Megaloblastic anemia for MBBS final year exam 10 mark question in medicine
Megaloblastic Anemia - 10 Mark Question (MBBS Final Year Medicine)
Definition
- Goldman-Cecil Medicine, p. 1015
Causes / Etiology
Vitamin B12 Deficiency
| Category | Examples |
|---|---|
| Lack of intrinsic factor (IF) | Pernicious anemia (autoimmune type A gastritis), gastrectomy, congenital IF defect |
| Malabsorption (terminal ileum) | Ileal resection, Crohn disease, ileal conduit, Imerslund-Gräseck syndrome |
| Usurpation | Bacterial overgrowth (blind loop syndrome), Diphyllobothrium latum (fish tapeworm), Giardia |
| Dietary | Vegans, lacto-ovo vegetarians, poverty, breast-fed infants of deficient mothers |
| Drugs | Metformin, proton pump inhibitors, nitrous oxide, methotrexate |
| Inborn errors | Transcobalamin deficiency, combined methylmalonic acidemia (CblC) |
Folic Acid Deficiency
| Category | Examples |
|---|---|
| Decreased intake | Poor diet, alcoholism, anorexia nervosa, infancy |
| Malabsorption | Celiac disease, tropical sprue, Crohn disease |
| Increased requirement | Pregnancy, hemolytic anemias, leukemia, proliferative skin diseases |
| Increased loss | Hemodialysis |
| Drugs (impaired utilization) | Methotrexate, phenytoin (anticonvulsants), oral contraceptives, trimethoprim |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 14.5
Pathogenesis / Biochemical Mechanism
Role of Vitamin B12
- Methionine synthase - converts homocysteine + methyl-THF → methionine + THF
- B12 deficiency blocks this → methyl-folate trap: methyl-THF accumulates and cannot be converted to the active THF form → secondary folate deficiency
- Serum homocysteine rises
- L-methylmalonyl-CoA mutase - converts methylmalonyl-CoA → succinyl-CoA (adenosyl-B12 dependent)
