Cricopharyngeal myotomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
cricopharyngeal myotomy dysphagia
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough answer:
Cricopharyngeal Myotomy
Anatomy and Rationale
The cricopharyngeus muscle forms the major component of the upper esophageal sphincter (UES). It is a semicircular band of striated muscle arising from the posterior surface of the cricoid cartilage that maintains tonic contraction at rest, relaxing during swallowing to allow passage of a food bolus. When this muscle fails to relax adequately - due to fibrosis, neurological injury, or uncoordinated contraction - it creates a zone of obstruction at the pharyngo-esophageal (PE) junction.
Cricopharyngeal myotomy divides these circular muscle fibres down to the underlying mucosa, reducing resting sphincter pressure and shortening sphincter length, while preserving the peak pharyngeal propulsive pressure on swallowing. Postoperative manometry confirms reduced (but not eliminated) resting cricopharyngeal pressure, which still affords protection against esophagopharyngeal regurgitation. - Schwartz's Principles of Surgery, p. 475
Indications
| Condition | Role of Myotomy |
|---|---|
| Zenker's diverticulum (ZD) | Always performed; omission leads to high recurrence rates |
| Cricopharyngeal dysfunction / achalasia | May be the sole procedure |
| Post-stroke or neurogenic dysphagia | Selective cases with UES dysfunction on manometry |
| Post-laryngectomy (TEP speech) | Prevents spasm causing tracheoesophageal voice failure (~10-12%) |
| Pharyngeal pouch (moderate-large) | Combined with diverticulopexy or diverticulectomy |
For small ZD (<1-2 cm), myotomy alone may be sufficient as the smallest pouches can disappear as mucosa "pouts" with the myotomy. - Fischer's Mastery of Surgery, p. 2814
It is now widely accepted that treating ZD without a cricopharyngeal myotomy carries a high recurrence rate. - Cummings Otolaryngology, p. 1270
Surgical Approaches
1. Open Transcervical Myotomy
Patient positioning: Supine, shoulder roll to extend the neck, head turned to the right to expose the left neck (most ZDs arise posteriorly on the left).
Incision: Either a transverse incision at the level of the cricoid cartilage, or a vertical incision along the anterior border of the sternocleidomastoid (SCM) - the vertical incision is preferred for very large pouches.
Steps:
- Subplatysmal flaps are raised; SCM retracted laterally
- Strap muscles retracted medially; omohyoid may be divided
- Middle thyroid veins ligated; thyroid lobe reflected forward
- Carotid sheath retracted laterally; pharynx/larynx rotated to the right
- Identify and protect the recurrent laryngeal nerve (enters larynx just inferior to the cricothyroid joint)
- Blunt dissection to posterior pharynx; diverticulum identified (aided by endoscopic packing / transillumination / nasogastric tube or bougie within the lumen)
- A 48 Fr Maloney bougie is placed in the esophagus as a guide
- The myotomy is created: division begins at the cricopharyngeus and extends 5-6 cm distally through the full thickness of circular muscle fibres down to mucosa
- The muscle fibres are pushed apart to create at least a 1 cm gap
- Diverticulum is then managed (excision, suspension, or inversion) depending on size
- Scott-Brown's Otorhinolaryngology, p. 864; Fischer's Mastery of Surgery, p. 2816
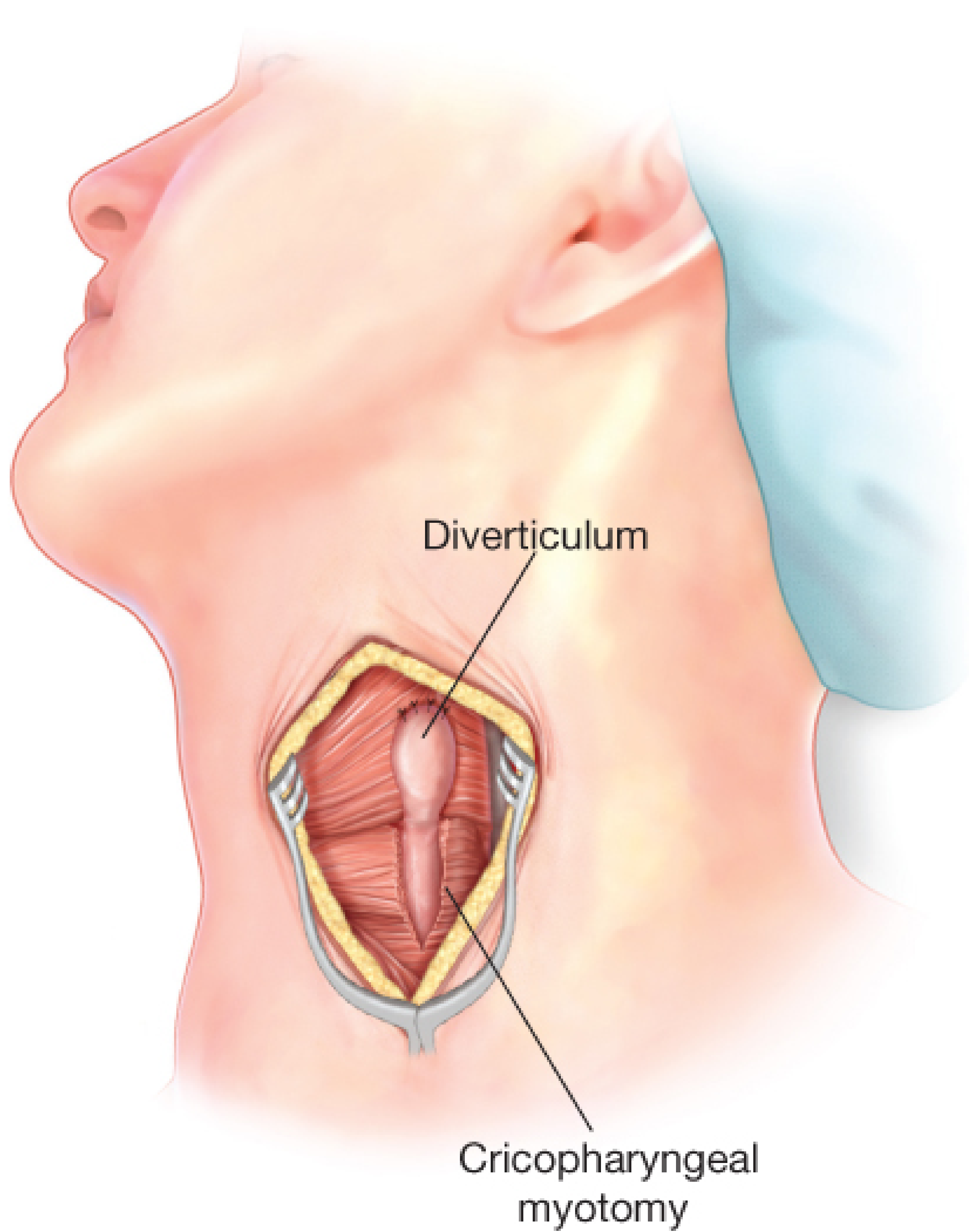
Repair of Zenker diverticulum with suspension diverticulopexy and cricopharyngeal myotomy (Fischer's Mastery of Surgery)
2. Endoscopic Approaches
Transoral stapled diverticulotomy (Dohlman procedure): A Weerda (bivalve) laryngoscope is placed transorally. One blade sits in the esophageal lumen, the other in the diverticulum. An endoscopic linear stapler divides the common septum (which contains the cricopharyngeus) between the two lumens over 30 mm, placing 3 rows of staples on each side. More than one application may be needed for large pouches. - Schwartz's Principles of Surgery, p. 474
- Requires a diverticulum >2-3 cm for adequate stapler placement
- Patients are fed liquids immediately and discharged the next day
- Residual lateral "pouches" may appear on imaging but are rarely symptomatic if the myotomy is complete
Flexible endoscopic myotomy: Uses electrocautery, argon beam, or CO2 laser to divide the bar. NICE-approved but lacks comparative trial data.
