Write detailed about origin , insertion, nerve supply, action of facial nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed to write a comprehensive, well-illustrated answer. Let me compose it.
Facial Nerve (Cranial Nerve VII) - Detailed Anatomy
Overview
The facial nerve (CN VII) is the nerve of the second branchial arch. It contains approximately 7,000-10,000 fibers and carries five functional modalities:
| Modality | Type | Function |
|---|---|---|
| Special Visceral Efferent (SVE) | Motor | Muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric |
| General Visceral Efferent (GVE) | Parasympathetic | Lacrimal, submandibular, sublingual glands; nasal/palatal seromucinous glands |
| Special Visceral Afferent (SVA) | Taste | Anterior 2/3 of tongue (via chorda tympani); palate and tonsillar fossa (via GSPN) |
| General Somatic Afferent (GSA) | Sensation | Skin of EAC, conchal skin, posterior auricle |
| Visceral Afferent | Reflex | Mucosa of nose, pharynx, palate |
Origin (Central / Nuclear)
The facial nerve has three brainstem nuclei:
-
Facial Motor Nucleus - Located in the lateral portion of the anterior pons (branchial motor column), more caudally than the trigeminal motor nucleus. It is composed of four cell groups. The fascicles from this nucleus loop dorsally around the abducens (CN VI) nucleus, forming the facial colliculus on the floor of the fourth ventricle - this is why a pontine lesion involving CN VII almost always also involves CN VI.
-
Superior Salivatory Nucleus - Origin of preganglionic parasympathetic (GVE) fibers carried in the nervus intermedius. Supplies the lacrimal, submandibular and sublingual glands.
-
Nucleus of the Tractus Solitarius - Receives special visceral afferent (taste) fibers from the anterior 2/3 of the tongue via the chorda tympani.
The motor root (larger trunk) and the nervus intermedius (smaller sensory/parasympathetic root, "nerve of Wrisberg") emerge separately from the brainstem at the pontomedullary junction, ventrolaterally, in the region called the cerebellopontine angle (CPA).
-
- The facial nerve is 1.8 mm in diameter vs 3 mm for CN VIII
-
- It exits 1.5 mm anterior, medial, and superior to CN VIII
-
- It crosses the CPA a distance of 15-17 mm together with CN VIII and the nervus intermedius
Course and Segments
1. Intracranial Segment (Cerebellopontine Angle)