- Blockade → methylmalonic acid (MMA) accumulates in blood and urine
- MMA elevation is specific to B12 deficiency (NOT seen in folate deficiency)
- MMA is incorporated into abnormal myelin - explains the neurological manifestations
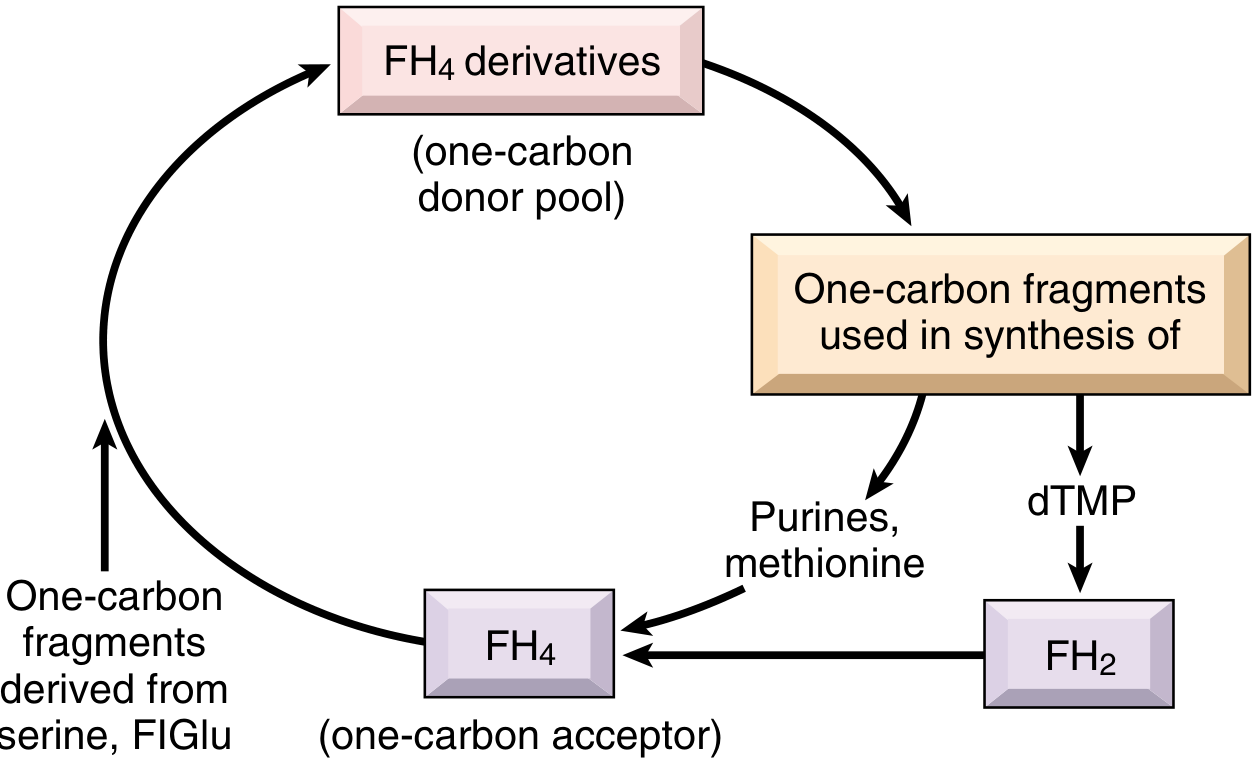
Role of Folate
- THF derivatives are needed for purine synthesis, dTMP synthesis, and methionine regeneration
- The 5,10-methylene-THF form participates in thymidylate synthase reaction (dUMP → dTMP)
- Folate deficiency → insufficient thymidine → uracil incorporated into DNA → DNA strand breaks, prolonged cell cycle, chromosomal damage, maturation arrest, apoptosis
- Goldman-Cecil Medicine, p. 1164-1167
Morphology / Pathology
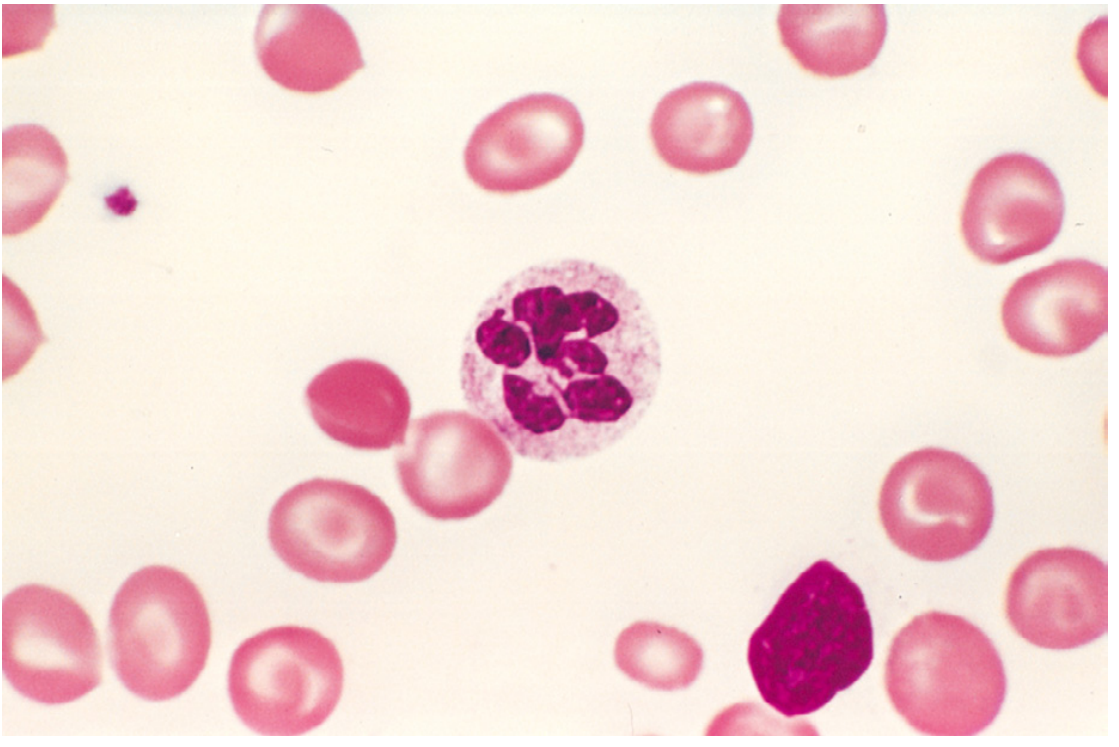
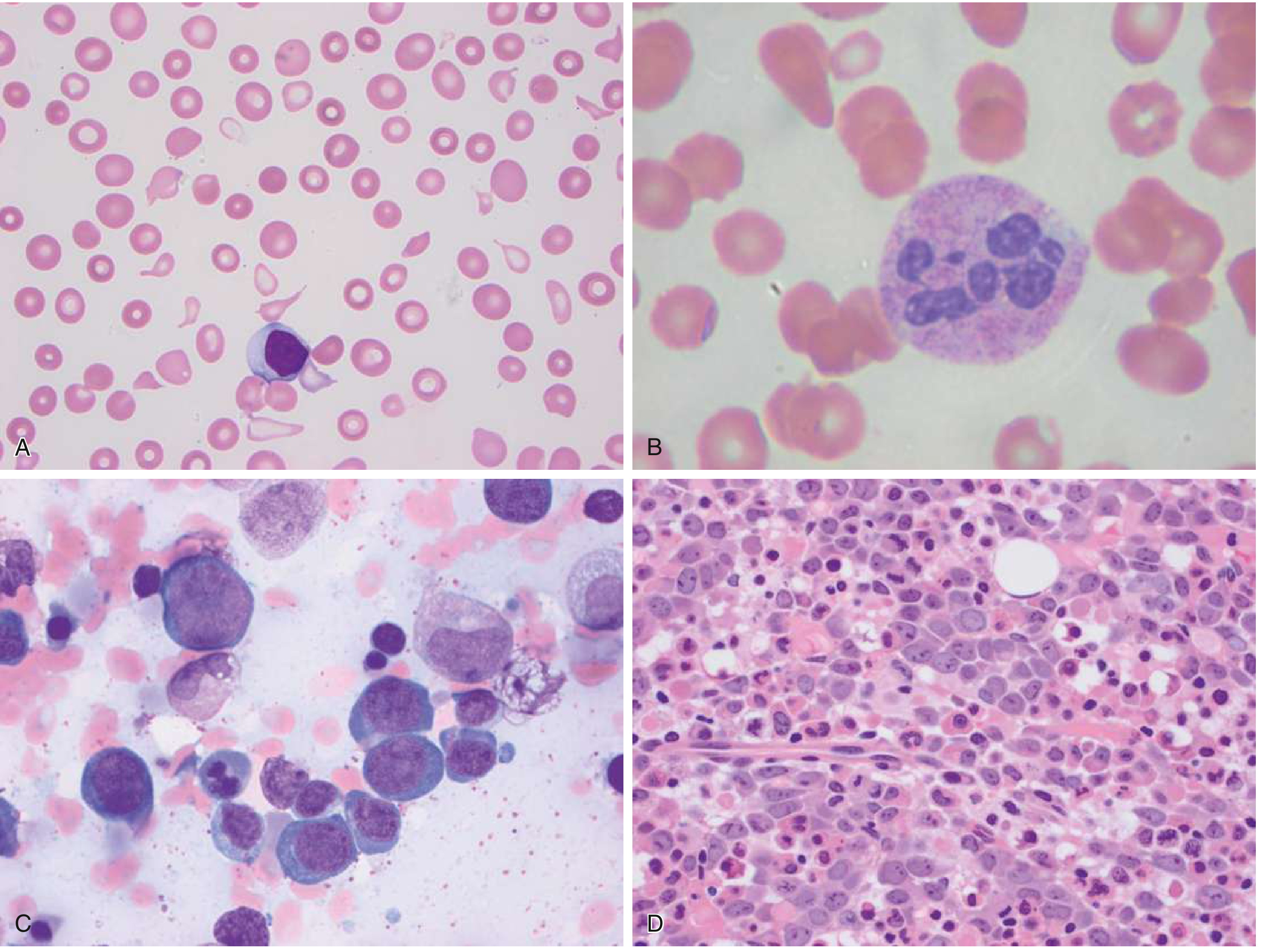
Peripheral Blood Smear
- Macro-ovalocytes (oval macrocytes) - highly characteristic; MCV often >110 fL
- Macrocytes appear "hyperchromic" (no central pallor) but MCHC is not elevated
- Marked anisocytosis and poikilocytosis
- Hypersegmented neutrophils (5 or more lobes; >5% with 5 lobes or any with 6+ lobes) - pathognomonic
- Low reticulocyte count
- Thrombocytopenia and leukopenia in severe cases (pancytopenia)
Bone Marrow
- Hypercellular marrow (paradox of anemia with hypercellular marrow = ineffective erythropoiesis)
- Megaloblasts at all stages: large cells with finely dispersed, "open" chromatin (lacy chromatin) while cytoplasm is hemoglobinized = nuclear-cytoplasmic asynchrony
- Giant metamyelocytes and band forms (dysmaturation of granulocyte precursors)
- Abnormally large megakaryocytes with bizarre multilobate nuclei
- High iron stores (ineffective erythropoiesis)
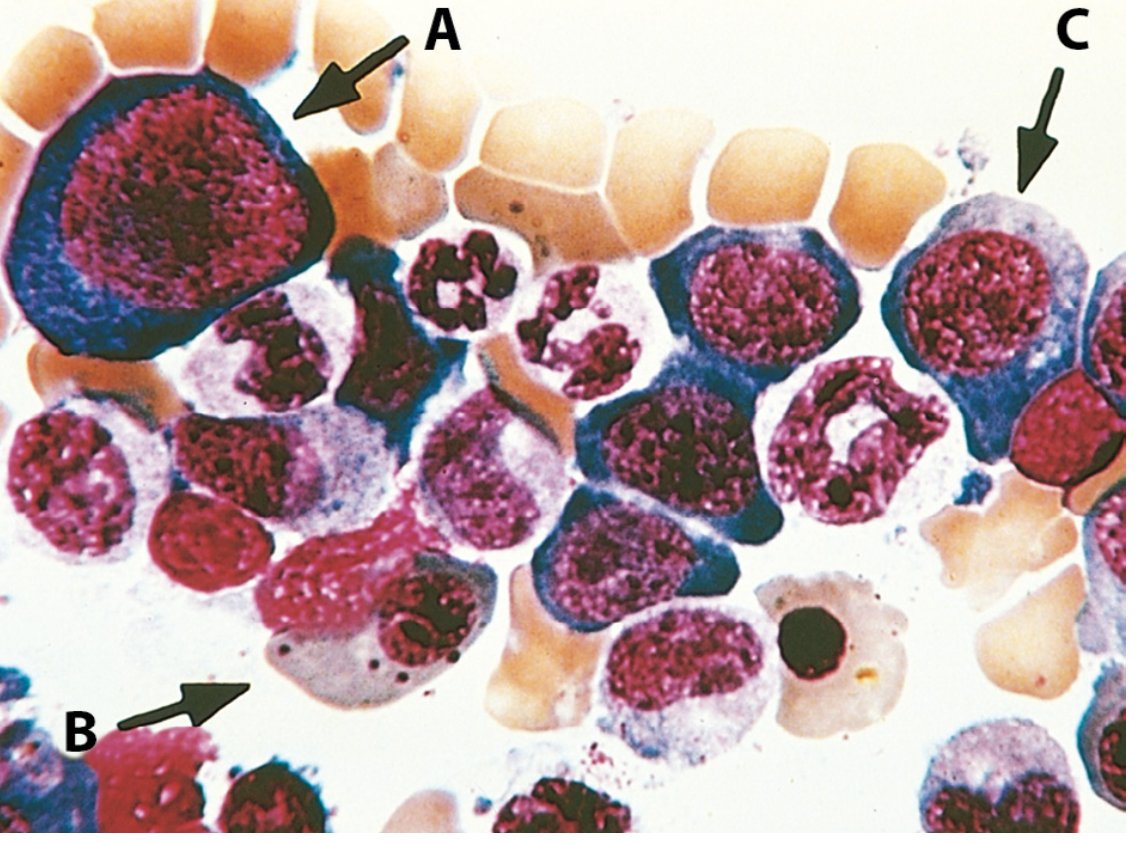
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 608-610
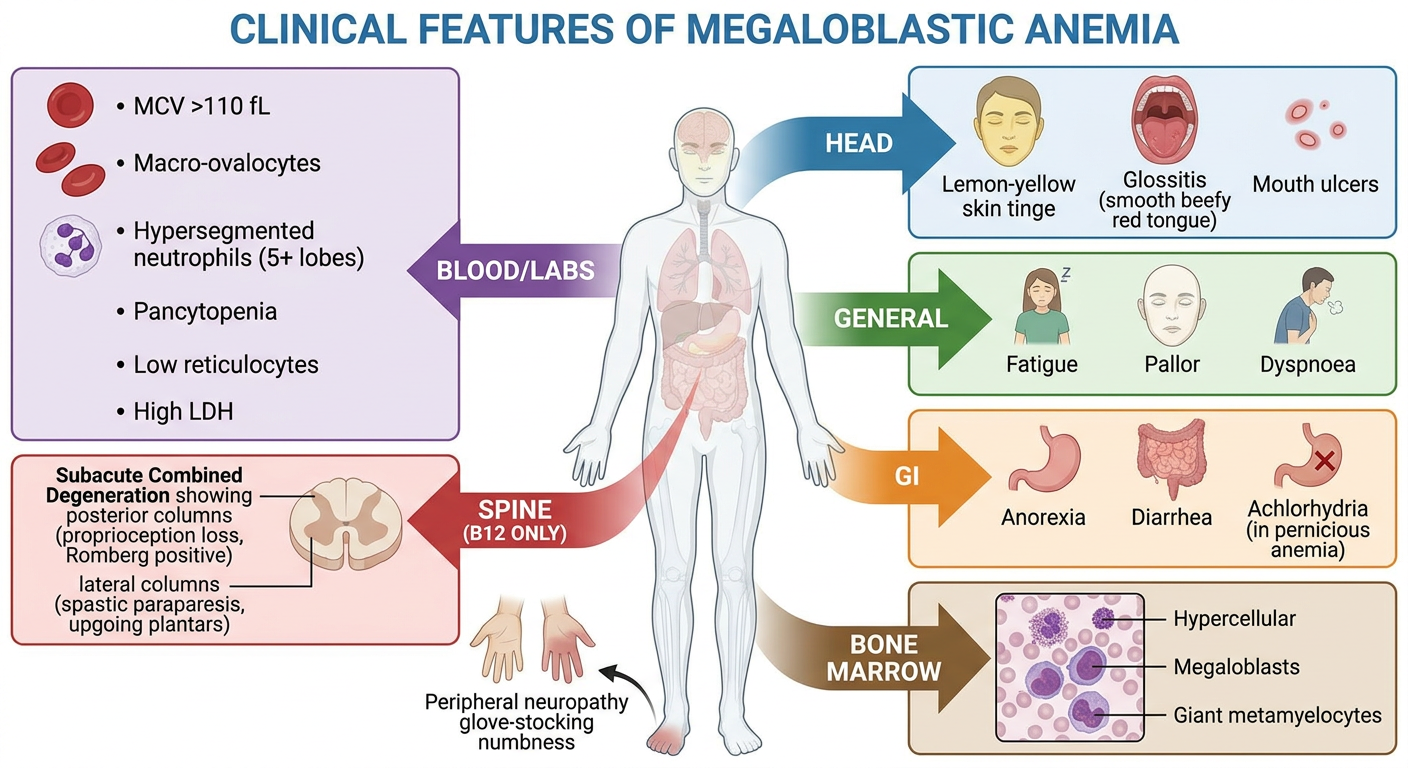
