Tab Amitriptyline
Reading File
Finding Sources
Finding Sources
Searching PubMed
amitriptyline clinical use efficacy
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it:
Tablet Amitriptyline
Class: Tricyclic Antidepressant (TCA) - Tertiary amine
Mechanism of Action
Amitriptyline works through multiple receptor targets:
- Reuptake inhibition - Blocks both the serotonin transporter (SERT) and norepinephrine transporter (NET), increasing synaptic concentrations of both neurotransmitters.
- Receptor blockade - Has strong binding affinity at:
- Muscarinic (M1) receptors - anticholinergic effects
- Histamine (H1) receptors - sedation
- Alpha-adrenergic (α1) receptors - orthostatic hypotension
- Postsynaptic 5-HT2a receptors
Amitriptyline is a tertiary amine; it is demethylated in the body to its active metabolite nortriptyline (a secondary amine). Both are pharmacologically active and contribute to its effects.
- Lippincott Illustrated Reviews: Pharmacology, p. 591
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 9553
Indications & Clinical Uses
| Indication | Notes |
|---|---|
| Major depressive disorder | FDA-approved; improves mood in 50-70% of patients. Onset 2+ weeks |
| Neuropathic pain | First-line agent; NNT ~2.5; dose 25-150 mg/day (lower than for depression), effect within 2 weeks |
| Migraine prophylaxis | Particularly effective; widely used for prevention |
| Fibromyalgia | First-line per AWMF guidelines; low doses (10-25 mg) help pain, sleep, and fatigue |
| Chronic pain syndromes | Back pain, gastrointestinal pain, idiopathic pain, tinnitus (60+ RCTs) |
| Panic disorder | Off-label; TCAs were among first drugs shown effective |
| IC/BPS (Interstitial Cystitis) | Used for bladder pain syndrome |
| Insomnia | Low-dose at bedtime, off-label |
Key insight: In pain syndromes, the analgesic effect appears independent of the antidepressant effect - the doses are lower, the onset is faster, and the mechanism is distinct. The NNT in pain (1 in 3 patients benefit) is actually better than in depression (1 in 6).
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 9553-9554
- Lippincott Illustrated Reviews: Pharmacology, p. 591
Dosing
Adult Dosing
| Indication | Starting Dose | Range |
|---|---|---|
| Depression | 25-75 mg at bedtime | Up to 150-300 mg/day |
| Neuropathic pain | 10-25 mg at night | 25-150 mg/day (median 75 mg) |
| Migraine prophylaxis | 10-25 mg QHS | 10-400 mg/24 hr |
| Fibromyalgia | 10 mg at bedtime | Up to 50 mg |
Pediatric Dosing (Harriet Lane)
| Indication | Dose |
|---|---|
| Chronic pain augmentation | Initial 0.1 mg/kg QHS, increase over 2-3 weeks to 0.5-2 mg/kg QHS |
| Migraine prophylaxis | Initial 0.1-0.25 mg/kg QHS; titrate every 2 weeks up to 2 mg/kg/day or 75 mg/day max |
For pediatric doses >1 mg/kg/24 hr: divide BID and monitor ECG.
- Harriet Lane Handbook, 23rd ed., p. 1012-1013
Pharmacokinetics
| Parameter | Value |
|---|---|
| Peak plasma | 1-12 hours |
| Half-life | ~25 hours (range 9-28 hours) |
| Metabolism | Hepatic - CYP1A2, 2C9, 2C19, 2D6 (primary), 3A3/4 |
| Inhibitor of | CYP1A2, 2C9, 2C19, 2D6, 2E1 |
| Therapeutic level | Sum of amitriptyline + nortriptyline: 100-250 ng/mL |
| Dosing | Usually QHS (bedtime) due to sedation; manufacturer recommends BID with highest dose at night |
| Bioavailability | Low and variable (extensive first-pass metabolism) |
Serum level monitoring: Obtain sample ≥8 hours after an oral dose, after 4-5 days of continuous dosing.
Sex differences: Women have higher plasma levels and lower clearance rates than men, especially with increasing age - primarily due to lower CYP2D6 activity.