Z-POEM (per-oral endoscopic myotomy for Zenker): Reserved for cases with prominent cricopharyngeus but a small diverticulum (pouch not removed).
Myotomy in Post-Laryngectomy Patients (TEP Speech)
A short posterior midline myotomy of 4-5 cm is carried out at the time of laryngectomy, starting just below the TEP site and extending cranially into thyropharyngeus fibres. It divides the circular muscle of the upper esophagus and cricopharyngeus.
Purpose: prevents reflex hypertonicity/spasm of the PE segment when the upper esophagus is distended with air during tracheoesophageal voice, which causes TEP speech failure in 10-12% of patients. A European multicentre audit confirmed that myotomy improved voice outcomes. - Scott-Brown's Otorhinolaryngology, p. 5176-5183
Postoperative Care
- Small drain left in the neck after open surgery
- Barium swallow on postoperative day 1 to confirm no leak
- Liquid diet initiated if swallow study satisfactory
- Dietary advancement over several weeks
- Nasogastric tube placed intraoperatively as a precaution; not left routinely - Fischer's Mastery of Surgery, p. 2817
Complications
| Complication | Notes |
|---|---|
| Fistula / cervical abscess | Reduced by diverticulopexy vs. diverticulectomy |
| Hematoma | |
| Recurrent laryngeal nerve palsy | Identify and protect during dissection |
| Esophageal stenosis | Risk of over-resection of esophageal wall without a bougie |
| Horner's syndrome | Due to sympathetic chain proximity |
| Difficulties in phonation | |
| Incomplete myotomy / residual dysphagia | Insufficient length (<4-5 cm) |
| Recurrence of ZD | More common after diverticulectomy without myotomy |
Schwartz's Principles of Surgery, p. 472
Key Points
- Myotomy length must be at least 4-5 cm - short myotomy is a common cause of failure
- Always performed with ZD surgery - recurrence is significantly higher without it
- Recurrent laryngeal nerve protection is the most important step during open dissection
- Postoperative manometry: peak pharyngeal pressure unchanged; resting UES pressure reduced but not eliminated; sphincter length shortened - Schwartz's Principles of Surgery, p. 475
- A systematic review (PMID 39353299) from 2024 on pediatric cricopharyngeal achalasia confirms myotomy as the definitive management in the pediatric population as well
Balloon Eustachian tube dilatation
Finding Sources
Finding Sources
Searching PubMed
balloon Eustachian tube dilation
Reading File
Reading Article
PMID: 40008607
Reading Article
PMID: 40944547
Reading File
Loading Image
I now have comprehensive, high-quality content from Cummings plus two landmark recent meta-analyses. Here is the full answer:
Balloon Eustachian Tube Dilation (BET / Balloon Eustachian Tuboplasty)
Background and Rationale
The Eustachian tube (ET) has three physiological functions: pressure equalization between the middle ear cleft and the atmosphere, mucociliary clearance of middle ear secretions, and protection of the middle ear from nasopharyngeal secretions and sound pressure. Obstructive ET dysfunction (ETD) occurs when the tube fails to open adequately, causing chronic negative middle ear pressure, otitis media with effusion (OME), tympanic membrane retraction, and ultimately chronic otitis media.
The most common cause is mucosal inflammatory disease (allergy, laryngopharyngeal reflux, sinonasal disease), and clinical evidence indicates that the obstructive pathology in most patients is located within the cartilaginous portion of the ET (approximately 25 mm long), not the bony portion.