The nerve traverses the subarachnoid space of the CPA before entering the internal auditory meatus (IAC). Within the IAC (~8-10 mm in length), the facial nerve lies in the anterosuperior quadrant; the superior and inferior vestibular nerves lie posterior to it, and the cochlear nerve lies caudally. By the lateral end (fundus) of the IAC, the facial nerve has merged with the nervus intermedius.
2. Intratemporal Segment (within the Fallopian Canal)
The facial nerve travels within the fallopian (facial) canal - the longest bony canal of any cranial nerve - from the fundus of the IAC to the stylomastoid foramen. It is divided into three segments:
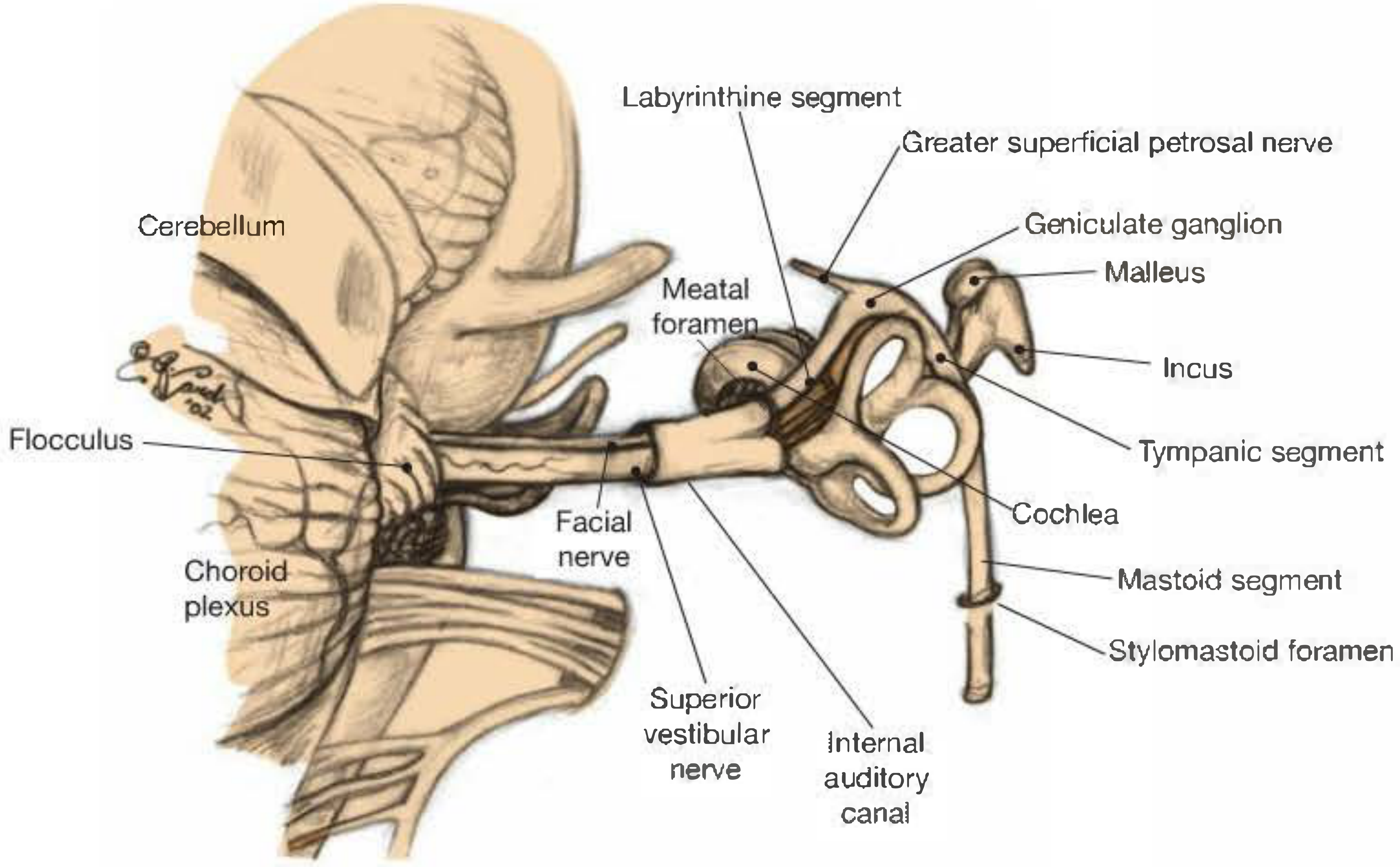
a) Labyrinthine Segment (4 mm)
- First, shortest, and narrowest segment
- Enters through the meatal foramen (~0.68 mm diameter) - the narrowest portion of the entire canal
- A dense arachnoid band at the lateral IAC and the narrow meatal foramen together create an anatomical "bottleneck" - critical in Bell's palsy, where nerve edema is constricted here
- Courses posterocephalad to the cochlea, anteromedial to the ampulla of the superior semicircular canal, cephalad to the vestibule
- Opens into the geniculate fossa (just deep to the squamous temporal region)
b) Tympanic (Horizontal) Segment (11 mm)
- Begins at the geniculate ganglion where the nerve makes its first (internal) genu - a sharp 75-degree posterior turn
- The geniculate ganglion contains bipolar ganglion cells for sensory functions (taste and somatic sensation). It has a separate developmental origin from the facial nerve itself (well defined by the 7th embryonic week). It is separated from the middle fossa by only a thin layer of bone, which is dehiscent in ~25% of ears
- From the geniculate ganglion, the Greater Superficial Petrosal Nerve (GSPN) arises and runs anteriorly along the middle fossa floor
- The horizontal segment occupies the medial wall of the anterior attic, passes over the cochleariform process, and forms the superior wall of the oval window niche. The bony wall of this segment is dehiscent in 35-55% of the population, especially above the oval window
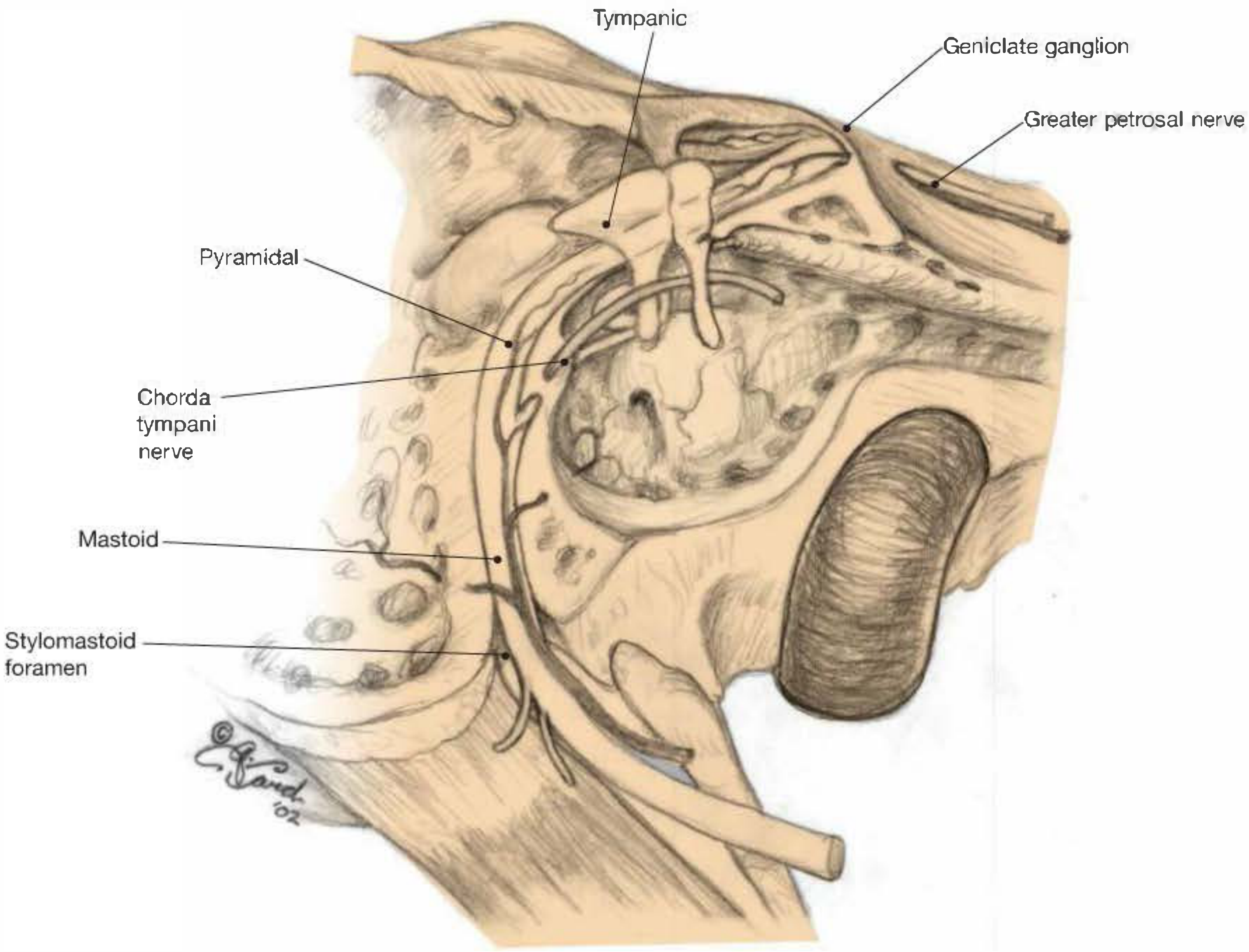
c) Mastoid (Vertical) Segment (13 mm)
- At the pyramidal eminence (where the stapedius tendon emerges), the nerve makes a second (external) genu into the vertical mastoid segment
- This turn is anteroinferior to the lateral semicircular canal
- The nerve to stapedius arises at or near the second genu
- Approximately midway, the chorda tympani nerve arises (though both branches can arise anywhere between the second genu and the stylomastoid foramen)
- The vertical segment exits the temporal bone through the stylomastoid foramen