- Maudsley Deprescribing Guidelines, p. 324
- Harriet Lane Handbook, 23rd ed., p. 1012
Pharmacogenomics (CYP2D6/2C19)
| CYP2D6 | CYP2C19 Normal | CYP2C19 Poor Metabolizer |
|---|---|---|
| Ultra-rapid metabolizer | Avoid; if necessary, titrate to higher dose | Avoid; use alternative |
| Normal metabolizer | Use recommended starting dose | Avoid; if necessary, 50% dose reduction |
| Intermediate metabolizer | 25% initial dose reduction | Avoid; use alternative |
| Poor metabolizer | Avoid; if necessary, 50% dose reduction | Avoid; use alternative |
- Harriet Lane Handbook, 23rd ed., p. 1012
Adverse Effects

Anticholinergic (M1 blockade):
- Dry mouth, blurred vision, constipation, urinary retention
- Sinus tachycardia, aggravation of narrow-angle glaucoma
Cardiovascular (α1 blockade + quinidine-like):
- Orthostatic hypotension, dizziness, reflex tachycardia
- Cardiac conduction changes (quinidine-like effect)
- Risk of life-threatening arrhythmias in overdose
CNS/Metabolic (H1 blockade):
- Sedation (prominent - use QHS dosing)
- Weight gain
- May precipitate mania in bipolar disorder
Other:
- Sexual dysfunction (less than SSRIs)
- Liver enzyme elevation
- Urine discoloration (blue/green)
- Lower seizure threshold
ECG monitoring: Decrease dose if PR interval reaches 0.22 sec, QRS reaches 130% of baseline, HR >140/min, or BP >140/90.
- Lippincott Illustrated Reviews: Pharmacology, p. 592-593
Contraindications
- Recent MAOI use (within 14 days) - risk of serotonin syndrome / hypertensive crisis
- Narrow-angle glaucoma
- Seizure disorders
- Severe cardiac disease / arrhythmias
- Acute post-myocardial infarction recovery
- Bipolar disorder (may precipitate manic switch - use with caution)
- Benign prostatic hyperplasia (exacerbation risk)
Drug Interactions
- MAOIs - Absolutely contraindicated (hypertensive crisis, serotonin syndrome)
- CNS depressants - Additive sedation
- Rifampin - Decreases amitriptyline levels
- Tramadol - Increased side effects
- CYP2D6 inhibitors (fluoxetine, paroxetine, bupropion) - Increase amitriptyline levels
- Anticholinergic drugs - Additive anticholinergic toxicity
- Antihypertensives - Enhanced hypotensive effects
- Quinidine / antiarrhythmics - Additive cardiac conduction effects
Overdose / Toxicity
TCAs have a narrow therapeutic index - 5 to 6x the maximal daily dose of a TCA can be lethal. Key features of TCA toxicity (the "3 C's"):
- Coma (CNS depression)
- Convulsions
- Cardiac arrhythmias (wide QRS, ventricular tachycardia)
Sodium bicarbonate is the treatment of choice for TCA-induced cardiac toxicity (to overcome sodium channel blockade and correct acidosis).
Discontinuation / Tapering
Amitriptyline is in a high-risk category for withdrawal effects. In one placebo-controlled study, 80% of patients experienced withdrawal when tapered over 6 months. Key principles:
-
Do not abruptly stop, especially after high doses for prolonged periods
-
Dose-effect relationship is hyperbolic (not linear): linear reductions cause progressively larger pharmacological effect changes
-
Three taper speed options (Maudsley):
- Fast (10 steps, 5-10 months): 100 → 50 → 25 → 12.5 → 7.5 → 5 → 3 → 1.6 → 0.8 → 0 mg
- Moderate (20 steps, 10-20 months)
- Slow (40 steps, 20-40 months)
-
Switch to liquid formulation (2 mg/mL) for doses below 5 mg
-
Every-other-day dosing is NOT recommended for tapering
-
Maudsley Deprescribing Guidelines, p. 324-327
Available Formulations
- Tablets: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg
- Sustained-release capsules
- Oral liquid (2 mg/mL) - useful for fine tapering
Trade names: Elavil, Endep
Recent Evidence (2024-2026)
A 2024 systematic review with network meta-analysis confirmed amitriptyline remains relevant among preventive drug treatments for chronic migraine. A 2025 network meta-analysis in the British Journal of Psychiatry examined antidepressant efficacy and tolerability in patients with comorbid physical conditions and depressive disorders - relevant given amitriptyline's dual use in pain and depression.