Balloon ET dilation is established as a safe and effective method of treating obstructive ETD by mechanisms similar to sinus ostial dilation - mechanically opening and remodelling the cartilaginous lumen. - Cummings Otolaryngology, p. 2519
Anatomy - Critical Concept
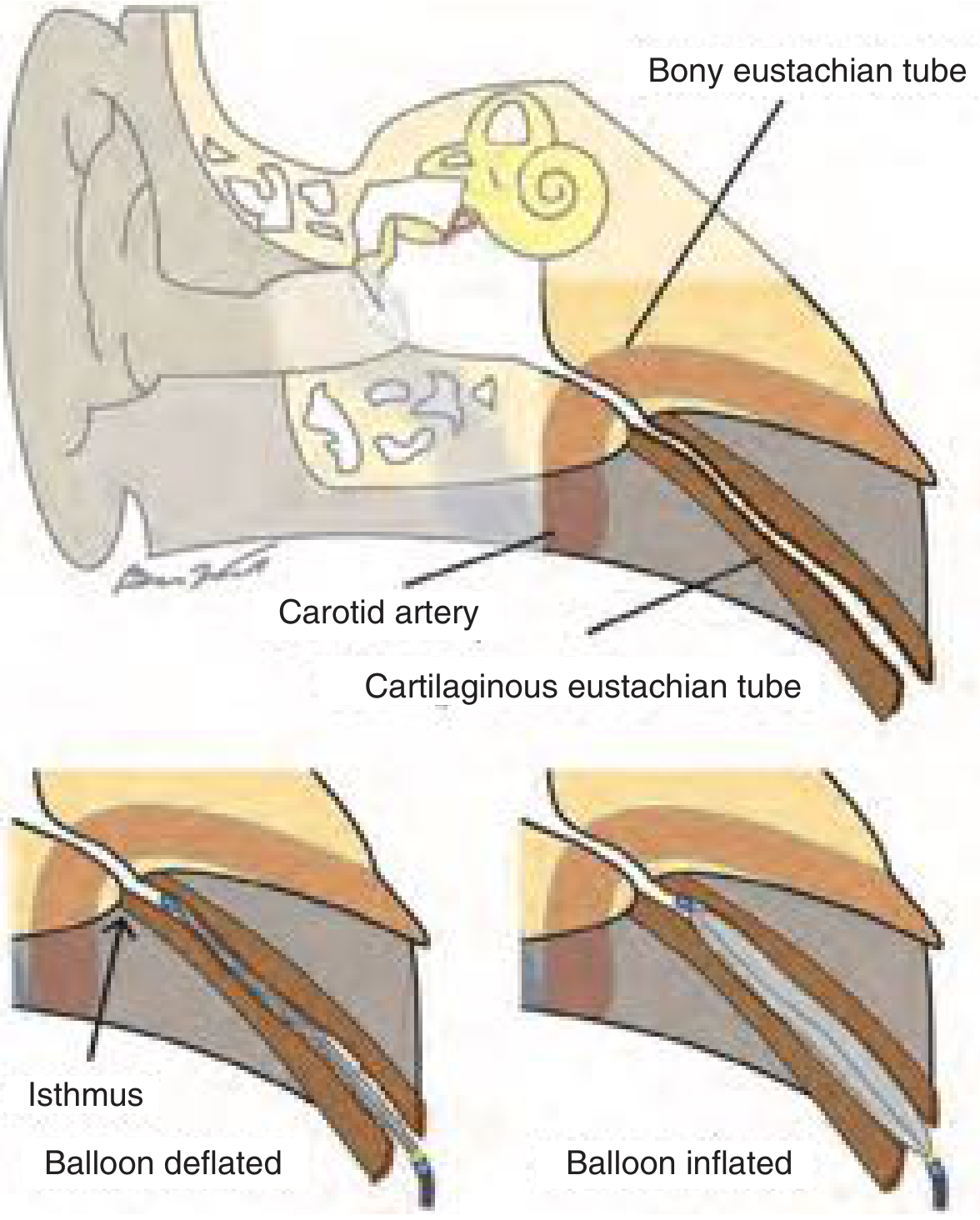
Fig. 131.6 - Balloon dilation addresses only the cartilaginous ET. The balloon must never be advanced beyond the isthmus at the bony-cartilaginous junction. (Cummings Otolaryngology)
The bony ET must never be entered or dilated because:
- It is in close proximity to the internal carotid artery (risk of catastrophic injury if the carotid is dehiscent into the lumen)
- It is unlikely to be the site of obstructive pathology
- FDA-approved balloons are specifically designed not to extend beyond the isthmus
Indications (Box 131.1 - Cummings)
Balloon dilation requires both criteria a and b:
a. ALL of the following:
- Chronic symptoms of obstructive ETD for ≥3 months
- Symptoms persistent despite appropriate directed medical therapy
- Objective pathologic findings on dynamic endoscopic examination of the ET lumen (e.g., inflamed mucosa or lymphoid hyperplasia/cobblestoning compromising tubal opening)
b. AT LEAST ONE of the following:
- Persistent OME or tympanic membrane with negative pressure on insufflation AND type B or C tympanogram
- Consistent history of baro-challenge (e.g., air travel, diving)
- Other objective evidence of obstructive dysfunction
Exclusions / contraindications to consider:
- Patulous ET (BET would worsen symptoms)
- Nasopharyngeal mass (must be excluded by nasopharyngoscopy before any intervention)
- Unilateral effusion in adults requires contrast-enhanced imaging before surgery
Technique
The procedure is performed under endoscopic guidance (generally under general anaesthesia):
- A guide catheter containing the balloon is advanced through the nasal cavity using a 30- or 45-degree angled endoscope
- If the ET lumen is not readily visible, the guide catheter is used to gently reflect the torus tubarius posteriorly and turned upward toward the ear
- The balloon is advanced out of the guide catheter along the anterolateral wall of the cartilaginous ET, coursing tangentially; the cartilaginous skeleton becomes increasingly circumferential superiorly and guides the catheter safely
- The catheter advances until it meets gentle resistance at the isthmus (bony-cartilaginous junction); catheter length is cross-checked to confirm it cannot be within the bony portion
- The balloon is inflated with saline to 10-12 atmospheres for a duration of up to 2 minutes
- A reduced duration may be used for less severe inflammatory pathology to avoid creating a patulous ET
- The guide catheter is braced against the nasal floor to prevent extrusion of the balloon during inflation
- After the allotted time, the balloon is deflated and withdrawn into the guide catheter (to prevent mucosal excoriation on withdrawal)
- The lumen is suctioned and inspected for mucosal injuries
- Procedure repeated on the contralateral side if indicated
- Cummings Otolaryngology, p. 2519-2520
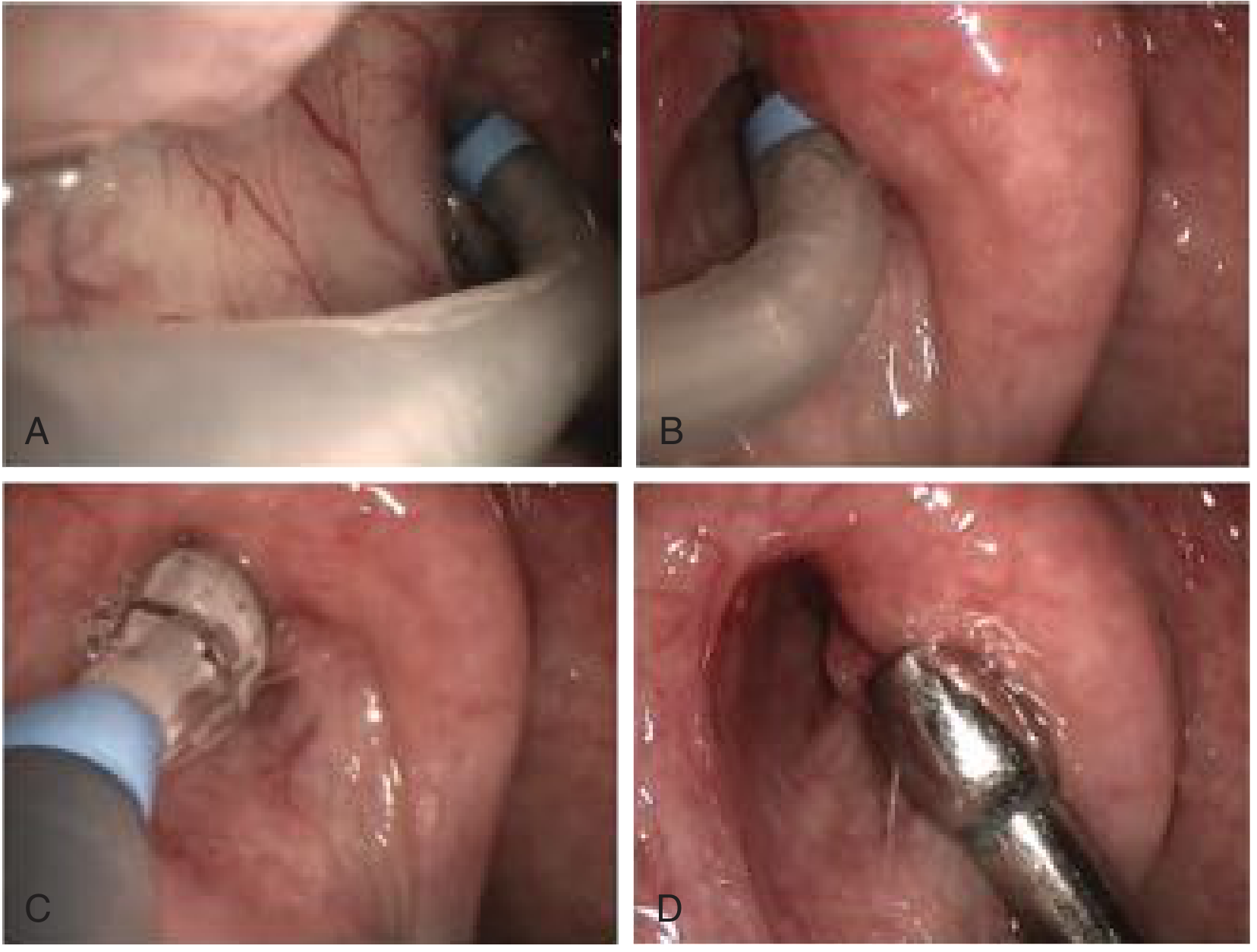
Fig. 131.7 - Intraoperative steps: (A) guide catheter advanced past inferior turbinate, (B) torus tubarius reflected to reveal ET lumen, (C) balloon inflated to 12 atm for 2 minutes, (D) enlarged lumen inspected post-dilation. (Copyright Dennis Poe, MD, PhD - Cummings)
Outcomes
| Measure | Finding |
|---|---|