3. Extratemporal Segment
After exiting the stylomastoid foramen, the facial nerve:
- Immediately gives off the posterior auricular branch - motor to the occipitalis and posterior auricular muscles
- Enters the posterior aspect of the parotid gland - the entry point is located at the midpoint of a line drawn from the superior border of the tragus to the angle of the mandible
- Divides into upper (temporofacial) and lower (cervicofacial) trunks
- These pass through the parotid gland with further branching and anastomosis
- Five terminal groups emerge from the borders of the parotid gland
Five Terminal Branches - Nerve Supply, Muscles (Insertion), and Actions
1. Temporal Branch
- Origin: Upper division (temporofacial trunk)
- Course: Usually 3-5 rami that originate over the middle third of the zygomatic arch; courses between the SMAS and deep fascia, then penetrates the undersurface of muscles
- Muscles supplied (insertion sites):
- Frontalis - inserted into the skin and subcutaneous tissue of the forehead
- Upper orbicularis oculi - encircles the orbital aperture
- Corrugator supercilii - inserts into the skin of the medial eyebrow
- Anterior and superior auricular muscles - insert into the auricle
- Actions:
- Raises the eyebrows (frontalis)
- Closes the eyelids (orbicularis oculi - upper portion)
- Draws the eyebrows medially and inferiorly, creating frowning wrinkles (corrugator supercilii)
- Moves the auricle anteriorly/superiorly
- Clinical note: This is the most at-risk branch during temple surgery. Injury causes brow ptosis, forehead flattening, and inability to raise the eyebrow - with long-term upper visual field compromise
2. Zygomatic Branch
- Origin: Upper division (temporofacial trunk)
- Course: Runs horizontally and upward after emerging from the parotid gland
- Muscles supplied (insertion sites):
- Lower orbicularis oculi - lower eyelid and cheek
- Procerus - inserts into the skin between the eyebrows
- Mouth elevator muscles (zygomaticus major and minor)
- Nasal muscles (nasalis, compressor narium)
- Actions:
- Closes the lower eyelid
- Draws the skin of the forehead downward (procerus - produces horizontal wrinkles at the root of the nose)
- Elevates the corner of the mouth and upper lip (smiling)
- Compresses/dilates the nostril
3. Buccal Branch
- Origin: Both upper and lower divisions (most anastomotic branch)
- Course: Runs horizontally across the cheek, deep in the parotid tissue - least at risk branch due to depth and abundant anastomoses