Can propranolol be used in migraine
Reading File
Finding Sources
Finding Sources
Searching PubMed
propranolol migraine prevention
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer.
Propranolol in Migraine
Yes - propranolol is FDA-approved for migraine prophylaxis and is one of the most widely used first-line preventive agents. It is not used to treat acute attacks.
Regulatory Status & Guideline Recommendation
Propranolol has first-line recommendation status for migraine prophylaxis across all major guidelines including:
- American Academy of Neurology (AAN) / American Headache Society (AHS)
- Canadian Headache Society
- European Federation of Neurological Societies (EFNS)
Along with topiramate, divalproex, and metoprolol, propranolol is considered a cornerstone of preventive therapy.
- Bradley and Daroff's Neurology in Clinical Practice, p. 439
Why Propranolol (and Not All Beta-Blockers)?
This is an important distinction. Not all beta-blockers work for migraine. The key pharmacological trait that separates effective from ineffective agents is:
Pure beta-adrenergic antagonism WITHOUT intrinsic sympathomimetic activity (ISA)
Beta-blockers with ISA (e.g., acebutolol, oxprenolol, alprenolol) are not effective in migraine. Those without ISA - propranolol, timolol, nadolol, atenolol, metoprolol - work.
Additionally, propranolol's high lipophilicity allows it to cross the blood-brain barrier and penetrate the CNS, which is thought to be an important factor in its efficacy.
- Lippincott Illustrated Reviews: Pharmacology, p. 267
- Cummings Otolaryngology, p. 3231
Mechanism of Action in Migraine
The exact mechanism is unknown. Proposed mechanisms include:
-
Central CNS effects (via blood-brain barrier penetration)
-
Reduction in cortical spreading depression
-
Modulation of serotonergic pathways
-
Decreased sympathetic outflow
-
Reduction in activity of catecholamine-sensitive pathways
-
Katzung's Basic & Clinical Pharmacology, 16th ed.
Efficacy
-
50-70% of patients with migraine derive benefit from prophylactic propranolol
-
Reduces headache frequency and intensity (not an acute abortive)
-
Benefits may also extend to vestibular migraine symptoms (vertigo/dizziness)
-
Full benefit may take up to 6 months to be realized; trials should last at least 2-3 months before declaring failure
-
Cummings Otolaryngology, p. 3231
-
Bradley and Daroff's Neurology in Clinical Practice, p. 435