| Tympanogram normalization | Significant improvement vs. medical therapy alone |
| Ability to perform Valsalva | Statistically significant improvement in retrospective and RCT data |
| Symptom scores (ETDQ-7) | Significant reduction in short-term (to 3 months) |
| Otoscopy | Improvement in TM retraction and effusion clearance |
Evidence note: Multiple retrospective series showed significant improvements in tympanograms, otoscopy, symptom scores, and Valsalva ability. Earlier prospective RCT data (MURET trial) supported efficacy. - Cummings Otolaryngology, p. 2520
Risks and Complications
The procedure is generally very safe. Recognized risks include:
| Risk | Comment |
|---|---|
| Mucosal injury / bleeding | Most common; usually minor |
| False passage creation | Prevented by careful endoscopic guidance along anterolateral wall |
| Patulous ET | Over-dilation; mitigated by reducing balloon inflation duration in less severe disease |
| Carotid artery injury | Catastrophic but rare; avoided by strict adherence to cartilaginous segment only |
| Cervical / mediastinal emphysema | Rare; reported case reports in literature |
| Infection | Rare |
| Failed dilation / residual symptoms | Particularly if mucosal inflammatory disease not controlled medically |
- Cummings Otolaryngology, p. 1993-1997
Current Evidence (2024-2026)
Cochrane Review 2025 (Swords et al., PMID 40008607) - 9 RCTs, 684 participants:
- BET vs. non-surgical treatment at ≤3 months: low-certainty evidence of reduced ETDQ-7 symptoms (MD -1.66, 95% CI -2.16 to -1.16) and improved tympanometry (RR 2.51, 95% CI 1.82-3.48)
- Evidence at 3-12 months was very uncertain
- No studies were rated overall low risk of bias
- Conclusion: BET may provide short-term symptomatic benefit, but long-term high-quality RCT evidence is still needed
Meta-Analysis 2026, Laryngoscope (Raj, Karanth & Poe, PMID 40944547) - 7 RCTs, 315 participants:
- BDET increased the chance of achieving a Type A tympanogram (RR 4.68, 95% CI 2.88-7.51 vs. control)
- When combined with cartilage tympanoplasty for adhesive otitis media: significant air-bone gap closure at 3 months (3.82 dB) and 6 months (4.06 dB)
- Level of Evidence: 1a
Adjunctive Procedures
BET is frequently combined with:
- Tympanostomy tubes - for immediate middle ear ventilation while waiting for long-term ET improvement
- Tympanoplasty (especially cartilage) - evidence shows improved air-bone gap closure
- Medical treatment of underlying inflammatory disease (nasal steroids, antihistamines, PPI for LPR) - should be optimized before and after dilation
- Adenoidectomy in appropriate patients
Key Points Summary
- BET targets only the cartilaginous ET (~25 mm); the bony ET is never dilated due to carotid proximity
- Inflation parameters: 10-12 atm saline, up to 2 minutes
- Pre-procedure dynamic nasopharyngoscopy is mandatory to confirm obstructive pathology and exclude nasopharyngeal mass
- Must exclude patulous ETD before performing BET (it would worsen symptoms)
- The 2025 Cochrane review confirms short-term benefit with low-certainty evidence; a 2026 meta-analysis (Level 1a) confirms significant tympanometric improvement
- Long-term durability and optimal patient selection criteria remain active areas of research
Microdebrider in ENT
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Excellent - I now have comprehensive content from multiple textbooks covering all major ENT applications of the microdebrider. Let me compose the full answer:
Microdebrider in ENT Surgery
What Is a Microdebrider?
