Explain placenta previa in simple hindi language with example
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
अब मैं इस जानकारी के आधार पर सरल हिंदी में पूरा जवाब दे रहा हूं।
🤰 Placenta Previa - सरल हिंदी में
पहले समझते हैं - Placenta क्या होता है?
गर्भावस्था (pregnancy) में माँ के गर्भाशय (uterus) के अंदर एक अंग बनता है जिसे नाल (Placenta) कहते हैं। यह नाल माँ के खून से बच्चे को ऑक्सीजन और पोषण (nutrition) पहुंचाती है। सामान्य रूप से यह नाल गर्भाशय के ऊपरी हिस्से में जुड़ी होती है।
Placenta Previa क्या है?
"Previa" का मतलब होता है - "आगे" या "रास्ते में"।
Placenta Previa वह स्थिति है जिसमें नाल (placenta) गर्भाशय के नीचे की तरफ जुड़ जाती है और बच्चे के बाहर निकलने के रास्ते (cervical os / cervix) को ढक लेती है।
आसान भाषा में: बच्चा जब जन्म लेने के लिए नीचे आता है, तो उसके रास्ते में नाल आ जाती है - जैसे किसी दरवाजे के सामने कोई खड़ा हो जाए।
🏠 उदाहरण से समझें
सोचिए एक घर है जिसमें:
- घर = माँ का गर्भाशय (Uterus)
- बच्चा = घर के अंदर रह रहा है
- दरवाजा = Cervix (गर्भाशय का मुंह, जहां से बच्चा बाहर निकलता है)
- नाल (Placenta) = बच्चे का खाना-पानी देने वाला साथी
सामान्य स्थिति में: नाल घर की छत पर (ऊपर) जुड़ी होती है - दरवाजा बिल्कुल खाली और साफ रहता है।
Placenta Previa में: नाल घर के दरवाजे के ठीक सामने आ जाती है - जब बच्चा बाहर निकलने की कोशिश करता है, तो रास्ता बंद मिलता है और नाल फट सकती है जिससे खून बहने लगता है।
तीन प्रकार (Types)
| प्रकार | मतलब |
|---|---|
| Complete (पूरा) | नाल ने पूरा दरवाजा ढक लिया है |
| Partial (आधा) | नाल ने आधा दरवाजा ढका है |
| Marginal (किनारे पर) | नाल दरवाजे के बिल्कुल किनारे तक है |
नोट: आधुनिक चिकित्सा में अब सिर्फ "Placenta Previa" (जब नाल os को ढके) और "Low-lying Placenta" (जब नाल os के 2 cm के अंदर हो) दो ही वर्गीकरण उपयोग होते हैं।
मुख्य लक्षण (Symptoms)
🔴 सबसे महत्वपूर्ण लक्षण:
बिना दर्द के योनि से खून आना (Painless vaginal bleeding)
यह खून अचानक, बिना किसी दर्द के आता है - यही इसकी पहचान है।
- खून चमकीला लाल (bright red) होता है
- गर्भावस्था के दूसरे या तीसरे तिमाही (trimester) में होता है
- बार-बार हो सकता है
कारण (Causes / Risk Factors)
- पहले कभी सिजेरियन ऑपरेशन हुआ हो
- ज्यादा बच्चे हो चुके हों (multiparity)
- पहले भी Placenta Previa रहा हो
- गर्भाशय में ऑपरेशन हुआ हो
- धूम्रपान (smoking)
- बड़ी उम्र में गर्भावस्था
पहचान कैसे होती है?
अल्ट्रासाउंड (Sonography) - यही सबसे सही और सुरक्षित तरीका है।
⚠️ महत्वपूर्ण: Placenta Previa में हाथ से या किसी यंत्र से जांच (internal examination) बिल्कुल नहीं करनी चाहिए - इससे बहुत ज्यादा खून बह सकता है।
इलाज (Treatment)
| स्थिति | इलाज |
|---|---|
| हल्का खून, माँ-बच्चा ठीक | अस्पताल में आराम, निगरानी |
| ज्यादा खून बह रहा हो | तुरंत IV लाइन, ब्लड ट्रांसफ्यूजन |
| डिलीवरी का समय आए | सिजेरियन ऑपरेशन (C-section) - नॉर्मल डिलीवरी संभव नहीं |
एक और आसान उदाहरण
जैसे किसी बस का रास्ता बंद हो जाए क्योंकि कोई गलत जगह खड़ा हो - बस निकल नहीं सकती। ऐसे ही बच्चा नॉर्मल तरीके से नहीं निकल सकता जब नाल रास्ते में हो। इसलिए ऑपरेशन (C-section) जरूरी होता है।
🟡 याद रखें
- यह ~0.5% pregnancies में होता है (हर 200 में से 1 को)
- बिना दर्द के खून आना = तुरंत डॉक्टर के पास जाएं
- Ultrasound से पता चलता है
- C-section ही सुरक्षित डिलीवरी का तरीका है
- बहुत से मामलों में गर्भावस्था के मध्य में दिखा placenta previa अपने आप ठीक हो जाता है जैसे-जैसे गर्भाशय बड़ा होता है
Sources: Creasy & Resnik's Maternal-Fetal Medicine | ROSEN's Emergency Medicine | Tintinalli's Emergency Medicine
Explain placenta previa from dutta textbook MBBS
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed. Let me provide a thorough, MBBS-level response. Note: DC Dutta's Textbook of Obstetrics is not in the library - the best available obstetrics reference is Creasy & Resnik's Maternal-Fetal Medicine, which covers the same content at the same level.