Dosing
| Formulation | Dose Range |
|---|---|
| Standard oral propranolol | 80-240 mg/day |
| Long-acting (LA/ER) - preferred for compliance | Once daily dosing |
| Starting dose | Low (e.g., 40 mg/day), titrate up |
- Titrate gradually to minimum effective or maximum tolerated dose
- Maintain for at least 3 months; continue for 6-12 months if there is a beneficial response
- Discuss discontinuation after 6 months in well-controlled patients
Adverse Effects
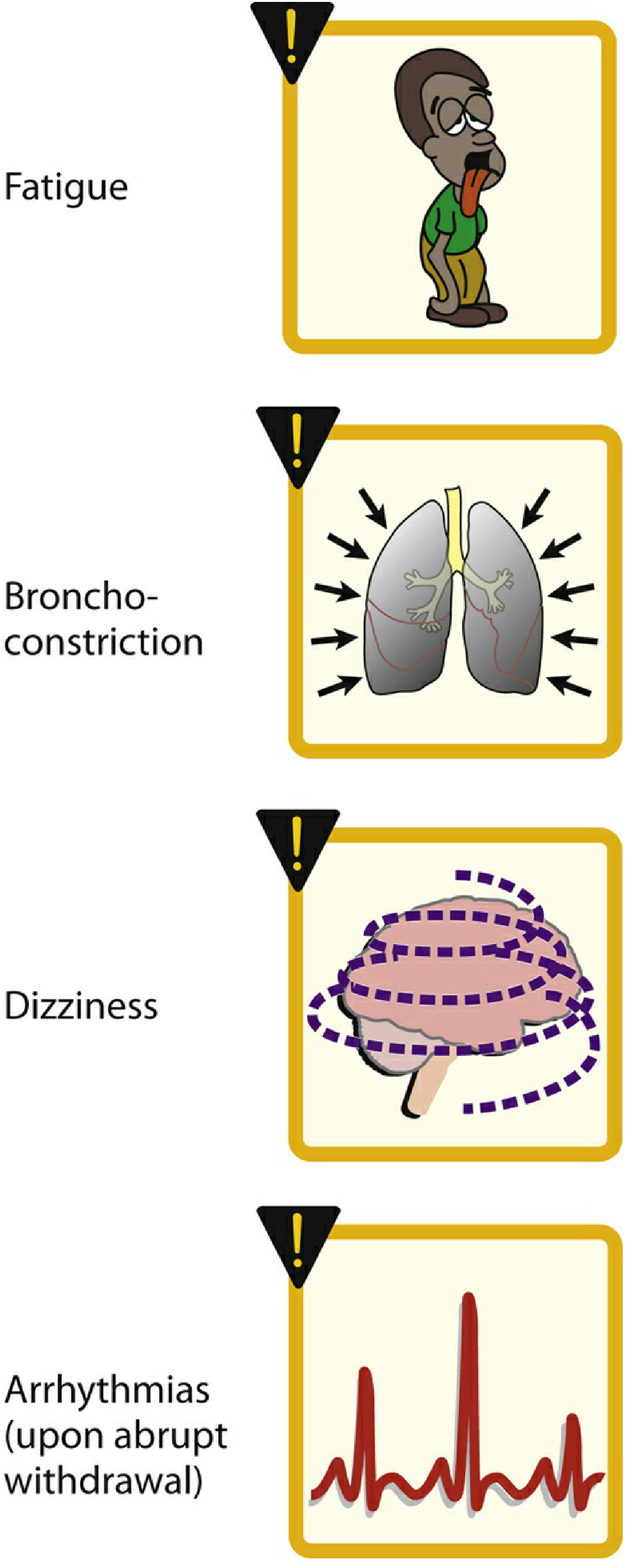
| Side Effect | Notes |
|---|---|
| Fatigue / lethargy | Common; may necessitate discontinuation |
| Bronchoconstriction | Beta-2 blockade; potentially fatal in asthma |
| Dizziness / orthostatic hypotension | Especially on rising |
| Bradycardia | Heart rate monitoring needed |
| Depression | May worsen pre-existing depression |
| Impotence | Sexual dysfunction |
| Insomnia / nightmares | CNS penetration |
| Hypoglycemia masking | Blunts adrenergic signs of hypoglycemia |
| Arrhythmia on abrupt withdrawal | Always taper slowly |
Side effects are generally minimized by slowly increasing the dose from a low starting level.
Contraindications
| Contraindication | Reason |
|---|---|
| Bronchial asthma / COPD | Potentially fatal bronchoconstriction (β2 blockade) |
| Congestive heart failure | Negative inotropy |
| Peripheral vascular disease | Worsens limb ischemia |
| Severe depression | May worsen |
| Diabetes on insulin/oral hypoglycemics | Masks hypoglycemia symptoms |
| Hypothyroidism | Caution |
| Sick sinus syndrome / heart block | Bradycardia risk |
Which Beta-Blockers Work for Migraine?
| Drug | Effective for Migraine | Has ISA |
|---|---|---|
| Propranolol | ✅ Yes (FDA-approved) | No |
| Timolol | ✅ Yes (FDA-approved) | No |
| Metoprolol | ✅ Yes | No |
| Nadolol | ✅ Yes | No |
| Atenolol | ✅ Yes | No |
| Acebutolol | ❌ No | Yes |
| Oxprenolol | ❌ No | Yes |
| Alprenolol | ❌ No | Yes |
- Cummings Otolaryngology, p. 3231; Bradley and Daroff's Neurology, p. 441
Propranolol vs. Acute Migraine Therapy
| Aspect | Propranolol | Triptans (e.g., sumatriptan) |
|---|---|---|
| Role | Prophylaxis only | Acute/abortive |
| Reduces frequency | ✅ Yes | ❌ No |
| Treats active attack | ❌ No | ✅ Yes |
| Onset of benefit | Weeks to months | Within hours |
If a patient on propranolol presents with an acute attack, it will not help abort it. Administer a triptan or NSAID for acute relief.