Clinical Features
General Anemia Features
- Fatigue, pallor, dyspnea on exertion, palpitations
- Lemon-yellow tinge (mild jaundice) - due to ineffective erythropoiesis and hemolysis
Features Specific to Vitamin B12 Deficiency (Pernicious Anemia)
- Glossitis (Hunter's glossitis) - smooth, beefy-red, painful tongue (atrophy of papillae)
- Anorexia, weight loss, diarrhea
- Achlorhydria (atrophic gastritis type A in pernicious anemia)
- Demyelination of posterior columns (dorsal columns) → loss of vibration sense, proprioception, positive Romberg's sign
- Demyelination of lateral corticospinal tracts → spastic paraparesis, hyperreflexia, extensor plantar response
- Peripheral neuropathy (glove-and-stocking sensory loss, decreased reflexes)
- Psychiatric symptoms ("megaloblastic madness"): memory loss, depression, psychosis
Features Specific to Folate Deficiency
- Anemia without neurological signs
- Glossitis
- Associated with alcoholism, pregnancy
Investigations / Diagnosis
Blood Tests
| Test | Finding |
|---|---|
| CBC | Macrocytic anemia (MCV >100 fL), pancytopenia in severe cases |
| Peripheral blood smear | Macro-ovalocytes, hypersegmented neutrophils |
| Reticulocyte count | Low (hypoproliferative) |
| Serum Vitamin B12 | Low (<200 pg/mL in deficiency) |
| Serum Folate | Low in folate deficiency |
| RBC folate | More reliable indicator of chronic folate status |
| Serum homocysteine | Elevated in BOTH B12 and folate deficiency |
| Serum methylmalonic acid (MMA) | Elevated ONLY in B12 deficiency (differentiates) |
| LDH | Markedly elevated (intravascular destruction) |
| Indirect bilirubin | Mildly elevated (hemolysis component) |
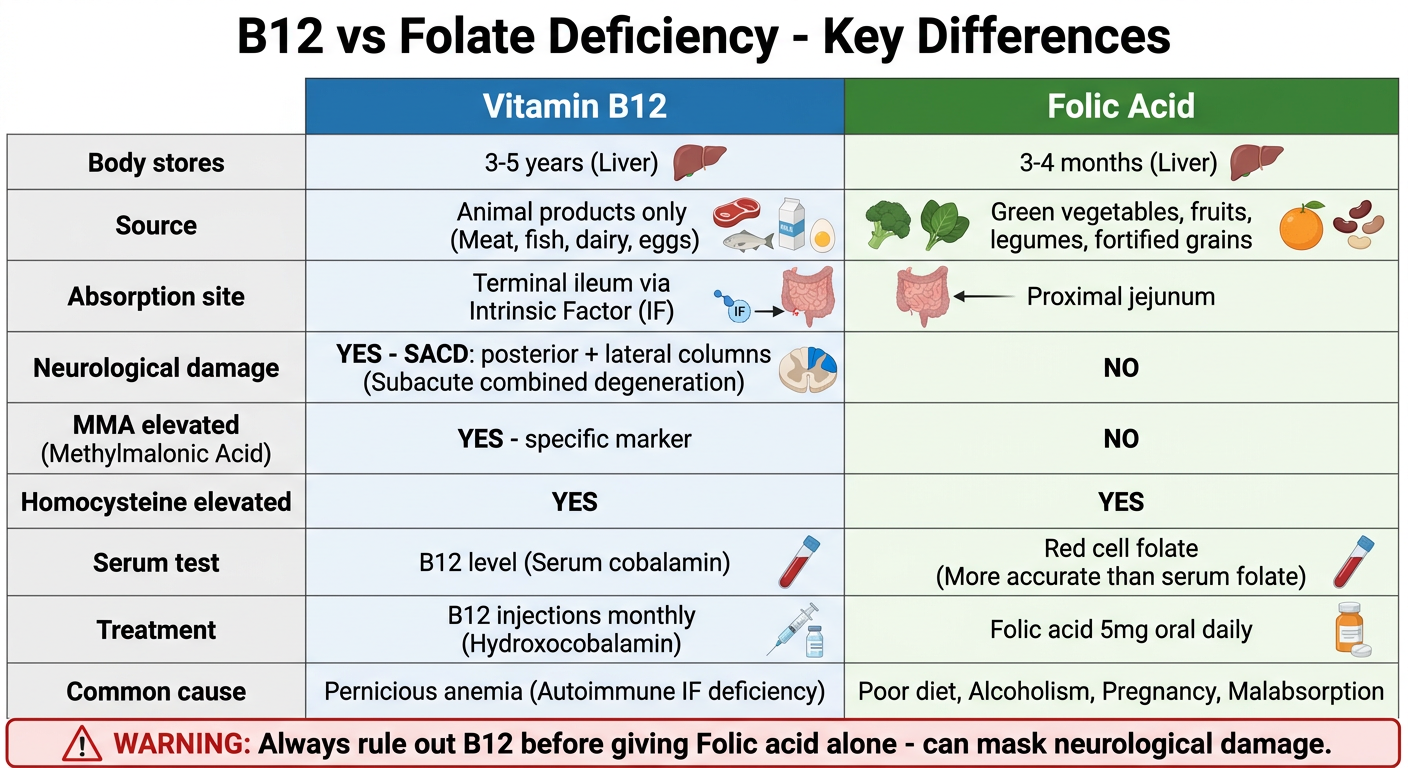
Differentiating B12 from Folate Deficiency
