Ostiomylitis
Reading File
Finding Sources
Searching PubMed
osteomyelitis diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive information to write a thorough answer on osteomyelitis. Let me compile it.
Osteomyelitis
Osteomyelitis is inflammation of bone and bone marrow, virtually always caused by infection. It is one of the most challenging musculoskeletal infections to treat because of its tendency to become chronic and its ability to destroy bone architecture.
Definition
Bone infection where organisms reach bone via:
- Hematogenous spread (most common in children)
- Contiguous spread from adjacent soft tissue or joint
- Direct inoculation - trauma, surgery, open fractures
Robbins & Kumar Basic Pathology
Microbiology
| Setting | Likely Organisms |
|---|---|
| Children (all ages) | S. aureus (MRSA most common in AHO) |
| Neonates | Group B Streptococcus, E. coli |
| Adults (general) | S. aureus, gram-negative rods |
| Sickle cell disease | Salmonella, gram-negatives |
| IV drug users / spinal | S. aureus, Pseudomonas aeruginosa |
| Diabetic foot | Polymicrobial (gram-positive + anaerobes) |
| Post-trauma/surgery | Polymicrobial |
| Neonatal | S. aureus, Group B Streptococcus |
S. aureus is the most common overall cause - its cell wall proteins bind collagen in bone matrix, facilitating adhesion. No organism is identified in nearly 50% of cases.
Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine
Pathophysiology
Acute Phase (first 48 hours)
- Bacteria proliferate → neutrophilic inflammation
- Necrosis of bone cells and marrow ensues within 48 hours
- Infection spreads through Haversian systems to reach the periosteum
- Purulent material forms → abscess → pressure-driven bony destruction
- Pus passes through cortical bone and elevates the periosteum, rendering cortical bone avascular
Why the metaphysis?
In children, the metaphysis of long bones is the primary site because:
- Slow blood flow through looped capillary vessels
- Combined microtrauma - both encourage bacterial seeding during bacteremia
- The terminal capillaries lack phagocytic lining cells
Chronic Phase (after 1 week)
- Chronic inflammatory cells release cytokines stimulating osteoclastic resorption
- Dead bone = sequestrum
- New bone forming a living shell around the sequestrum = involucrum
- The involucrum has drainage gaps; pus can track through these into soft tissue and eventually to the skin surface as sinus tracts
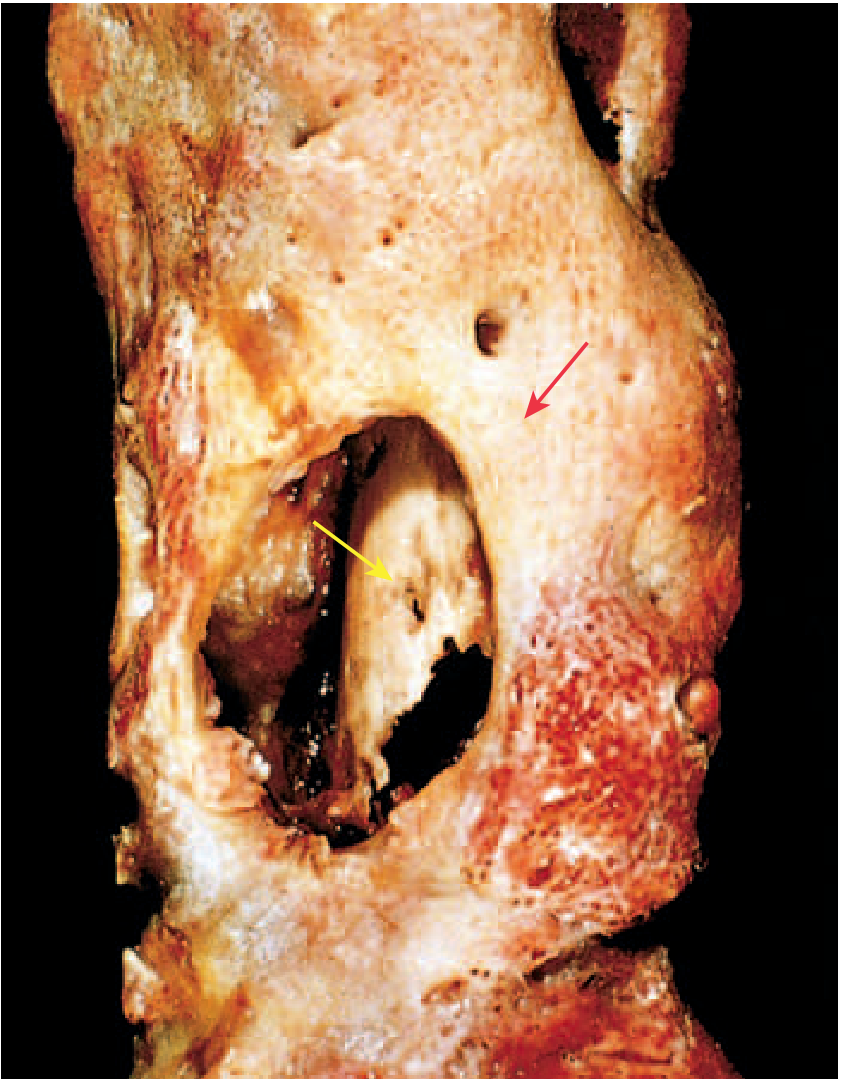