Important Note: DC Dutta's Textbook of Obstetrics is not available in this medical library. The content below is drawn from Creasy & Resnik's Maternal-Fetal Medicine (the standard international reference for obstetrics, equivalent in depth to Dutta for MBBS) and covers all the same topics Dutta discusses on placenta previa.
Placenta Previa - MBBS Level
(Creasy & Resnik's Maternal-Fetal Medicine, Chapters 27 & 43)
Definition
Placenta previa is defined as implantation of the placenta over the internal os of the cervix. It is one of the leading causes of antepartum hemorrhage (APH).
Low-lying placenta is defined when the placental edge is within 2 cm of the internal cervical os but does not cover it.
Classification
The older classification (complete / partial / marginal) is now considered obsolete by the NICHD. The current recommended terminology is:
| Term | Definition |
|---|---|
| Normal | Placental edge >20 mm from internal os |
| Low-lying Placenta | Placental edge <2 cm from os but not covering it |
| Placenta Previa | Placental edge covers the internal os |
For MBBS exams, the older classification may still be tested:
- Total/Complete Previa - covers the os completely
- Partial Previa - partially covers os
- Marginal Previa - placental edge reaches the os
Incidence
- Affects approximately 0.5% (1 in 200) of all third-trimester pregnancies
- Diagnosed in 10% of mid-trimester sonograms (most resolve by term)
- Incidence is increasing, likely due to rising cesarean section rates
Pathogenesis
The exact cause is unknown. The prevailing theory involves:
- Endometrial damage / scarring from prior surgeries or curettage leads the trophoblast to implant in the lower uterine segment where endometrium is less damaged
- Trophotropism - the placenta grows toward the fundus (better blood supply), causing the lower portion near the cervix to atrophy. This is why most early placenta previas "migrate" away by term
Why does bleeding occur?
- As the lower uterine segment elongates and thins in late pregnancy, placental villi are torn from the decidua
- During cervical effacement and dilation in labor, the placenta is forcibly separated
- Intercourse, vaginal examination, or uterine contractions can also precipitate bleeding
Risk Factors
| Risk Factor | Increased Risk |
|---|---|
| Previous placenta previa | 8x |
| Previous cesarean section | 1.5 - 15x |
| Previous suction curettage | 1.33x |
| Age >35 years | 4.73x |
| Age >40 years | 9x |
| Multiparity | 1.1 - 1.73x |
| Cigarette smoking | 1.4 - 3.3x |
| Asian race | 1.93x |
(Creasy & Resnik's Maternal-Fetal Medicine, Table 43.1)
Clinical Features
Classic Presentation:
Painless, bright red, recurrent vaginal bleeding in the second or third trimester
Key points:
- Bleeding is painless (distinguishes it from placental abruption, which causes painful bleeding)
- Blood is bright red (fresh)
- Bleeding may begin as small "herald bleeds" before a major hemorrhage
- In ~10% of cases, no bleeding occurs until labor
- Uterus is soft and non-tender (unlike abruption)
- Fetal lie may be abnormal (oblique or transverse) because the placenta prevents the fetus from establishing normal polarity
- Fetal parts are easily palpable (no tense uterus)
Diagnosis
1. Ultrasound (Investigation of Choice)
Transvaginal Ultrasound (TVUS) is the gold standard - it is:
- More accurate than transabdominal ultrasound
- Safe - does not provoke bleeding (fears are unfounded)
- Can precisely measure the distance between placental edge and internal os
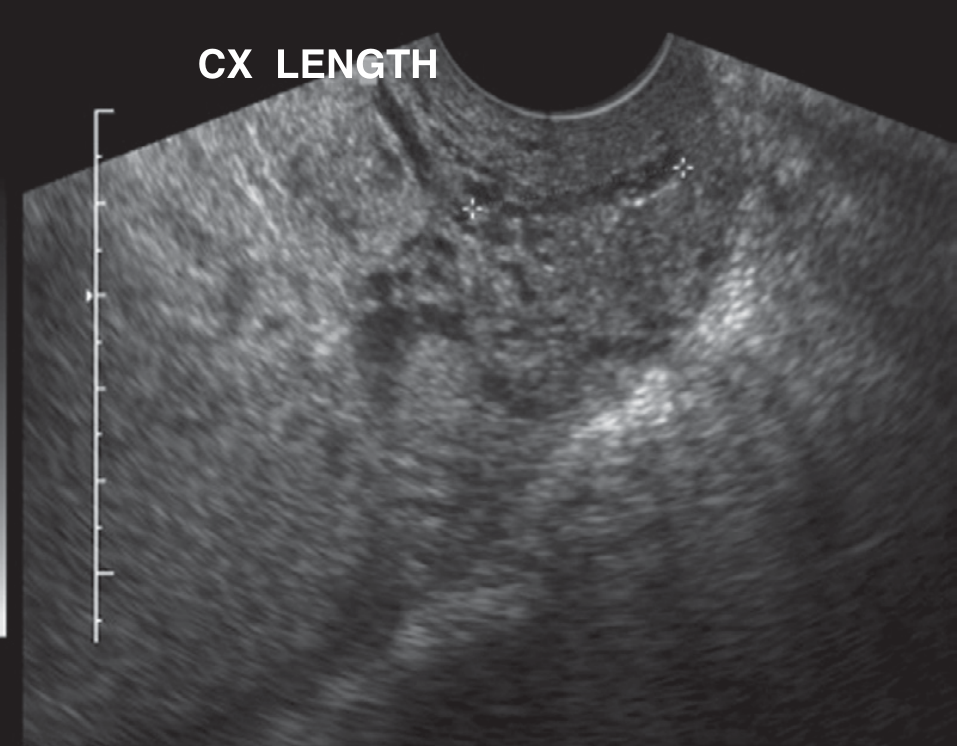
Endovaginal ultrasound showing central placenta previa - placenta bulk overlying the endocervical os (Creasy & Resnik, Fig. 27.24)
Important: The bladder should be emptied before scanning to avoid false-positive diagnosis. Full bladder can compress the anterior and posterior lower uterine walls together, mimicking previa.