| Feature | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Serum MMA | Elevated | Normal |
| Serum homocysteine | Elevated | Elevated |
| Neurological symptoms | Present (SACD) | Absent |
| Serum IF antibodies | Present in pernicious anemia | Absent |
| Schilling test | Abnormal (corrected by IF) | Normal |
Bone Marrow Biopsy
- Hypercellular with megaloblastic changes (rarely needed for diagnosis)
Schilling Test (historical)
- Oral radiolabeled B12 given, then IM B12 given to saturate binding proteins
- Measure urinary excretion of radiolabeled B12
- Stage I (B12 alone): Low excretion → confirms malabsorption
- Stage II (B12 + IF): Corrects if pernicious anemia; does not correct if ileal disease
Anti-Intrinsic Factor Antibodies
- Highly specific for pernicious anemia (>95% specificity)
- Type I (blocking antibodies): block IF-B12 complex formation
- Type II (binding antibodies): bind to IF-B12 complex
Anti-Parietal Cell Antibodies
- Present in ~90% of pernicious anemia - but less specific (also present in atrophic gastritis)
Treatment
Vitamin B12 Deficiency
- Hydroxocobalamin 1000 mcg IM daily for 7 days, then weekly for 4 weeks, then monthly for life (if pernicious anemia or irreversible cause)
- Or cyanocobalamin 1000 mcg IM - same schedule
- Cyanocobalamin 1000-2000 mcg/day orally - effective even in pernicious anemia because 1% is absorbed by passive diffusion independent of IF
- Reticulocyte crisis begins within 3-5 days, peaks by day 5-10
- Neurological improvement may occur over weeks to months but is incomplete if long-standing
Folic Acid Deficiency
- Folic acid 5 mg/day orally for 4 months (or until the underlying cause is corrected)
- Prophylaxis in pregnancy: 400-800 mcg/day (reduces neural tube defects)
- Treat the underlying cause (alcohol cessation, treat malabsorption, etc.)