Robbins & Kumar Basic Pathology, p. 779; Bailey and Love's Short Practice of Surgery
Classification
By Duration
- Acute: Days to weeks - fever, leukocytosis, elevated inflammatory markers
- Subacute: Slow onset, symptoms less prominent; cultures often negative
- Chronic: Persistent or recurrent after acute episode; sequestrum/involucrum present; sinus tracts may form
By Age Group / Clinical Subset
Children (Acute Hematogenous Osteomyelitis - AHO)
- Male:female ratio 2-3:1
- Long bones involved ~80% of time (distal metaphysis most common)
- Fever, chills, pain, point tenderness, refusal to bear weight
- Blood cultures positive in ~40%; tissue cultures positive 86%
- MRSA now the most common cause
Neonates
- Often post-abnormal pregnancy or delivery
- Multiple sites in ~50% of cases
- Septic arthritis often accompanies osteomyelitis (unique neonatal vascular anatomy allows metaphyseal vessels to penetrate the growth plate)
- Leading pathogen: Group B Streptococcus
Adults / Vertebral Osteomyelitis
- Increasing with aging population and chronic diseases
- Risk factors: IV access devices, indwelling lines, urinary infections, IV drug use
- Lumbar (58%) > thoracic (30%) > cervical (11%)
- Only ~10% appear septic/toxic - most present insidiously
- Back pain is the most common symptom (~90%), with spinous process tenderness
- Diagnostic delay up to 4 months is common
- ESR elevated in 98%, CRP in 100% of cases
- Epidural abscess accompanies it in many cases - up to 60% present without fever or leukocytosis
Diabetic Foot / Contiguous Spread
- Most common in adults; polymicrobial
- Often complication of open fractures, surgery, or DM ulcers
ROSEN's Emergency Medicine; Goldman-Cecil Medicine
Clinical Features
Symptoms
- Fever, rigors (may appear toxic)
- Systemic: headache, fatigue, malaise, anorexia
- Localized pain - throbbing in nature, progressive
- Limp or inability to bear weight (children with lower extremity involvement)
Signs
- Point tenderness over the infected bone segment (cardinal finding)
- Palpable warmth, soft tissue swelling, erythema
- In chronic osteomyelitis: palpable involucrum or sequestrum, skin sinus tracts
- Sympathetic effusion in adjacent joint (even without joint infection)
ROSEN's Emergency Medicine
Investigation
Laboratory
- FBC: Leukocytosis (may be absent in chronic cases)
- ESR: Elevated in 98% of vertebral osteomyelitis
- CRP: Elevated in ~100% of vertebral osteomyelitis; most sensitive marker
- Blood cultures: Before starting antibiotics; positive in ~40% of AHO / vertebral cases
