the gut and can worsen hypotension
- Increase salt intake slightly — salt retains fluid and helps maintain BP (unless she has a reason to restrict salt)
- Rise slowly — from lying → sitting → standing, pause at each step
- Avoid hot environments — hot showers, crowded places cause vasodilation and worsen hypotension
- Compression stockings — reduce venous pooling in the legs
- Sleep/rest on the left side — improves venous return to the heart
- Avoid prolonged standing
- Light regular exercise (walking, swimming) improves vascular tone if cleared by her doctor
Monitoring:
- Her BP should be checked at every antenatal visit
- If she develops symptoms (frequent fainting, inability to keep fluids down, persistent dizziness), she needs prompt medical review
- Watch for signs of ectopic pregnancy if there is pain or bleeding (which can also cause low BP)
Warning signs to go to hospital:
- Sudden severe drop in BP with pain or bleeding
- Fainting with no quick recovery
- Unable to take in fluids (risk of dehydration spiral)
The Reassuring News
For most women with constitutional 90/60 mmHg baseline, pregnancy progresses normally. The body has compensatory mechanisms (high cardiac output, increased heart rate), and many such women have healthy pregnancies without complications. The key is awareness, monitoring, and lifestyle adjustments — not medication.
Sources: Creasy & Resnik's Maternal-Fetal Medicine | Barash's Clinical Anesthesia 9e | Tintinalli's Emergency Medicine | Morgan & Mikhail's Clinical Anesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.