Key Differences - B12 vs Folate Deficiency at a Glance
| Feature | B12 | Folate |
|---|---|---|
| Stores in body | 2-5 mg (lasts 3-5 years) | 5-20 mg (lasts 3-4 months) |
| Source | Animal products only | Green vegetables, fruits, liver |
| Neurological | SACD (yes) | No |
| MMA elevation | Yes (specific) | No |
| Absorption site | Terminal ileum (requires IF) | Proximal jejunum |
| Treatment | B12 injections | Oral folic acid |
Complications
- Pancytopenia with severe infection risk and bleeding
- Subacute combined degeneration (B12 only) - if untreated, irreversible paraplegia
- Gastric carcinoma - increased risk in pernicious anemia (atrophic gastritis)
- Neural tube defects in fetus of folate-deficient mothers
- Thrombosis from hyperhomocysteinemia (both B12 and folate deficiency)
- Reversible infertility
Summary Mnemonics
- SACD = B12 only (Subacute Combined Degeneration)
- MMA = B12 marker (Methylmalonic Acid elevated only in B12 deficiency)
- Homocysteine rises in BOTH
- "Treat folate - always rule out B12 first"
Same content but give me diagram and photos so i can remember easily
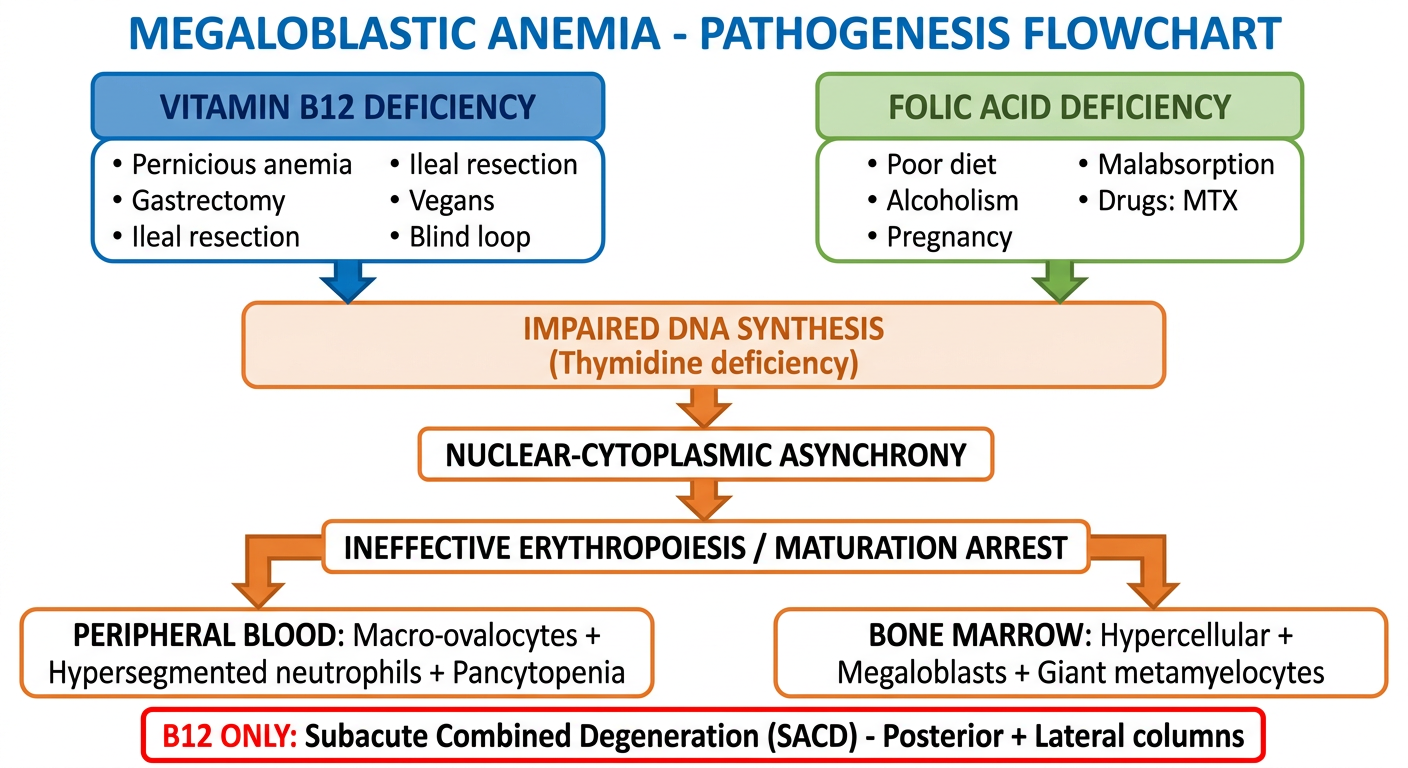
Medical education diagram for MBBS students: Megaloblastic Anemia - Pathogenesis Flowchart. Show two parallel pathways: Left pathway labeled "Vitamin B12 Deficiency" with causes listed (Pernicious anemia, Gastrectomy, Ileal resection, Vegans, Blind loop). Right pathway labeled "Folic Acid Deficiency" with causes (Poor diet, Alcoholism, Pregnancy, Malabsorption, Drugs: MTX). Both arrows converge to a central box: "Impaired DNA Synthesis (Thymidine deficiency)". Below that flows to: "Nuclear-Cytoplasmic Asynchrony" then to "Ineffective Erythropoiesis / Maturation Arrest" then branches into: left = "Peripheral Blood: Macro-ovalocytes + Hypersegmented neutrophils + Pancytopenia" and right = "Bone Marrow: Hypercellular + Megaloblasts + Giant metamyelocytes". At the bottom a red warning box: "B12 ONLY: Subacute Combined Degeneration (SACD) - Posterior + Lateral columns". Clean white background, color coded blue for B12, green for folate, orange for shared pathway.
Medical comparison table diagram for MBBS exam: "B12 vs Folate Deficiency - Key Differences". Two-column visual comparison with clear headers: left column blue "Vitamin B12" and right column green "Folic Acid". Compare these rows: Body stores (3-5 years vs 3-4 months), Source (Animal products only vs Green vegetables, fruits), Absorption site (Terminal ileum via Intrinsic Factor vs Proximal jejunum), Neurological damage (YES - SACD: posterior + lateral columns vs NO), MMA elevated (YES - specific marker vs NO), Homocysteine elevated (YES vs YES), Serum test (B12 level vs Red cell folate), Treatment (B12 injections monthly vs Folic acid 5mg oral daily), Common cause (Pernicious anemia vs Poor diet/Alcoholism/Pregnancy). Bottom row in red bold: WARNING: Always rule out B12 before giving Folic acid alone - can mask neurological damage. Clean professional medical textbook style, white background.