- Bone biopsy with culture: Gold standard for identifying causative organism - obtain whenever possible
Imaging
Plain radiography
- First-line but has a major limitation: changes lag behind disease by 10-14 days (up to 2 weeks)
- Early signs: soft tissue swelling only
- Later: cortical irregularity (bony destruction), periosteal reaction
- Plain films are often normal in the first 2 weeks
MRI (modality of choice)
- Highest sensitivity and specificity
- Shows marrow edema, abscess, periosteal reaction early
- Identifies epidural extension in vertebral osteomyelitis
- "Penumbra sign" in subacute infection: peripheral high-signal ring of granulation tissue surrounding low-signal abscess cavity
- Contrast-enhanced fat-suppressed sequences show avid enhancement
CT
- Good for defining cortical destruction and detecting sequestra
- Often used to guide needle biopsy
- Higher radiation dose
Ultrasound
- Useful in children and infants
- Detects subperiosteal abscess, guides aspiration
- Normal US does not exclude osteomyelitis
Bone scintigraphy (Tc-99m MDP)
- Useful when MRI is unavailable or contraindicated
- 3-phase scan increases specificity
- Used for multifocal infection screening (whole-body)
Grainger & Allison's Diagnostic Radiology; ROSEN's Emergency Medicine
Diagnostic Algorithm
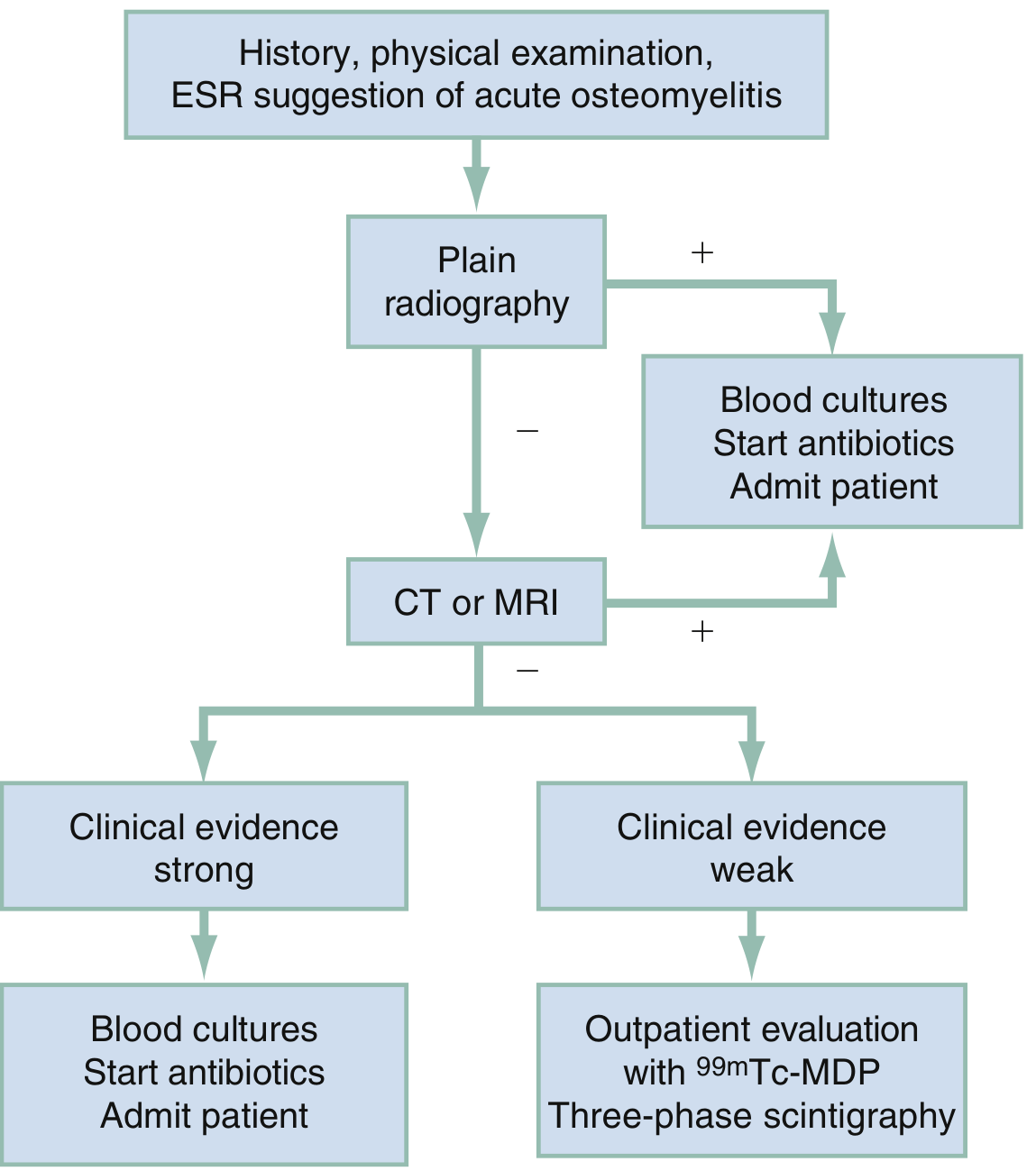
Algorithm for imaging in ED diagnosis of osteomyelitis - Rosen's Emergency Medicine
Treatment
General Principles
- Blood cultures and bone biopsy BEFORE starting antibiotics (whenever possible)
- Empiric antibiotics - cover S. aureus (including MRSA in high-prevalence areas) as first priority
- Surgical drainage when abscess or necrotic bone is present
- Total duration: typically 4-6 weeks for acute; longer for chronic or vertebral
Empiric Antibiotic Selection
| Situation | Empiric Choice |
|---|---|
| Community AHO (low MRSA risk) | Anti-staphylococcal penicillin (oxacillin/nafcillin) or cephalosporin |
| MRSA concern (most AHO now) | Vancomycin IV |
| Gram-negative coverage needed (DM, UTI source, neonate) | Add piperacillin-tazobactam or a carbapenem |
| Sickle cell (Salmonella) | Fluoroquinolone or cephalosporin |
- De-escalate based on culture and sensitivity results
- IV-to-oral switch once clinically improving (oral bioavailability good for many agents)
- Recent evidence supports oritavancin for MRSA osteomyelitis (long-acting lipoglycopeptide) - [2025 meta-analysis, PMID 41224240]
Surgical Indications
