What is pulse’s paradox
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Pulsus Paradoxus
Pulsus paradoxus (sometimes called "paradoxical pulse") is an exaggeration of the normal inspiratory drop in systolic blood pressure. It is defined as a fall in systolic BP greater than 10 mmHg during inspiration.
Why "Paradox"?
The name was coined by Adolf Kussmaul in 1873. He noted that in cardiac tamponade, the heart sounds continued while the radial pulse disappeared - a pulse "paradoxically" absent despite a beating heart. The heart was still contracting, yet the peripheral pulse vanished with each breath.
Normal Physiology
During normal inspiration:
- Intrathoracic pressure falls
- Right ventricular (RV) filling increases
- Systolic BP drops slightly, usually <10 mmHg
This small variation is completely normal.
Mechanism of Pulsus Paradoxus
The diagram below (from Miller's Anesthesia) shows three pathways during inspiration that together reduce left ventricular output:
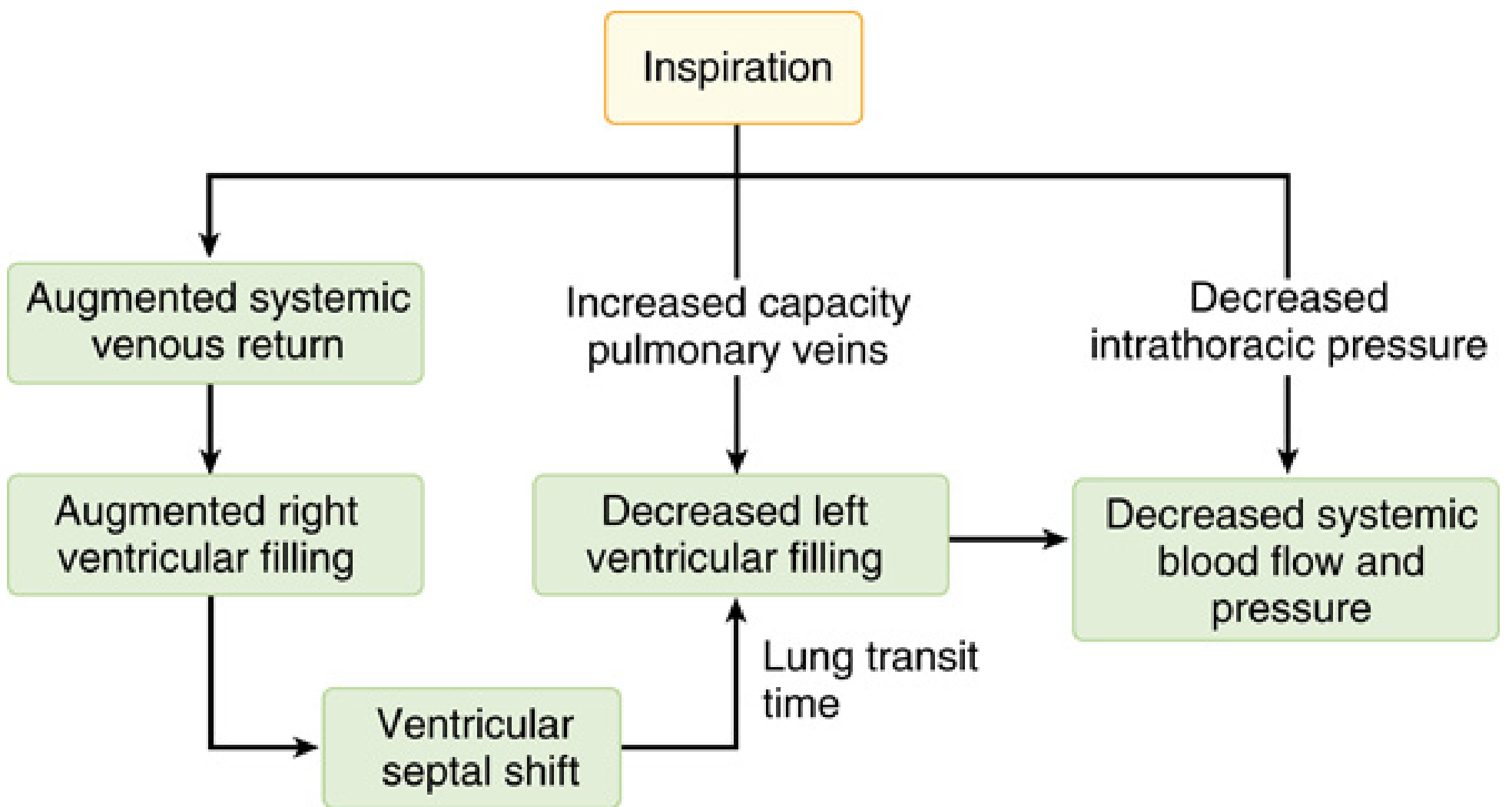
Three simultaneous mechanisms act on inspiration:
- Ventricular interdependence - Augmented systemic venous return fills the RV more. The distended RV shifts the interventricular septum leftward (septal shift), reducing LV filling volume.