Medical diagram for MBBS students: Clinical Features of Megaloblastic Anemia - Mind Map / Body Diagram. Central figure of a human body with labeled arrows pointing to affected systems. Include: HEAD: Lemon-yellow skin tinge, glossitis (smooth beefy red tongue), mouth ulcers. BLOOD/LABS panel: MCV >110 fL, Macro-ovalocytes, Hypersegmented neutrophils (5+ lobes), Pancytopenia, Low reticulocytes, High LDH. SPINE (B12 ONLY - highlighted in red): Subacute Combined Degeneration showing posterior columns (proprioception loss, Romberg positive) and lateral columns (spastic paraparesis, upgoing plantars), peripheral neuropathy glove-stocking numbness. GENERAL: Fatigue, pallor, dyspnoea. GI: Anorexia, diarrhea, achlorhydria (in pernicious anemia). BONE MARROW panel: Hypercellular, megaloblasts, giant metamyelocytes. Color coded, clean white background, professional medical illustration style suitable for exam notes.
Medical diagram for MBBS exam: Treatment Protocol for Megaloblastic Anemia. Two treatment boxes side by side. Left box (blue, "VITAMIN B12 DEFICIENCY"): Step 1 - ALWAYS rule out B12 before folate. Step 2 - Hydroxocobalamin 1000mcg IM daily x 7 days, then weekly x 4 weeks, then monthly for life (pernicious anemia). Or cyanocobalamin same schedule. Or high-dose oral 1-2mg daily (dietary deficiency only). Expected response: Reticulocyte crisis Day 3-5, Peak Day 7-10. Right box (green, "FOLIC ACID DEFICIENCY"): Folic acid 5mg oral daily x 4 months. Prophylaxis in pregnancy: 400-800mcg daily (prevents neural tube defects). Treat underlying cause (alcohol, malabsorption). Below both boxes - shared monitoring box: "Reticulocyte count rise confirms diagnosis. Check B12 AND folate in all macrocytic anemias." Large red warning banner at top: "DANGER: Do NOT give Folic Acid alone in B12 deficiency - will correct anemia but WORSEN neurological damage!" Clean white background, professional medical style.
🔬 Megaloblastic Anemia - Visual Study Guide (MBBS Final Year)
1. PATHOGENESIS FLOWCHART
2. HOW B12 IS ABSORBED (Textbook Diagram - Robbins)
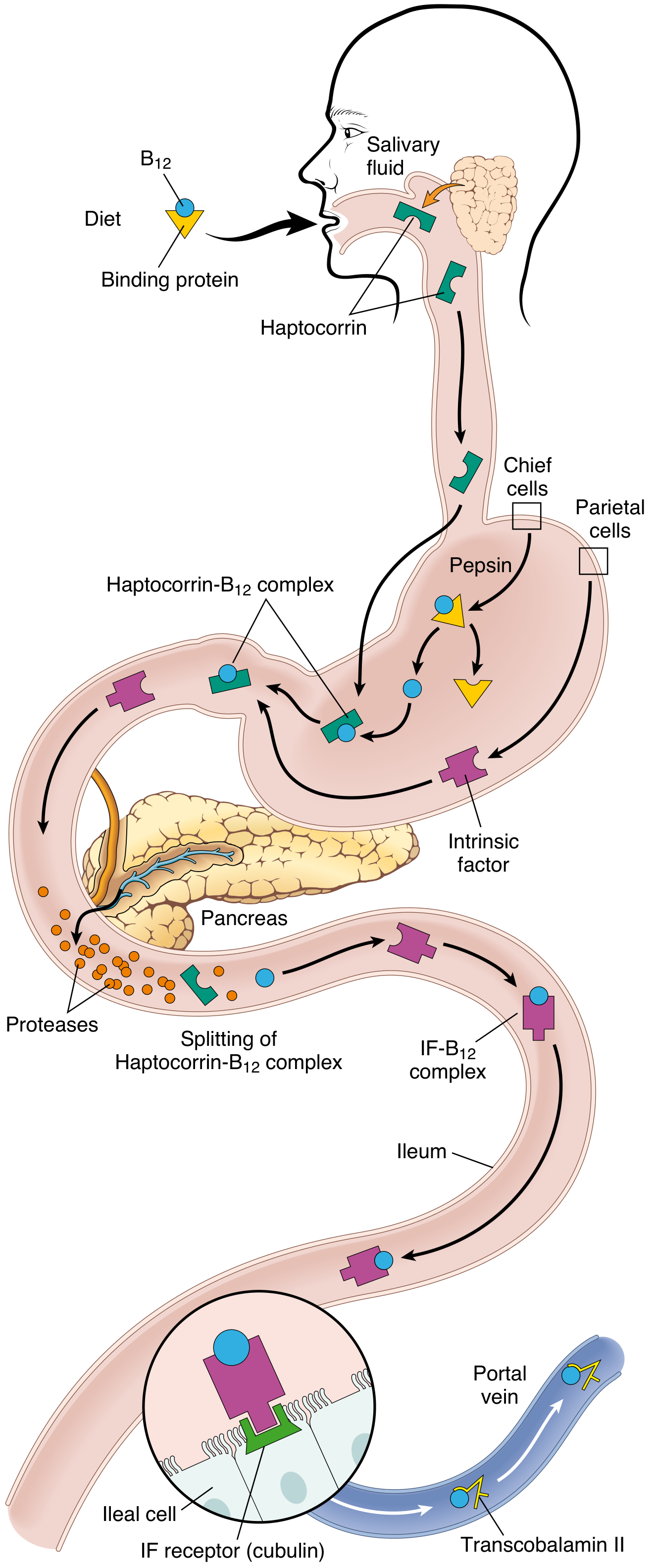
- Mouth: B12 released from food → binds salivary haptocorrin
- Stomach: Pepsin frees it → Intrinsic Factor (IF) secreted by parietal cells
- Duodenum: Pancreatic proteases split haptocorrin → B12 binds IF
- Ileum: IF-B12 complex binds cubilin receptor → endocytosed
- Blood: Transported by Transcobalamin II → liver and bone marrow
Pernicious anemia = autoimmune destruction of parietal cells → no IF → no B12 absorption
3. BIOCHEMICAL MECHANISM - THE METHYLFOLATE TRAP

- B12 (Methyl-Cbl) is needed by Methionine Synthase to convert Homocysteine → Methionine
- In doing so, N⁵-Methyl FH₄ is converted to FH₄ (active folate)
- FH₄ → N⁵'¹⁰-Methylene FH₄ → used by Thymidylate Synthetase → dUMP → dTMP → DNA
4. PERIPHERAL BLOOD SMEAR + BONE MARROW (Actual Textbook Photos)
5. CLINICAL FEATURES - BODY MAP
- Posterior columns = Proprioception lost (Romberg +ve, can't feel vibration)
- Lateral (corticospinal) = Leg spasticity (hyperreflexia, upgoing plantars)
- Peripheral nerves = Pins and needles, glove-stocking numbness
- Psychiatry = Psychosis/"megaloblastic madness"
SACD happens ONLY in B12 deficiency, NEVER in folate deficiency - this is the single most important exam point.