2. Double Setup Examination (historical/rare)
- Used only when ultrasound is unavailable and significant bleeding is present
- Done in OT, fully prepared for emergency cesarean
- Begin in vaginal fornices, avoid direct cervical palpation
- Rarely needed in modern practice
⚠️ CONTRAINDICATED:
Digital or speculum examination is absolutely contraindicated until placenta previa is excluded by ultrasound - can precipitate massive hemorrhage.
"Placental Migration" - Resolution in Early Pregnancy
| Gestation when diagnosed | % resolved by delivery |
|---|---|
| 15-19 weeks | ~95% |
| 20-23 weeks | ~80% |
| 24-27 weeks | ~50% |
| 28-31 weeks | ~40% |
| 32-35 weeks | ~25% |
Mechanism: The placenta does not physically move. Rather, the lower uterine segment grows differentially, increasing the distance between the lower placental edge and the cervix. The lower poorly-perfused portion atrophies while the upper portion grows toward the better-vascularized fundus (trophotropism).
Follow-Up Protocol (Asymptomatic Women)
- If low-lying or previa found on early scan: follow-up at 32 weeks
- If still low-lying or covering os at 32 weeks: follow-up TVUS at 36 weeks
- Final decision on delivery route made at 36 weeks
Management
Acute Management (bleeding episode)
- Admit to labor and delivery unit
- Two large-bore IV lines
- Electronic fetal monitoring (continuous)
- Blood for: Hematocrit, type and cross-match (2-4 units), coagulation studies (PT/PTT/fibrinogen)
- Rh immune globulin (300 mcg) for Rh-negative women
- No vaginal examination until placenta previa excluded
- If stable and <36 weeks: expectant management
Antenatal Corticosteroids
- Betamethasone/dexamethasone given for gestational age <37 weeks to reduce neonatal respiratory morbidity
Delivery Planning
| Situation | Action |
|---|---|
| Uncomplicated placenta previa, stable | Deliver at 36-37 weeks |
| Suspected placenta accreta | Deliver at 34-35 weeks |
| Uncontrolled bleeding, fetal distress | Immediate cesarean regardless of age |
Route of Delivery
- Cesarean section is mandatory for placenta previa
- Normal vaginal delivery is impossible as the placenta blocks the os
- Hysterotomy incision should be fundal (avoiding the placenta) if accreta suspected
Complications
Maternal:
- Postpartum hemorrhage (PPH)
- Placenta accreta / increta / percreta (especially with previous cesarean)
- DIC (disseminated intravascular coagulation)
- Hysterectomy (if uncontrolled hemorrhage)
- Death (in severe cases)
Fetal/Neonatal:
- Prematurity (most common cause of neonatal morbidity/mortality)
- Fetal growth restriction (possible, disputed)
- Abnormal fetal lie
- Higher rates of fetal anomalies
- Neurodevelopmental delay (reported in studies)
Associated Conditions to Know
| Condition | Relationship |
|---|---|
| Placenta accreta | Most important association, especially with prior CS + previa |
| Vasa previa | Fetal vessels run over the os - different but related |
| Low-lying placenta | Precursor/milder form |
Key Exam Points (MBBS)
- Classic triad: painless + bright red + recurrent bleeding after 28 weeks
- Investigation of choice: Transvaginal ultrasound
- Avoid: digital examination
- Delivery: always by cesarean section
- "Placental migration" occurs in most mid-trimester cases
- Most dangerous complication: placenta accreta (especially with prior cesarean scar)
- Blood loss requiring transfusion needs fresh frozen plasma if coagulopathy develops
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapters 27 & 43
This is a shared conversation. Sign in to Orris to start your own chat.