Recent Evidence
A 2024 systematic review with network meta-analysis in Health Technology Assessment reviewed preventive drug treatments for chronic migraine, confirming propranolol and other beta-blockers remain relevant in current prophylaxis strategies alongside newer CGRP antagonists.
Summary: Propranolol is a well-proven, guideline-endorsed, FDA-approved first-line agent for migraine prophylaxis. Its efficacy rate of 50-70%, once-daily long-acting formulation, and decades of clinical experience make it a practical choice - provided the patient has no contraindications (especially asthma or significant depression).
Role of pregabalin and thiocolchicide in sciatica
Finding Sources
Finding Sources
Searching PubMed
pregabalin sciatica radiculopathy
Searching PubMed
thiocolchicoside muscle relaxant back pain
Reading File
Reading File
Reading File
Searching PubMed
pregabalin neuropathic pain radiculopathy efficacy
Searching PubMed
thiocolchicoside sciatica lumbar radiculopathy
Finding Sources
Finding Sources
Searching PubMed
thiocolchicoside efficacy safety
Searching the Web
thiocolchicoside sciatica mechanism of action clinical evidence
Reading File
Reading Article
PMID: 39458083
Reading Article
PMID: 40150527
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer:
Pregabalin and Thiocolchicoside in Sciatica
Background: Understanding Sciatica
Sciatica (lumbar radiculopathy) is most commonly caused by posterolateral disc herniation at L4/5 or L5/S1 compressing a nerve root. The pain has two components:
- Neuropathic - burning, shooting, electric pain from nerve root compression/inflammation
- Mechanical/muscular - reflex paraspinal muscle spasm secondary to the underlying disc pathology
These two distinct pain mechanisms are why drugs targeting neuropathic pain (pregabalin) and muscle relaxants (thiocolchicoside) are used together in clinical practice.
PART 1: PREGABALIN IN SCIATICA
Mechanism of Action
Pregabalin is a gabapentinoid - a structural analogue of GABA, though it does not act on GABA receptors directly. Its analgesic mechanism involves:
- Binds to the α2δ (alpha-2-delta) subunit of voltage-gated calcium channels on neuronal cell surfaces
- This inhibits calcium influx into presynaptic neurons
- Reduces release of excitatory neurotransmitters (glutamate, substance P, norepinephrine)
- Produces membrane stabilization and reduces central sensitization
- Has antiepileptic, analgesic, and anxiolytic activity
The mechanism is identical to gabapentin, but pregabalin has better pharmacokinetic properties - oral bioavailability ≥90% (vs. <60% for gabapentin), more predictable dose-response, and faster absorption.
- Firestein & Kelley's Textbook of Rheumatology, p. 1002
- Miller's Anesthesia, 10th ed.
- Bradley and Daroff's Neurology in Clinical Practice
Licensed Indications for Pregabalin
Pregabalin is FDA-approved for:
- Neuropathic pain associated with diabetic peripheral neuropathy
- Postherpetic neuralgia
- Fibromyalgia
- Neuropathic pain associated with spinal cord injury
- Adjunctive therapy for partial-onset seizures
- Generalised anxiety disorder (UK only)
Sciatica is NOT a licensed indication - its use here is off-label.
- Maudsley Deprescribing Guidelines, p. 832
What Does the Evidence Say for Sciatica?
This is the most clinically important and controversial point:
The Landmark 2017 NEJM Trial
The most cited high-quality RCT (Mathieson et al., N Engl J Med 2017;376:1111-1120) specifically evaluated pregabalin in acute and chronic sciatica. The conclusion was negative - pregabalin did not provide superior pain relief over placebo for sciatica, and was associated with more adverse effects.