6. B12 vs FOLATE - KEY DIFFERENCES
| B12 | Folate | |
|---|---|---|
| Body stores | 3-5 years | 3-4 months |
| Source | Animal products only | Green vegetables |
| Absorption | Terminal ileum + IF | Proximal jejunum |
| SACD | YES | NO |
| MMA elevated | YES (specific!) | NO |
| Homocysteine | Elevated | Elevated |
| Treatment | IM injections | Oral tablets |
MMA is the key differentiator - elevated only in B12 deficiency. Both raise homocysteine.
7. TREATMENT PROTOCOL
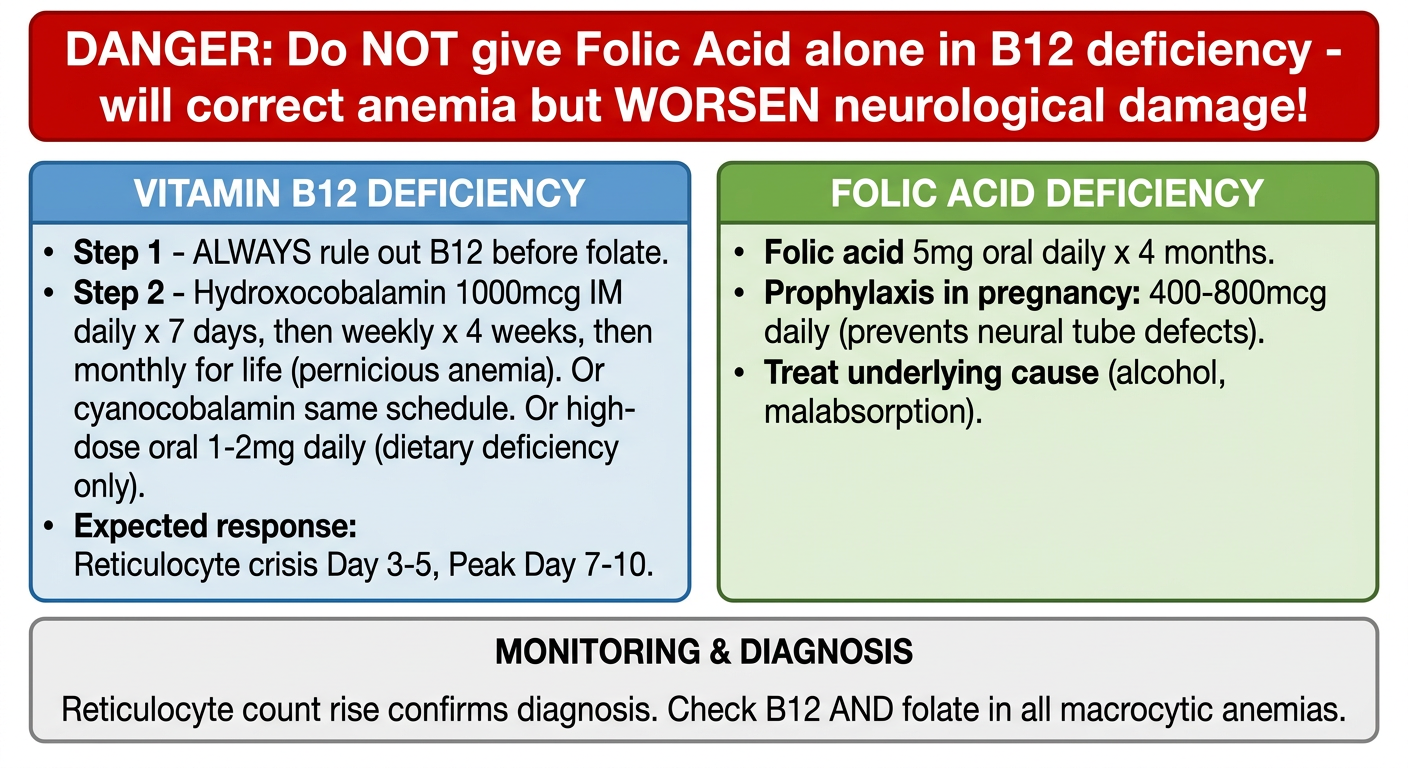
Day 1-7: 1000 mcg IM DAILY
Week 2-5: 1000 mcg IM WEEKLY
Then: 1000 mcg IM MONTHLY for life (pernicious anemia)
- Day 3-5: Reticulocyte count starts rising ("reticulocyte crisis")
- Day 7-10: Peak reticulocytosis
- Weeks-months: Neurological improvement (may be incomplete)
8. INVESTIGATIONS CHEAT SHEET
| Test | B12 Def | Folate Def | Why |
|---|---|---|---|
| MCV | >100 fL | >100 fL | Large cells |
| Peripheral smear | Macro-ovalocytes + hyperseg. neutrophils | Same | Impaired DNA |
| Serum B12 | Low | Normal | - |
| Serum/RBC folate | Normal | Low | - |
| Homocysteine | High | High | Both enzymes blocked |
| MMA | High | Normal | Only B12 pathway |
| LDH | Very high | Very high | Intramedullary hemolysis |
| Reticulocytes | Low | Low | Hypoproliferative |
| Anti-IF antibody | + (pernicious anemia) | - | Specific for PA |
| Anti-parietal cell Ab | + in 90% | - | Sensitive but not specific |
QUICK EXAM MNEMONICS
| Mnemonic | What to remember |
|---|---|
| "MMA = B12 Marker" | Only B12 deficiency raises MMA |
| "SACD = B12 Only" | Neurological damage never from folate |
| "Both raise Homocysteine" | Can't differentiate B12 from folate by Hcy alone |
| "Lemon-yellow anemia" | Combined pallor + jaundice = megaloblastic |
| "Rule out B12 FIRST" | Folate alone worsens hidden B12 neuropathy |
| "Hyperseg neut = Diagnostic" | One 6-lobed = abnormal; confirm diagnosis |
| "Hypercellular marrow + Anemia = Ineffective erythropoiesis" | Cells die inside marrow before release |
In this not included hyperpigmatation in b12 def
hyperpigmentation vitamin B12 deficiency mechanism skin nails
Medical education diagram for MBBS students - Dermatological and mucocutaneous manifestations of Vitamin B12 deficiency. Central heading: "Skin and Mucocutaneous Signs of B12 Deficiency". Show a hand and face illustration with labeled arrows pointing to: 1) Palmar creases - darkened hyperpigmentation; 2) Knuckles and dorsum of hand - hyperpigmented macules; 3) Nails - longitudinal melanonychia (brown pigmented bands); 4) Face - diffuse hyperpigmentation especially perioral; 5) Tongue - smooth, beefy red, atrophic papillae (Hunter glossitis); 6) Hair - premature graying (canities). Bottom box with mechanism: "Mechanism: B12 maintains glutathione in reduced form -> normally inhibits tyrosinase -> In B12 deficiency, tyrosinase overactive -> increased melanin synthesis -> hyperpigmentation. KEY: This is REVERSIBLE with B12 replacement. Can mimic Addison disease but no adrenal insufficiency." Bright clinical colors, clean white background, professional medical illustration style.