The microdebrider (powered tissue shaver / endoscopic debrider) is a motorized cutting-suction instrument that simultaneously resects tissue and aspirates it into a collection system. A rotating or oscillating inner blade inside a hollow outer cannula cuts tissue that is drawn into a side-opening port by continuous suction. The result is precise, controlled tissue removal with immediate clearance of the operative field - without thermal injury to surrounding structures.
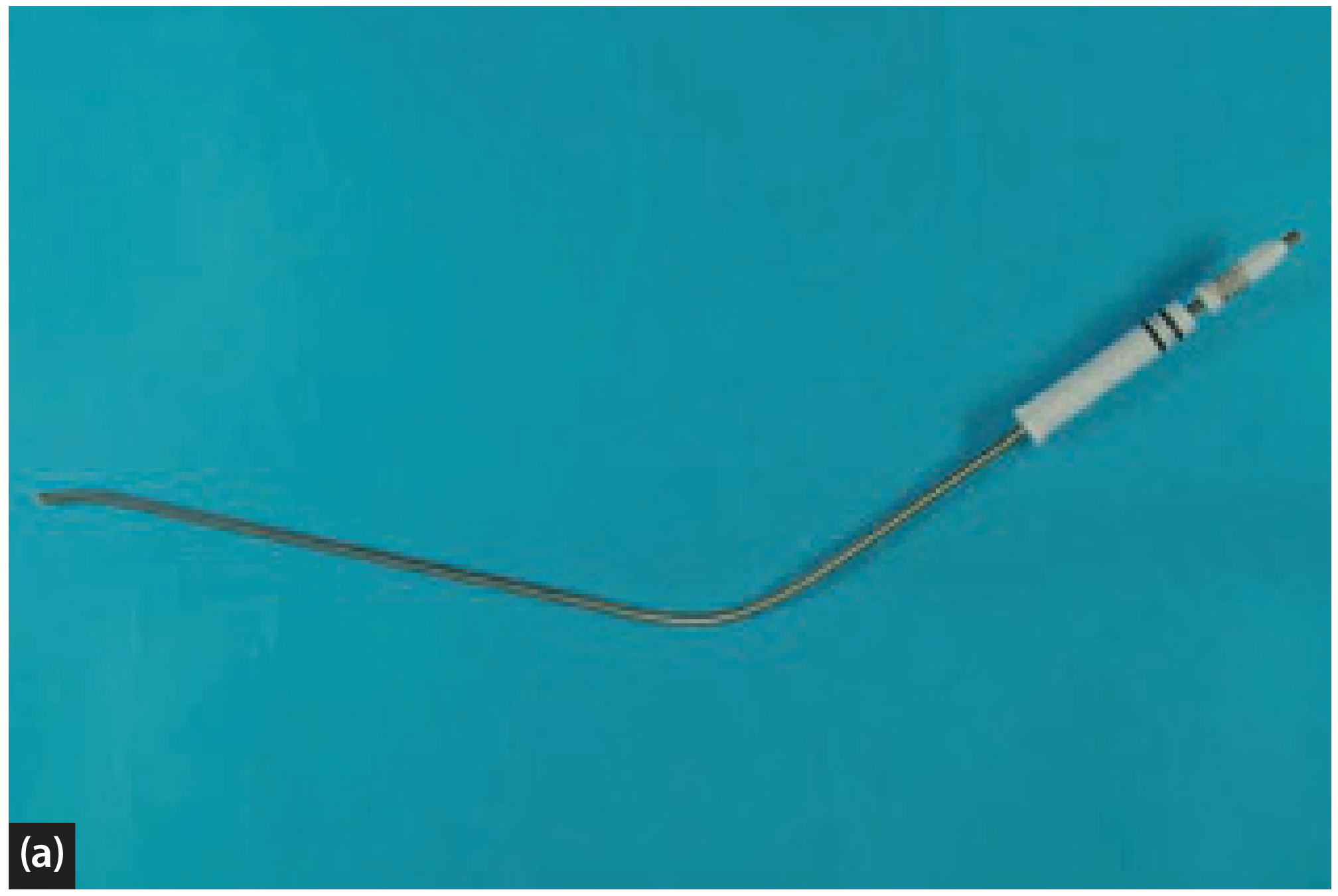
Microdebrider with curved laryngeal blade. (Scott-Brown's Otorhinolaryngology, Vol. 2)
Components and Settings
| Component | Detail |
|---|---|
| Console/motor unit | Controls rotational speed and direction (oscillating or continuous rotation) |
| Handpiece | Connects to blade; may be straight or angled |
| Outer cannula | Rigid, with a side-opening window |
| Inner rotating blade | Non-serrated (mucosa-sparing) or serrated (bone-cutting) variants |
| Suction channel | Integral; connects to a collection system |
| Blade diameters | 2 mm (mini - for turbinate submucosal work), 3.5 mm, 4 mm |
| Speed range | 300-700 rpm for laryngeal/delicate work; up to 4000 rpm for sinus bone |
| Blade angulation | 0°, 40°, 60°, 90° - chosen according to surgical site |
ENT Applications
1. Functional Endoscopic Sinus Surgery (FESS) / Nasal Polypectomy
The microdebrider is particularly helpful in chronic rhinosinusitis with nasal polyposis (CRSwNP):
-
Primary polyp surgery: polyps are gelatinous with minimal blood supply - the microdebrider removes them rapidly with low blood loss
-
Revision polypectomy (scarred, vascular polyps): the instrument significantly reduces blood loss and improves visualization by quickly debulking polyps while simultaneously suctioning blood, keeping the field clear
-
Allows systematic clearance - first anteriorly and inferiorly until landmarks (middle turbinate, orbit, skull base) are identified, then methodical ethmoidectomy
-
Used to remove the inferomedial vertical basal lamella to open the posterior ethmoid in posterior ethmoidectomy
-
Blade angulation can be changed to address frontal recess, sphenoid, or maxillary sinus
-
Cummings Otolaryngology, p. 583, 892
2. Inferior Turbinate Reduction
Two distinct microdebrider approaches are used:
a. Submucosal (mucosal-preserving) technique - preferred:
- A small incision is made at the anterior end of the inferior turbinate
- A submucosal tunnel is created
- A 2 mm oscillating mini-microdebrider blade is introduced submucosally
- The erectile tissue (inferior and medial turbinate) is partially resected from within
- Post-operative nasal packing is not necessary
- All overlying mucosa is preserved, maintaining mucociliary function
- Can be combined with posterior nasal nerve division at the sphenopalatine foramen (FITS - functional inferior turbinosurgery) to also address autonomic control
b. Direct mucosal reduction (destructive technique):
-
Mucosa is debrided down to periosteum along the medial aspect and inferior edge of the anterior two-thirds of the turbinate
-
Bleeding is minimal as long as periosteum is undisturbed
-
Normal mucosa regenerates within 6-12 weeks; mucociliary clearance problems have not been observed
-
Also used in turbinoplasty to remove the lateral mucosal leaf while the medial mucosa is repositioned as a "neoturbinate"
-
Scott-Brown's Otorhinolaryngology Vol. 1, p. 1210-1213
3. Adenoidectomy
-
The microdebrider (along with Coblation and suction coagulator) is a direct-vision technique for adenoidectomy, superior to blind curettage in terms of precision
-
Allows controlled removal under endoscopic view, reducing the risk of velopharyngeal insufficiency
-
In a randomized controlled trial, the microdebrider was 20% faster than the curettage technique
-
Disadvantage: high unit cost compared to suction coagulator
-
Advantage: single-use blades abolish the risk of cross-infection transmission
-
Allows deliberate preservation of adenoid tissue at the inferior nasopharynx where VPI is a risk
-
Scott-Brown's Otorhinolaryngology Vol. 2, p. 6314-6323
4. Powered Intracapsular Tonsillectomy and Adenoidectomy (PITA)
The microdebrider is the instrument of choice for PITA:
-
The bulk of tonsillar tissue is removed while deliberately preserving the tonsillar capsule as a "biologic dressing" over the pharyngeal constrictor musculature
-
Decreased thermal injury to tonsillar fossa musculature
-
Benefits: reduced postoperative pain, decreased analgesic use, and potentially reduced hemorrhage risk compared to monopolar electrocautery tonsillectomy
-
Limitation: risk of tonsillar tissue regrowth and possible re-infection from residual tonsil tissue
-
Both retrospective and small prospective studies confirm significantly less postoperative pain and decreased analgesic use vs. monopolar electrocautery
-
