SAAG
Reading File
Finding Sources
Searching PubMed
serum ascites albumin gradient SAAG ascites
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
SAAG serum ascites albumin gradient algorithm portal hypertension
Here is a comprehensive overview of the Serum-Ascites Albumin Gradient (SAAG):
Serum-Ascites Albumin Gradient (SAAG)
What is SAAG?
SAAG = Serum albumin − Ascitic fluid albumin
It is a simple subtraction (not a ratio), calculated from samples drawn on the same day. It does not change with diuresis.
Physiology
The SAAG reflects oncotic-hydrostatic pressure balance in the hepatic sinusoids — specifically, it correlates with the hepatic venous pressure gradient (HVPG). A high SAAG indicates elevated sinusoidal pressure (portal hypertension), where the osmotic pressure of albumin counterbalances the increased portal pressure per Starling's law. — Harrison's Principles of Internal Medicine 22E, p. 1329
Interpretation
| SAAG | Interpretation | Mechanism |
|---|---|---|
| ≥ 1.1 g/dL | Portal hypertension–related ascites | ~97% accurate for portal HTN |
| < 1.1 g/dL | Non–portal hypertension ascites | Excludes portal HTN |
Causes by SAAG Category
High SAAG (≥ 1.1 g/dL) — Portal hypertension
- Cirrhosis
- Alcoholic hepatitis
- Congestive heart failure / constrictive pericarditis
- Budd-Chiari syndrome (hepatic vein thrombosis)
- Sinusoidal obstruction syndrome (veno-occlusive disease)
- Portal vein thrombosis
- Massive liver metastases
- Fulminant liver failure
- Fatty liver of pregnancy
- Myxedema
Low SAAG (< 1.1 g/dL) — Non–portal hypertension
- Peritoneal carcinomatosis
- Tuberculous peritonitis
- Nephrotic syndrome
- Pancreatic ascites
- Biliary ascites / leak
- Peritoneal mesothelioma
- Chylous ascites
- Bowel obstruction/infarction
- Serositis (connective tissue diseases)
— Yamada's Textbook of Gastroenterology, 7th ed. | Sleisenger & Fordtran's GI & Liver Disease
Refining Diagnosis Within High-SAAG Ascites
When SAAG ≥ 1.1 g/dL, ascitic fluid total protein helps narrow the cause further:
| SAAG ≥ 1.1 | Ascitic protein | Cause |
|---|---|---|
| ≥ 1.1 | < 2.5 g/dL | Cirrhosis, late Budd-Chiari, massive liver metastases (sinusoids damaged/scarred — protein doesn't cross) |
| ≥ 1.1 | ≥ 2.5 g/dL | Cardiac ascites, early Budd-Chiari, IVC obstruction, sinusoidal obstruction syndrome (sinusoids intact — protein crosses freely) |
Pro-tip: Serum BNP elevation supports cardiac ascites in high-SAAG cases. — Harrison's 22E, p. 1948
Diagnostic Algorithm
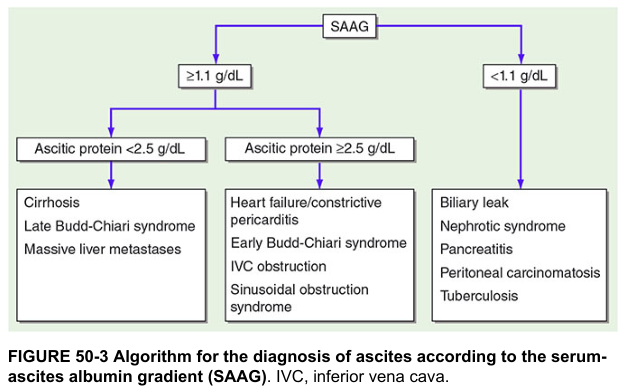
Figure: SAAG-based algorithm for diagnosing ascites etiology — Harrison's Principles of Internal Medicine
How to Measure
- Perform diagnostic paracentesis (left lower quadrant preferred — greater depth of ascites, thinner abdominal wall)
- Send ascitic fluid for: albumin, total protein, cell count with differential, Gram stain/culture if infection suspected
- Draw serum albumin simultaneously
- Calculate: SAAG = serum albumin − ascitic albumin
Accuracy: ~97% for diagnosing portal hypertension — Pfenninger & Fowler's Procedures for Primary Care | Sleisenger & Fordtran's
Clinical Pearls
- SAAG is the preferred method over the older transudate/exudate classification by total protein alone
- SAAG does not identify the specific cause of ascites — it only indicates whether portal hypertension is present
- "Mixed" ascites can occur (e.g., cirrhosis + peritoneal carcinomatosis) — SAAG may still be ≥ 1.1 due to the dominant portal hypertension component
- If the cause remains unclear after history, exam, blood tests, and ultrasound, SAAG is a key next step — Sleisenger & Fordtran's, p. 4220
Types of dysphagia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
dysphagia types oropharyngeal esophageal classification causes diagram
Reading File
Here is a comprehensive overview of the types of dysphagia:
Dysphagia — Classification
Dysphagia (Greek: dys = disordered + phagia = to eat) — the sensation that food is hindered in its passage from the mouth to the stomach.
The primary division is anatomical location:
1. Oropharyngeal Dysphagia (Transfer Dysphagia)
Definition: Inability to propel a food bolus from the hypopharynx through the upper esophageal sphincter (UES) into the esophageal body.