- Increased pulmonary vascular capacitance - The expanded lungs pool blood in pulmonary veins, reducing pulmonary venous return to the left heart.
- Decreased intrathoracic pressure - Increases the LV afterload relative to the aorta (the aorta is outside the chest and therefore at higher pressure relative to the falling intrathoracic environment).
The net result: decreased LV filling → decreased stroke volume → fall in systolic BP on inspiration.
In cardiac tamponade, the pericardial fluid creates a fixed total pericardial volume, so when the RV expands during inspiration, it forcibly compresses the LV (exaggerated ventricular interdependence), making the drop much larger than normal.
How to Measure It
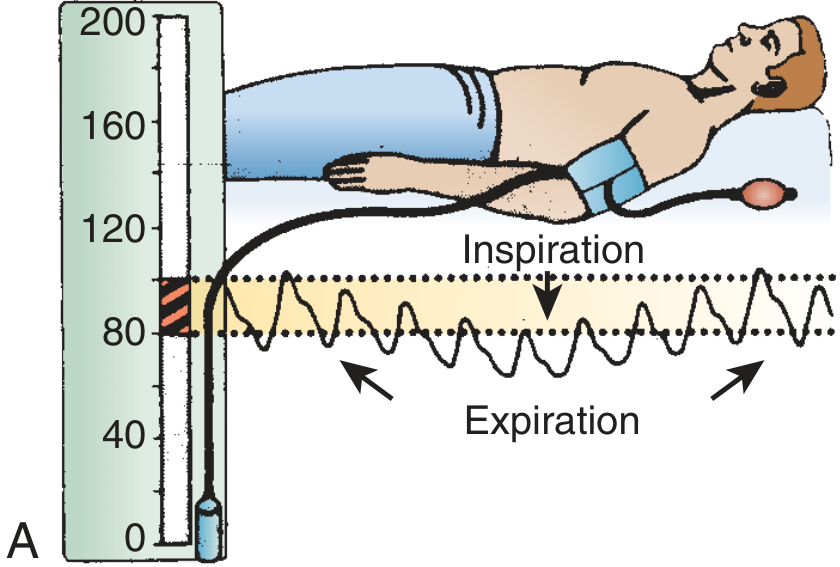
Using a sphygmomanometer:
- Patient reclines at 30-45 degrees, breathing normally
- Inflate BP cuff above systolic pressure
- Slowly deflate until Korotkoff sounds are first heard (expiration only) - record this pressure
- Continue deflating until sounds are heard throughout the entire respiratory cycle - record this pressure
- The difference between these two values = pulsus paradoxus
>12 mmHg = abnormal (most tamponade patients show 20-30 mmHg or greater)
An alternative bedside method: observe the pulse oximetry waveform disappearing on inspiration and reappearing on expiration.
- Note: pulsus paradoxus is hard to measure in tachycardia, atrial fibrillation, or tachypnea. It becomes palpable at the radial/femoral artery when the difference exceeds 15 mmHg.
Causes
| Category | Examples |
|---|---|
| Pericardial | Cardiac tamponade (classic cause), constrictive pericarditis |
| Pulmonary | Severe asthma, COPD, tension pneumothorax |
| Vascular | Massive pulmonary embolism, hypovolemic/hemorrhagic shock |
Important Exceptions
Pulsus paradoxus may be absent in tamponade if the patient has:
- Aortic insufficiency (AR)
- Atrial septal defect (ASD)
- Pre-existing elevated LV end-diastolic pressure (e.g., LV hypertrophy or dilation)
These conditions independently reduce LV filling or pressure variations, masking the paradox.
Sources: - Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 44 | Miller's Anesthesia 10e, p. 7763 | Harrison's Principles of Internal Medicine 22e, p. 1906
This is a shared conversation. Sign in to Orris to start your own chat.