- Muscles supplied (insertion sites):
- Orbicularis oris - encircles the mouth opening
- Buccinator - inserts into the orbicularis oris at the angle of the mouth
- Risorius - inserts into the skin at the angle of the mouth
- Levator labii superioris and accessory elevator muscles
- Mentalis (partially, with marginal mandibular)
- Actions:
- Closes and protrudes the lips (orbicularis oris - e.g., kissing, whistling)
- Compresses the cheeks against the teeth during mastication, preventing food accumulating in the vestibule (buccinator)
- Retracts the angle of the mouth laterally - "grinning" (risorius)
4. Marginal Mandibular Branch
- Origin: Lower division (cervicofacial trunk)
- Course: Exits the inferior portion of the parotid gland, courses over the mandible anterior to the facial artery, located 1-2 cm above the inferior border of the mandible
- Muscles supplied (insertion sites):
- Orbicularis oris (lower portion) - encircles the mouth
- Risorius
- Depressor anguli oris - inserts into the angle of the mouth
- Depressor labii inferioris - inserts into the lower lip skin
- Mentalis - inserts into the skin of the chin
- Actions:
- Depresses the lower lip and corner of the mouth (frowning)
- Protrudes and wrinkles the chin skin (mentalis)
- Closes the lower mouth
- Clinical note: Injury causes ipsilateral crooked smile, drooling, and inability to fully depress the lower lip
5. Cervical Branch
- Origin: Lower division (cervicofacial trunk)
- Course: Passes inferiorly to the neck, deep to platysma
- Muscles supplied (insertion sites):
- Platysma - broad sheet inserted into skin of lower face, mandible, and clavicle region
- Actions:
- Draws the angle of the mouth downward and laterally
- Tenses the skin of the neck
- Assists in depressing the mandible
Additional Motor Branches (arise before parotid division)
| Branch | Muscle | Action |
|---|---|---|
| Posterior auricular nerve | Occipitalis, posterior auricular m. | Draws the scalp posteriorly; moves auricle posteriorly |
| Nerve to stylohyoid | Stylohyoid | Draws hyoid bone posterosuperiorly |
| Nerve to posterior digastric | Posterior belly of digastric | Elevates hyoid / depresses mandible |
| Nerve to stapedius | Stapedius | Dampens ossicular movements (acoustic reflex); protective against loud noise |
Autonomic (Parasympathetic) Branches - Nerve Supply
These arise from the superior salivatory nucleus via the nervus intermedius:
Greater Superficial Petrosal Nerve (GSPN)
- Arises from the geniculate ganglion