Cummings Otolaryngology, p. 3525
5. Laryngeal Papillomatosis (Recurrent Respiratory Papillomatosis - RRP)
The powered microdebrider has become the gold standard for laryngeal papilloma removal, particularly in juvenile-onset RRP (JORRP):
-
A non-serrated laryngeal blade is used at 300-700 rpm - low speed allows papillomas to be suctioned into the debrider with minimal cutting trauma to surrounding normal laryngeal tissues
-
No thermal trauma (unlike CO2 laser)
-
Under direct microlaryngoscopic control, it is extremely precise with minimal mucosal damage
-
The laryngeal blade geometry allows gentle but comprehensive removal with minimal contamination of the lower respiratory tract with blood or papilloma fragments
-
Compared with CO2 laser: retrospective studies show good disease clearance, shorter procedure time, less post-operative pain, and no incidence of delayed soft-tissue complications (vocal fold fibrosis, interarytenoid fibrosis)
-
CO2 laser remains preferred by some surgeons for hemostasis in highly vascular disease; the microdebrider is advantageous in children and for frequent debridements
-
Scott-Brown's Otorhinolaryngology Vol. 2, p. 3037-3055
6. Central Airway / Tracheobronchial Disease
- Used endoscopically via rigid bronchoscope for debulking of endobronchial tumours and managing airway obstruction from laryngotracheal carcinoma
- Allows tissue removal under direct vision with simultaneous suction, maintaining a clear airway
- Listed alongside laser, argon plasma coagulation, and cryotherapy as a tool for managing central airway disorders
- Murray & Nadel's Respiratory Medicine; Cummings Otolaryngology
Advantages of the Microdebrider
| Advantage | Mechanism |
|---|---|
| No thermal injury | Purely mechanical cutting - no heat generated at the blade tip |
| Simultaneous suction | Clears blood and debris instantly, maintaining visualization |
| Mucosal preservation | Tissue drawn into the port only if directly applied; surrounding mucosa largely spared |
| Precise, controlled resection | Suction pulls tissue into the blade window - surgeon controls what is removed |
| Faster operative time | Simultaneous cutting and evacuation vs. separate steps |
| Versatile blade selection | Straight, angled, serrated, non-serrated; sizes from 2-4 mm |
| Single-use blades | Eliminates prion/infection transmission risk |
Disadvantages and Limitations
| Disadvantage | Notes |
|---|---|
| High unit cost | Console + disposable blades are expensive; limits use to higher-volume centres |
| No intrinsic haemostasis | Unlike laser or electrocautery; active bleeding requires separate management |
| Tissue destruction is irreversible | Must be used with precision; once mucosa is removed it cannot be replaced |
| Risk of patulous ET / over-resection | In turbinate/ET work, excessive removal causes long-term problems |
| Requires endoscopic skill | Blind use risks injury to orbit, skull base, or carotid artery |
| Blade fouling | Can become blocked with thick/inspissated secretions |
Safety Considerations
- In FESS: always identify the lamina papyracea (orbital wall) and skull base before using the microdebrider - inadvertent application can cause orbital fat herniation, CSF leak, or intracranial penetration
- In turbinate surgery: restrict to mucosal-preserving submucosal technique when concurrent FESS is performed; reserve direct mucosal debridement for gross hypertrophy
- In laryngeal work: work at low rpm (300-700) with a non-serrated blade to avoid injury to true vocal fold mucosa; do not apply over the anterior commissure without careful judgment to avoid webbing
- In adenoidectomy: maintain endoscopic vision to preserve a cuff of adenoid tissue inferiorly near the ET orifice and velopharyngeal port
Summary of Blade Types by Application
| Application | Blade Type | Speed |
|---|---|---|
| FESS / polypectomy | Straight 3.5-4 mm, serrated for bone | Medium-high (1500-4000 rpm) |
| Inferior turbinate | 2 mm mini, non-serrated | Medium |
| Tonsillectomy (PITA) | 3.5-4 mm, serrated | Medium-high |
| Adenoidectomy | Standard straight/angled | Medium |
| Laryngeal papilloma | Curved non-serrated laryngeal blade | Low (300-700 rpm) |
| Endobronchial tumour | Rigid bronchoscopic blade | Variable |
Endoscopic versus microscopic ear surgeries
Finding Sources
Finding Sources
Searching PubMed
endoscopic versus microscopic ear surgery
Reading File
Reading File
Reading File
Reading Article
PMID: 38415937
Reading Article
PMID: 39749405
Reading File
Reading Article
PMID: 40077841
Loading Image
I now have comprehensive content from multiple textbooks and four high-quality recent systematic reviews/meta-analyses. Let me compile the full answer:
Endoscopic vs. Microscopic Ear Surgery
Historical Context