- Failure of antibiotics (no improvement in 24-48 hours in children)
- Subperiosteal abscess
- Sequestrum / chronic osteomyelitis
- Spinal cord compression from epidural abscess (emergency)
- Sinus tract formation
Complications
- Chronic osteomyelitis (5-25% of acute cases - risk factors: delayed diagnosis, immunocompromise, extensive necrosis, inadequate treatment)
- Septic arthritis (especially when metaphysis is intracapsular, e.g., proximal femur)
- Pathologic fracture
- Growth disturbance (children - if epiphysis involved)
- Bacteremia and sepsis
- Epidural abscess / spinal cord compression (vertebral)
- Secondary amyloidosis (chronic)
- Squamous cell carcinoma in chronic draining sinus tracts
- Sarcoma developing in chronically infected bone
Robbins & Kumar Basic Pathology, p. 779; ROSEN's Emergency Medicine
Special Types
Brodie Abscess
- Subacute osteomyelitis variant
- Well-defined lytic lesion with a sclerotic rim on imaging
- Usually in metaphysis; most common in adolescents
- Cultures often negative
Chronic Recurrent Multifocal Osteomyelitis (CRMO)
- Autoinflammatory, not infectious
- Multiple skeletal foci, indolent, recurrent episodes
- Culture always negative
- May be associated with psoriatic disease
- Recent 2026 systematic review on treatment ([PMID 41654205])
Mycobacterial Osteomyelitis (Pott's Disease)
- ~1-3% of patients with TB develop osseous infection
- Spine involved in 40% (Pott disease)
- Multi-vertebral involvement, psoas abscess
- Histology: caseating granulomas
- More destructive and treatment-resistant than pyogenic osteomyelitis
- Localized pain, low-grade fever, weight loss
Robbins & Kumar Basic Pathology
Key Points Summary
| Feature | Detail |
|---|---|
| Most common pathogen | S. aureus (MRSA in AHO) |
| Preferred site in children | Metaphysis of long bones |
| Best initial imaging | Plain X-ray (but changes lag 10-14 days) |
| Best diagnostic imaging | MRI |
| X-ray lag period | 10-14 days |
| Classic chronic findings | Sequestrum + Involucrum + Sinus tracts |
| Lab most consistently elevated | CRP (100% in vertebral OM) |
| Treatment backbone | IV antibiotics + surgical debridement when needed |
| Dangerous complication | Epidural abscess in vertebral OM |
Sources:
- Robbins & Kumar Basic Pathology, pp. 779-780
- ROSEN's Emergency Medicine - Concepts and Clinical Practice
- Goldman-Cecil Medicine International Edition
- Grainger & Allison's Diagnostic Radiology
- Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.