Key clinical features:
- Difficulty initiating the swallow (within 1 second of swallowing)
- Nasal regurgitation, coughing/choking during eating, drooling
- Aspiration — food enters the trachea rather than the esophagus
- Associated dysarthria, nasal speech
- Patient localizes symptoms to the cervical region
- Often worse with liquids than solids (opposite of esophageal mechanical dysphagia)
Causes:
| Category | Examples |
|---|---|
| Neuromuscular | Stroke, Parkinson disease, ALS, multiple sclerosis, myasthenia gravis, Guillain-Barré, polymyositis/dermatomyositis, postpolio syndrome, Huntington disease, brainstem tumors |
| Structural | Zenker diverticulum, cervical web, cricopharyngeal bar, carcinoma, osteophytes, Chagas disease (in endemic areas), thyromegaly, post-surgical/radiation changes |
| Other | Poor dentition/dentures, xerostomia (medications, radiation, Sjögren), idiopathic UES dysfunction |
— Sleisenger & Fordtran's GI & Liver Disease, p. 190
2. Esophageal Dysphagia
Definition: Impaired transit of the bolus through the esophageal body. Divided into two major subtypes:
2a. Mechanical (Structural/Obstructive) Dysphagia
Mechanism: Fixed luminal narrowing prevents bolus passage despite normal peristalsis.
Classic pattern: Dysphagia to solids only initially; progresses to liquids if obstruction becomes severe.
Intrinsic causes:
- Esophageal carcinoma / benign tumors
- Peptic stricture (GERD-related)
- Schatzki ring (lower esophageal ring)
- Eosinophilic esophagitis (EoE)
- Esophageal webs
- Diverticula
- Medication-induced stricture
- Foreign body
Extrinsic causes:
- Mediastinal mass
- Vascular compression (dysphagia lusoria — aberrant right subclavian artery)
- Spinal osteophytes
Clinical clues by pattern:
| Pattern | Likely cause |
|---|---|
| Episodic, non-progressive, solids only | Schatzki ring, esophageal web |
| Progressive over weeks–months | Carcinoma |
| Young patient with atopy, food impactions | Eosinophilic esophagitis |
| Prolonged heartburn → dysphagia | Peptic stricture |
2b. Motor (Neuromuscular / Motility) Dysphagia
Mechanism: Failure of orderly peristaltic contractions or LES relaxation.
Classic pattern: Dysphagia for both solids AND liquids from the start.
Primary motility disorders:
- Achalasia — absent peristalsis + incomplete LES relaxation; nocturnal regurgitation of undigested food; equal difficulty with solids and liquids
- Distal esophageal spasm (DES) — episodic dysphagia + chest pain; sensitivity to hot/cold liquids
- Hypercontractile (jackhammer) esophagus
- Nutcracker (high-pressure) esophagus
- Esophagogastric junction outflow obstruction (EGJOO)
Secondary motility disorders:
- Scleroderma (systemic sclerosis) — absent peristalsis in distal esophagus; reflux + mild dysphagia; heartburn common; Raynaud phenomenon
- Chagas disease (Trypanosoma cruzi)
- Reflux-related dysmotility
- Other rheumatologic disorders
— Sleisenger & Fordtran's | Yamada's Textbook of Gastroenterology, 7th ed.
3. Functional Dysphagia
When no structural, motility, or mucosal cause can be identified despite thorough workup, symptoms are classified under functional dysphagia per the Rome IV criteria. Abnormal visceral sensory perception (hypersensitivity to esophageal distension) likely plays a role. — Yamada's, p. 872
Diagnostic Algorithm
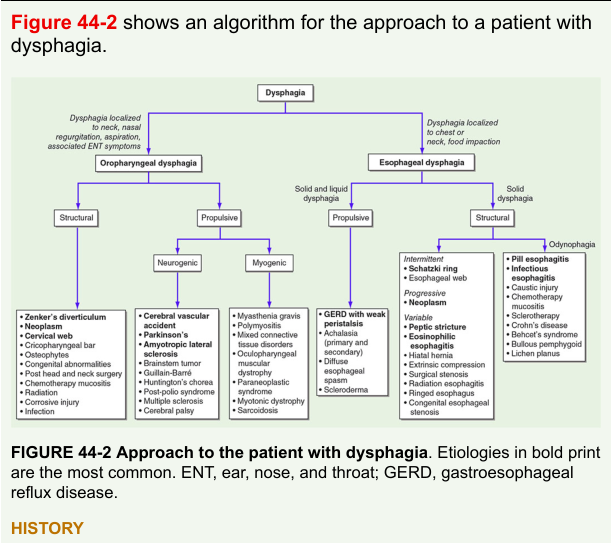
Figure: Approach to dysphagia, distinguishing oropharyngeal vs. esophageal causes, then structural vs. propulsive — Harrison's Principles of Internal Medicine
Key Differentiating Features at a Glance
| Feature | Oropharyngeal | Esophageal — Mechanical | Esophageal — Motor |
|---|---|---|---|
| Site of symptoms | Neck / cervical | Lower sternum / epigastric | Lower sternum |
| Onset after swallowing | Immediate (≤1 sec) | Delayed | Delayed |
| Solids vs. liquids | Worse with liquids | Solids only initially | Both solids & liquids |
| Progression | Variable | Progressive (if malignant) | Often intermittent |
| Associated features | Cough, aspiration, nasal regurgitation, dysarthria | Weight loss, heartburn, food impaction | Chest pain, regurgitation of undigested food |
| Initial investigation | Modified barium swallow | Endoscopy / barium swallow | High-resolution manometry |
— Harrison's Principles of Internal Medicine 22E | Sleisenger & Fordtran's GI & Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.