The operating microscope has been the mainstay of otology since the 1950s, providing surgeons with illuminated, magnified, binocular stereoptic vision of the middle ear through the ear canal or post-auricular approach. Endoscopes were first used in the ear for inspection only, particularly to visualize hidden recesses after microscopic dissection. However, improvements in camera and optical technology have yielded high-definition, wide-angle endoscopes that now allow endoscopes to be used for the entire surgical dissection - giving rise to Endoscopic Ear Surgery (EES) and, in its fullest form, Totally Endoscopic Ear Surgery (TEES). - Cummings Otolaryngology, p. 2753
Fundamental Differences
| Feature | Endoscopic Ear Surgery (EES) | Microscopic Ear Surgery (MES) |
|---|---|---|
| Visualization | Wide-angle, panoramic; angled scopes "look around corners" | Line-of-sight only; limited to structures in direct axial view |
| Binocularity | Monocular (2D image) | Binocular (true 3D stereoscopic depth perception) |
| Both hands | One hand holds endoscope; only ONE hand free for dissection | Both hands free for simultaneous dissection and suction |
| Illumination | Co-axial, intense - follows the line of view | External; shadows may form in deep recesses |
| Hidden recesses | Excellent access (sinus tympani, hypotympanum, protympanum, anterior epitympanum) | Blind spots exist; many areas inaccessible without mastoidectomy |
| Incision | Transcanal (no external incision in TEES) | Post-auricular or endaural incision often required |
| Mastoidectomy | Usually avoided for confined disease | Often required for adequate exposure |
| Magnification | High and variable (move endoscope closer) | Fixed by objective lens; requires adjusting microscope |
| Learning curve | Significant - one-handed technique is challenging | Established; widely taught |
| Equipment | Endoscope + camera tower (high cost) | Operating microscope (established in most theatres) |
The Endoscope in Middle Ear Surgery
Key Anatomical Advantage
The endoscope's chief advantage is visualizing the hidden recesses of the middle ear that the microscope simply cannot see due to line-of-sight constraints:
- Sinus tympani - the most common site of cholesteatoma recurrence; depth and variants clearly seen with angled endoscopes; previously required blind or mastoidectomy-based approaches
- Retrotympanum - many anatomic variations; clearly visualized endoscopically
- Hypotympanum - inferior to the tympanic annulus
- Protympanum - anterior region containing the bony ET
- Anterior epitympanum / supratubal recess - behind the tensor fold
- Epitympanic diaphragm and tympanic isthmus - middle ear ventilation pathways
Endoscopic visualization has also enabled improved in-vivo anatomic understanding of the myriad ossicular ligaments, membranous folds, and ventilation pathways - knowledge that was previously only obtainable from sectioned cadaveric specimens. - Cummings Otolaryngology, p. 4136-4138
Fig. 20-1: Transtympanic endoscopic view of the middle ear; 1.9-mm, 0-degree Hopkins rod endoscope. (Shambaugh Surgery of the Ear)
Endoscopes Used in Ear Surgery
| Parameter | Detail |
|---|---|
| Diameter | 1.9 mm (transtympanic), 2.7 mm, 3 mm, 4 mm |
| Length | 11 cm (standard otology length) |
| Angle | 0° (straight), 30° (most useful), 45°, 70° |
| Camera | CCD/HD camera attached; image on monitor |
| Light source | 150W or 300W xenon/LED |
Caloric effect warning: With a 300W light source, the endoscope left in situ >45-60 seconds can generate temperatures up to 50°C and cause heat-induced caloric vertigo. The 150W source avoids this. Endoscope must be periodically withdrawn or brightness reduced. - Shambaugh Surgery of the Ear, p. 457-476
Surgical Technique - Key Principles of EES
- Transcanal approach: speculum slightly smaller than used with microscope inserted into the EAC to protect canal skin
- Endoscope held in the non-dominant hand; only one instrument in the dominant hand at a time
- Tympanomeatal flap elevated under endoscopic view
- 0° scope for general survey; 30° scope for viewing beneath overhangs and into superior/posterior recesses
- Camera properly oriented on the monitor before instruments are passed (disorientation from camera rotation causes trauma)
- Hemostasis is critical - even minor bleeding obscures the lens; epinephrine-soaked pledgets, bipolar cautery used meticulously
- The endoscope is withdrawn and reinserted with the view angle pre-rotated whenever a significant direction change is required
- At conclusion, myringotomy margins inspected (under microscope if needed) to confirm minimal trauma
Applications: Procedure-by-Procedure Comparison
1. Tympanoplasty
Endoscopic: Transcanal, no post-auricular incision; excellent middle ear visualization for graft placement; typically underlay fascia/cartilage technique.
Microscopic: Post-auricular or endaural; binocular view; both hands free for overlay or underlay graft.