✅ ADDED: Hyperpigmentation in B12 Deficiency
Skin & Mucocutaneous Manifestations of B12 Deficiency
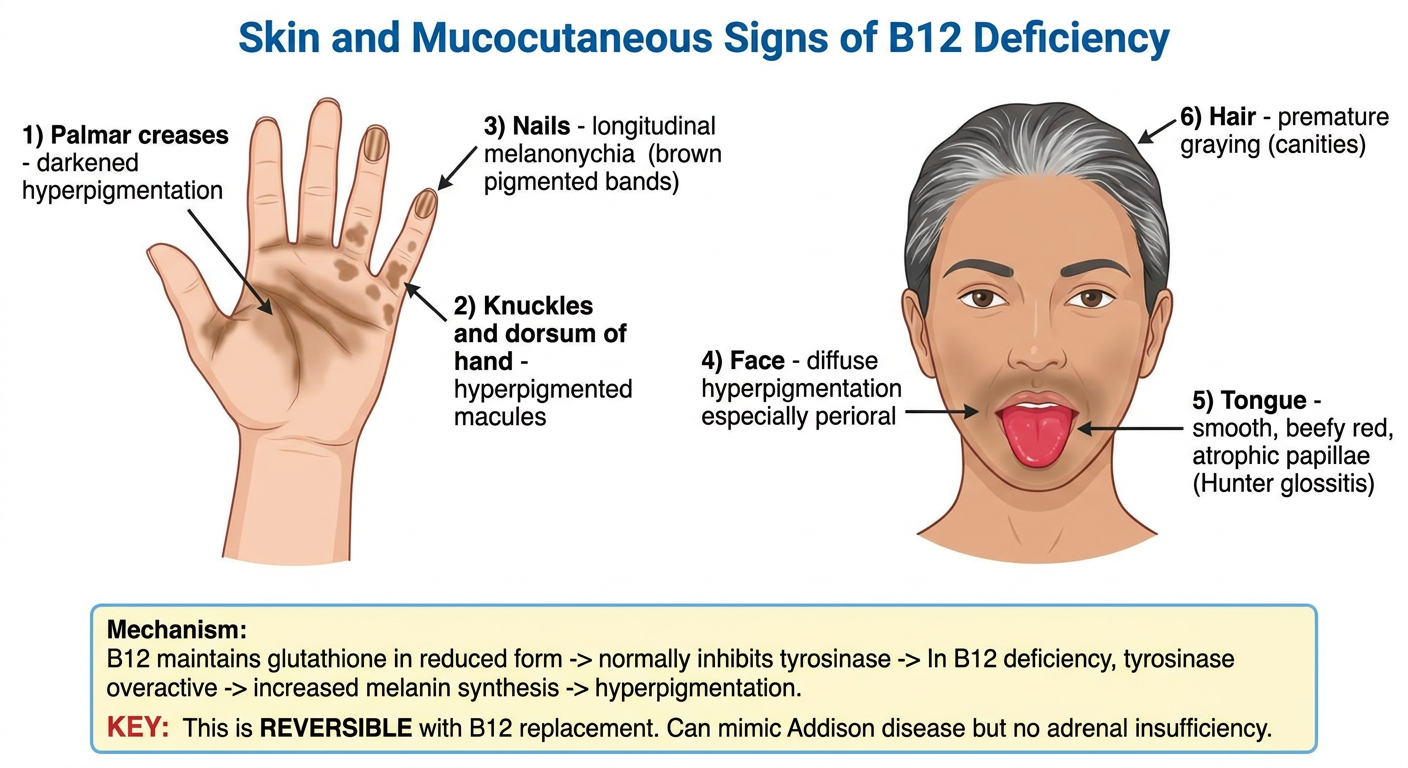
What it looks like
- Diffuse and symmetric, or scattered macules
- Most concentrated on: palmar creases, flexures, knuckles, dorsum of hands, nails, face, and pressure points
- The nails show longitudinal melanonychia (dark pigmented bands)
- Can closely mimic Addison's disease - but there is NO adrenal insufficiency (cortisol/ACTH normal)
Full Dermatological Triad of B12 Deficiency
"Glossitis, hyperpigmentation, and canities (premature greying) are the MAIN dermatologic manifestations of vitamin B12 deficiency"
| Skin Sign | Description |
|---|---|
| Hyperpigmentation | Palms, knuckles, nails, face - resembles Addison's |
| Hunter's Glossitis | Smooth, beefy-red, atrophic tongue; linear lesions early |
| Canities | Premature graying or depigmentation of hair |
| Angular cheilitis | Cracks at corners of mouth |
| Nail changes | Longitudinal melanonychia; dark bands on nails |
Note: Folate deficiency ALSO causes hyperpigmentation (identical appearance), along with glossitis and cheilitis - but WITHOUT the neurological signs.
Mechanism (3 proposed hypotheses)
-
Main mechanism - B12 normally maintains glutathione in reduced form, which inhibits tyrosinase (melanin-synthesizing enzyme). In B12 deficiency → glutathione oxidised → tyrosinase overactive → excess melanin synthesis → hyperpigmentation
-
Defective melanin transport between melanocytes and keratinocytes
-
Megaloblastic changes in keratinocytes altering melanin distribution
Electron microscopy confirms: increased melanin synthesis (not a transport defect) is the dominant mechanism. Melanosomes are normal in number.
KEY Exam Points
- Reversible - completely resolves with B12 replacement (IM injections)
- Can be the only presenting sign in mild deficiency (up to 1 in 5 patients)
- Skin manifestations may appear before hematological signs
- Mimics Addison disease - always check serum cortisol to differentiate
- Both B12 AND folate deficiency can cause hyperpigmentation - use MMA to differentiate
Updated Clinical Features Table - B12 Deficiency
| System | Features |
|---|---|
| General | Pallor, fatigue, lemon-yellow tinge |
| Skin | Hyperpigmentation (palms, knuckles, nails, face), canities (premature greying) |
| Mouth/tongue | Hunter's glossitis (smooth red tongue), angular cheilitis |
| Blood | Macro-ovalocytes, hypersegmented neutrophils, pancytopenia |
| Neurological | SACD - posterior columns + lateral columns, peripheral neuropathy, psychosis |
| GI | Achlorhydria, anorexia, diarrhea |
| Nails | Longitudinal melanonychia |
Please do not this this mistake next time in any questions i can't afford this
- Hematological - blood counts, smear findings, bone marrow
- Neurological - SACD, peripheral neuropathy, psychiatric
- Dermatological - skin, nails, hair, mucous membranes (hyperpigmentation, glossitis, canities, angular cheilitis, melanonychia)
- Gastrointestinal - tongue, GI symptoms, achlorhydria
- Other/Systemic - cardiovascular, endocrine associations