- Carries preganglionic parasympathetic fibers - synapses in the pterygopalatine ganglion
- Postganglionic fibers innervate:
- Lacrimal gland (lacrimation)
- Seromucinous glands of the nasal cavity and palate
- Also carries taste fibers from the soft palate
Chorda Tympani Nerve
- Arises in the mastoid segment of the fallopian canal (~midway)
- Traverses the middle ear (between malleus and incus), exits the skull via the petrotympanic fissure
- Joins the lingual nerve (CN V3) in the infratemporal fossa
- Carries:
- Preganglionic parasympathetics - synapse in the submandibular ganglion - postganglionic fibers supply the submandibular and sublingual glands (salivation)
- Taste (SVA) fibers from the anterior 2/3 of the tongue
Summary Table: Fiber Types and Their Origins/Targets
| Fiber Type | Nucleus of Origin | Ganglion | Target Organ |
|---|---|---|---|
| SVE (Motor) | Facial motor nucleus (pons) | - | Muscles of facial expression, stapedius, stylohyoid, posterior digastric |
| GVE (Parasympathetic) via GSPN | Superior salivatory nucleus | Pterygopalatine ganglion | Lacrimal gland, nasal/palatal glands |
| GVE (Parasympathetic) via chorda tympani | Superior salivatory nucleus | Submandibular ganglion | Submandibular, sublingual glands |
| SVA (Taste) via chorda tympani | - | Geniculate ganglion (cell bodies) | Anterior 2/3 tongue |
| SVA (Taste) via GSPN | - | Geniculate ganglion (cell bodies) | Soft palate, tonsillar fossa |
| GSA (Somatic sensation) | - | Geniculate ganglion (cell bodies) | EAC skin, conchal skin of auricle |
Upper vs Lower Motor Neuron Lesions
Understanding the dual cortical innervation of the facial nucleus is clinically important:
- The upper facial muscles (forehead/brow) receive bilateral cortical input (from both hemispheres)
- The lower facial muscles receive predominantly contralateral cortical input
| Type | Lesion Site | Forehead | Lower Face | Example |
|---|---|---|---|---|
| UMN (central) | Cortex or corticobulbar tracts | Spared (bilateral cortical supply) | Contralateral weakness | Hemispheric stroke |
| LMN (peripheral) | Facial nucleus, fascicles, or peripheral nerve | Involved (complete ipsilateral palsy) | Ipsilateral weakness | Bell's palsy, parotid tumor |
Sources: Shambaugh Surgery of the Ear, p. 644-645; Neuroanatomy through Clinical Cases, 3rd Ed.; Cummings Otolaryngology Head and Neck Surgery; Dermatology 2-Volume Set, 5th Ed., p. 2927-2928; Gray's Anatomy for Students; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.