Evidence (2024 Meta-Analysis - Gkrinia et al., PMID 38415937) - 33 studies, 2,646 patients:
- Graft success rate: comparable between techniques (no significant difference)
- Air-bone gap improvement: equivalent
- Endoscopic significantly better for: postoperative wound infection, dysgeusia (chorda tympani preservation), otitis externa, auricular numbness, and surgical duration
- Endoscopic benefits are greatest vs. the post-auricular microscopic approach (vs. transcanal microscopic, differences are smaller)
2. Stapedotomy (Otosclerosis)
Endoscopic: Single-handed technique; avoids chorda tympani manipulation as the wide-angle view allows the footplate to be approached without displacing the nerve.
Microscopic: Binocular depth perception aids prosthesis placement onto the footplate.
Evidence (2025 Meta-Analysis of RCTs - Albazee et al., PMID 39749405) - 11 RCTs, 515 patients:
- Surgical duration: no significant difference
- Air-bone gap improvement: equivalent (MD 1.04 dB, not significant)
- Endoscopic significantly better for:
- Less chorda tympani nerve manipulation (RR 0.58)
- Less dysgeusia (RR 0.33 - 67% reduction)
- Less postoperative pain (SMD -1.59)
- CTN injury, facial nerve injury, TM perforation, dizziness: no significant difference
3. Cholesteatoma Surgery (TEES vs. Microscopic)
Endoscopic: Transcanal dissection; angled scopes directly visualize sinus tympani, retrotympanum, and epitympanic recesses without mastoidectomy; disease-limiting step is extension posterior to the dome of the lateral semicircular canal (requires mastoidectomy if exceeded).
Microscopic: Canal wall-up (CWU) or canal wall-down (CWD) with mastoidectomy; gold standard for extensive disease; two-handed dissection; residual cholesteatoma in the sinus tympani is a known limitation.
Evidence (2025 Meta-Analysis - Giffoni et al., PMID 40077841) - 13 studies, 1,134 cases:
- Residual cholesteatoma: significantly LESS with endoscopic approach (RR 0.65; 95% CI 0.47-0.89) - 35% relative risk reduction
- TM perforation and graft displacement: no significant difference
- Postoperative taste disturbance, transient vertigo: no significant difference
- TEES does not yet demonstrate a significant improvement in recurrence rates (residual vs. recurrence distinction is important)
Key limiting rule for TEES: Cholesteatoma extending posteriorly beyond the dome of the lateral semicircular canal into the mastoid requires mastoidectomy and microscopic visualization. - Cummings Otolaryngology, p. 4145
4. Ossiculoplasty
- Endoscopic approach provides excellent visualization of the oval window, round window, and stapes superstructure
- Prosthesis placement is technically demanding with one hand; many surgeons use a combined approach
- Hearing results assumed comparable to microscope-guided ossiculoplasty - Cummings Otolaryngology (cholesteatoma chapter), p. 82
5. Myringotomy / Grommets
- EES transcanal approach is fast and avoids speculum ear-stretching
- Endoscope allows clear visualization of the anterosuperior quadrant which is a common blind spot under the microscope
Advantages and Limitations Summary
Advantages of Endoscopic Ear Surgery
| Advantage | Clinical Significance |
|---|---|
| Visualizes hidden recesses | Reduces residual cholesteatoma; identifies disease not visible microscopically |
| No external incision (TEES) | Reduced morbidity, wound complications, auricular numbness, hyperesthesia |
| Co-axial illumination | No shadows; excellent view in deep, narrow canals |
| Angled scopes (30°, 45°, 70°) | Access beneath ossicular overhangs, into sinus tympani and epitympanum |
| Shorter operative time | Shown for tympanoplasty; avoids mastoidectomy set-up time |
| Less chorda tympani disturbance | Significantly less dysgeusia (tympanoplasty and stapedotomy data) |
| Less post-op pain | Shown for stapedotomy and tympanoplasty |
| Reduced hospital stay | Earlier discharge; return to activities sooner |
| Children/parents prefer it | "No incision" is highly valued in pediatric practice |
Limitations of Endoscopic Ear Surgery
| Limitation | Impact |
|---|---|
| One-handed technique | No simultaneous suction-dissection; requires alternating instruments and endoscope |
| No depth perception (monocular) | Tactile feedback important; risk of orientation errors |
| Lens contamination with blood | Any bleeding obscures the view completely; meticulous haemostasis mandatory |
| Thermal risk | Light source >150W generates heat; caloric vertigo if left in situ; theoretical risk of thermal injury |
| Cannot address mastoid disease | Cholesteatoma beyond lateral SCC requires conversion to microscopic mastoidectomy |
| Learning curve | Significant - one-handed dissection and monitor-based orientation require dedicated training |
| Equipment cost | Endoscopy tower, HD cameras, angled Hopkins rod scopes represent additional investment |
| Limited two-handed manoeuvres | Placing prostheses, suturing grafts, and manipulating ossicles is harder with one hand |
The Combined (Hybrid) Approach
In current practice, endoscopy and microscopy are complementary, not competing:
- Microscope for dissection + endoscope for inspection: The endoscope is used after microscopic removal to inspect hidden recesses (especially sinus tympani) for residual cholesteatoma - this alone has been shown to reduce residual disease rates
- Endoscope for middle ear + microscope for mastoid: TEES for the tympanic portion of cholesteatoma, then mastoidectomy under microscope if needed
- Endoscope to plan approach: Pre-dissection endoscopic survey guides whether TEES alone is feasible based on disease extent on CT and intraoperative findings
Current Consensus
- EES is no longer "promising" - it is a well-established technique with a solid evidence base
- For tympanoplasty: comparable graft success with fewer wound complications and shorter operative time endoscopically
- For stapedotomy: equivalent audiometric outcomes, but endoscopic approach significantly reduces chorda tympani disturbance and dysgeusia
- For cholesteatoma: endoscopic approach significantly reduces residual disease (35% RR reduction); TEES is the preferred approach for disease confined to the middle ear
- The microscope remains indispensable for extensive disease, mastoid surgery, and where two-handed technique is required
- Most modern otology units adopt a context-dependent hybrid strategy based on preoperative CT, disease extent, and surgeon expertise
This is a shared conversation. Sign in to Orris to start your own chat.