Current Textbook Position
| Source | Position on Pregabalin for Sciatica |
|---|---|
| Goldman-Cecil Medicine | "Pregabalin is not helpful for acute or chronic sciatica" |
| Maudsley Deprescribing Guidelines | Listed among off-label uses with "lack of evidence of efficacy" - warns of harms without clear benefit |
| Bailey & Love's Short Practice of Surgery | "A trial of pregabalin (GABA analogue) may be helpful" - leaves open as conservative option |
The guideline-level evidence is against routine use. Goldman-Cecil explicitly states it is not helpful.
- Goldman-Cecil Medicine, International Edition, p. 2507
- Maudsley Deprescribing Guidelines, p. 863
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 1036
Why Is Pregabalin Still Widely Prescribed in Sciatica?
- Sciatica has a neuropathic pain component - nerve root compression shares pathophysiology with other neuropathic conditions where pregabalin is proven
- Off-label prescribing is widespread - up to 80% of gabapentinoid use in the USA is off-label
- It is often used when standard NSAIDs and paracetamol are insufficient
- Desire to avoid opioids has driven its use as an alternative
- Some clinicians argue the 2017 NEJM trial had methodological limitations
⚠️ The Maudsley guidelines caution: widespread off-label prescribing of gabapentinoids has been partly driven by pharmaceutical marketing (with large fines paid for misrepresentation), and exposes patients to harms without proven benefits.
Dosing in Sciatica (Off-Label Practice)
| Approach | Dose |
|---|---|
| Starting dose | 75 mg BD (twice daily) |
| Titrated dose | 150 mg BD (300 mg/day) |
| Maximum | 300 mg BD (600 mg/day) |
| Duration | Typically 6-12 weeks during conservative management |
Adverse Effects of Pregabalin
| Side Effect | Frequency |
|---|---|
| Dizziness | Very common |
| Somnolence / grogginess | Very common |
| Weight gain | Common |
| Peripheral edema | Common |
| Blurred vision | Common |
| Cognitive impairment / confusion | Common |
| Dependence / withdrawal | Significant risk with prolonged use |
Pregabalin is now a Schedule 3 controlled substance in the UK due to misuse potential and dependence risk.
PART 2: THIOCOLCHICOSIDE IN SCIATICA
What Is Thiocolchicoside?
Thiocolchicoside (brand names: Muscoril, Myoril, Neoflax) is a semi-synthetic derivative of colchicine used as a centrally acting muscle relaxant with additional anti-inflammatory and analgesic properties. It is not available in the USA but is widely used in Europe, Asia (including India), and South America.
Mechanism of Action
The mechanism is incompletely understood, but involves multiple receptor targets:
| Receptor | Action | Effect |
|---|---|---|
| GABA-A receptors | Competitive antagonist (paradoxically, at lower doses may potentiate GABA) | Inhibitory CNS modulation → muscle relaxation |
| Glycine receptors | Competitive antagonist (comparable potency to GABA-A effect) | Inhibitory spinal pathway modulation |
| Nicotinic acetylcholine receptors (nAChR) | Antagonist | Neuromuscular junction modulation |
Note: Because thiocolchicoside acts as a GABA-A and glycine antagonist, it has proconvulsant potential and is contraindicated in seizure-prone individuals - an important safety point.
- Wikipedia/Synapse.patsnap; web_search sources
Role in Sciatica
In sciatica, thiocolchicoside targets the muscular/spasmodic component:
- Disc herniation triggers reflex paraspinal and paravertebral muscle spasm
- This spasm increases mechanical pressure on the nerve root, worsening radicular pain
- Thiocolchicoside relaxes this spasm, reducing the mechanical contribution to pain
- It does NOT address the neuropathic component directly
Clinical use in sciatica:
- Used as adjunct to NSAIDs, not as monotherapy
- Most evidence is for acute low back pain with sciatica, rather than pure radiculopathy
- Standard course: 4-7 days oral or IM
What Does the Evidence Say?
2024 Systematic Review & Meta-Analysis (PMID: 39458083)
- 8 RCTs, 1397 patients (mostly acute LBP/sciatica)
- Thiocolchicoside significantly reduced VAS pain scores vs. controls
- At 2-3 days: pooled MD = -0.49 (95% CI: -0.90 to -0.09)
- At 5-7 days: pooled MD = -0.82 (95% CI: -1.46 to -0.18)
- BUT: Effect sizes were below the minimally important difference (MID) of 1.0 on a 0-10 VAS scale
- All 8 RCTs had high risk of bias
- Overall certainty of evidence: very low
- Conclusion: statistically significant but clinically marginal benefit
2025 Systematic Review - Diclofenac + Thiocolchicoside Combination (PMID: 40150527)
- 9 studies, 1097 patients
- Combination therapy showed significant pain reduction and functional improvement vs. placebo or active controls
- No clear evidence of superiority over other available treatments
- Adverse effects: GI discomfort, drowsiness - no severe complications consistently reported
2023 RCT (PMID: 37301824) - IM Thiocolchicoside + Diclofenac vs. Diclofenac alone
- Single-administration IM combination was superior to diclofenac monotherapy for acute moderate-to-severe LBP in the short term
Dosing
| Route | Dose | Frequency | Duration |
|---|---|---|---|
| Oral | 8 mg | Every 12 hours | Up to 7 days |
| IM injection | 4 mg | Every 12 hours | Up to 5 days |
Adverse Effects & Safety Concerns
| Effect | Notes |
|---|---|
| Drowsiness / sedation | Common but milder than other relaxants |
| Gastrointestinal discomfort | Common |
| Teratogenicity / genotoxicity | European Medicines Agency (EMA) raised safety concerns; contraindicated in pregnancy |
| Proconvulsant | Contraindicated in epilepsy (GABA-A / glycine antagonism) |
| Hepatotoxicity | Rare case reports |
The EMA raised a formal safety concern regarding thiocolchicoside's genotoxic and reproductive toxicity potential. This has led to its withdrawal or restriction in several European countries.
Comparative Summary
| Feature | Pregabalin | Thiocolchicoside |
|---|---|---|
| Drug class | Gabapentinoid / anticonvulsant | Centrally acting muscle relaxant |
| Target | α2δ subunit of voltage-gated Ca²⁺ channels | GABA-A, glycine, nAChR antagonist |
| Pain component targeted | Neuropathic (nerve root) | Muscular spasm |
| FDA/licensed for sciatica | No (off-label) | No (not available in USA) |
| Evidence in sciatica | Negative (landmark 2017 NEJM RCT) | Marginal; statistically significant but clinically small effect |
| Guideline recommendation | Not recommended (Goldman-Cecil) | Used as NSAID adjunct in practice |
| Main concern | Dependence, overuse, withdrawal | Proconvulsant, teratogenic, EMA safety concerns |
| Duration of use | Weeks-months (with tapering) | Short-term only (≤7 days) |
Practical Clinical Perspective
For a patient with sciatica:
- First-line: NSAIDs (naproxen, diclofenac) + reassurance + physiotherapy; 70% resolve in 6-12 weeks
- Muscle spasm component: Thiocolchicoside (short-term ≤7 days) as an adjunct - modest evidence, acceptable short-term safety
- Neuropathic component: The evidence does NOT support pregabalin for sciatica despite its widespread use; reserve for truly refractory neuropathic pain after proper discussion of limited evidence and dependence risk
- Interventional: Transforaminal epidural corticosteroid injection for short-term (2-6 weeks) pain relief
- Surgery (microdiscectomy): If conservative treatment fails after 6-12 weeks, or for progressive neurological deficits
The combination of pregabalin + thiocolchicoside is commonly prescribed in India and other countries as a fixed-dose combination, but the evidence base for this combination specifically in sciatica is not robust. The 2017 NEJM trial finding that pregabalin is no better than placebo for sciatica is a sobering check on routine prescribing.
- Goldman-Cecil Medicine, p. 2507-2513
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 1036
- Thiocolchicoside meta-analysis 2024, PMID 39458083
- Diclofenac-thiocolchicoside systematic review 2025, PMID 40150527
- Mathieson et al. Trial of pregabalin for acute and chronic sciatica. N Engl J Med 2017;376:1111-1120
This is a shared conversation. Sign in to Orris to start your own chat.