Anemia
Reading File
Asking for Preferences
Finding Sources
Searching the Web
anemia classification pathophysiology diagnosis treatment overview 2024
Searching PubMed
"anemia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
anemia classification peripheral blood smear morphology types
I now have comprehensive content from Harrison's, Robbins, Goldman-Cecil and other authoritative sources. Let me compile the full overview.
Anemia — Comprehensive Overview
Definition
Anemia is defined as a reduction in red blood cell (RBC) mass below normal for a given population. Standard WHO thresholds are:
- Men: Hemoglobin (Hb) < 13 g/dL
- Women: Hb < 12 g/dL
- Pregnant women: Hb < 11 g/dL
Classification
Anemias are classified in two complementary ways:
1. By Red Cell Size (MCV-Based)
| Type | MCV | Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, thalassemia, anemia of chronic disease (ACD), sideroblastic anemia, lead poisoning |
| Normocytic | 80–100 fL | Acute blood loss, hemolysis, aplastic anemia, renal disease, hypothyroidism, multiple myeloma |
| Macrocytic | > 100 fL | B12/folate deficiency (oval macrocytes), liver disease, alcohol use, hypothyroidism, reticulocytosis, myelodysplasia (round macrocytes) |
Note: The RDW (red cell distribution width) is a useful clue — a normal RDW in microcytosis favors thalassemia over iron deficiency (which typically raises RDW).
2. By Mechanism (Reticulocyte-Based)
| Category | Reticulocyte Count | Causes |
|---|---|---|
| Hyperproduction (loss/destruction) | ↑ Elevated | Bleeding, hemolytic anemia (autoimmune, mechanical, congenital) |
| Underproduction | ↓ Low or inappropriately normal | Nutritional deficiency, marrow replacement, aplastic anemia, EPO deficiency |
Major Types in Detail
🔴 Iron Deficiency Anemia (IDA)
Most common anemia worldwide — affects ~25–50% in lower-resource countries.
Pathophysiology:
- Iron is essential for heme synthesis (4 Fe atoms per hemoglobin molecule)
- Iron absorption is regulated by hepcidin (liver peptide) via ferroportin inhibition
- Inflammation raises hepcidin → blocks iron absorption and release from stores
- Causes: Chronic blood loss (GI, menstrual), poor dietary intake, malabsorption (celiac, post-gastrectomy), pregnancy
Lab findings:
| Test | Iron Deficiency |
|---|---|
| Serum ferritin | ↓ < 30 μg/L (depleted stores) |
| Serum iron | ↓ |
| TIBC | ↑ |
| Transferrin saturation | ↓ < 20% |
| MCV | ↓ (microcytic) |
| RDW | ↑ |
| Peripheral smear | Hypochromic, microcytic cells |
Treatment: Oral ferrous sulfate (150–200 mg elemental iron/day); IV iron (e.g., ferric carboxymaltose) for malabsorption/intolerance. Treat underlying cause.
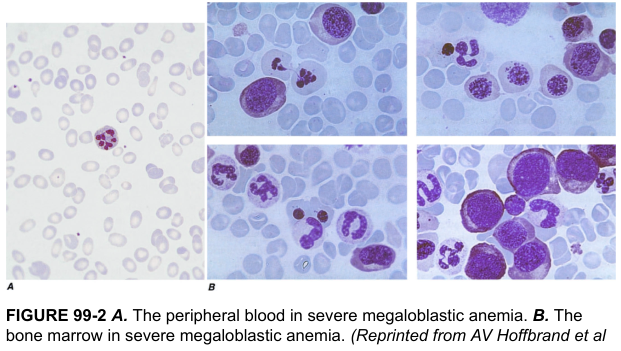
🟠 Megaloblastic Anemia (B12 / Folate Deficiency)
Mechanism: Defective DNA synthesis in erythroid precursors → nuclear–cytoplasmic asynchrony → large, immature megaloblasts.
Key features:
- Oval macrocytes on smear
- Hypersegmented neutrophils (≥5 lobes — pathognomonic)
- Bone marrow: hypercellular with giant megaloblasts
- B12 deficiency also causes subacute combined degeneration of the spinal cord (demyelination of posterior and lateral columns)
Causes of B12 deficiency: Pernicious anemia (anti-intrinsic factor antibodies), strict veganism, terminal ileal disease (Crohn's), gastrectomy
Causes of folate deficiency: Poor diet, pregnancy, malabsorption, methotrexate, phenytoin, alcohol
Lab: ↑ MCV, ↑ homocysteine (both), ↓ methylmalonic acid (MMA only in B12 deficiency — key differentiator)
Treatment: B12 (IM cyanocobalamin for pernicious anemia; oral B12 if dietary); folic acid 1–5 mg/day orally for folate deficiency.
🟡 Anemia of Chronic Disease / Anemia of Inflammation (ACD/AI)
Second most common anemia globally (up to 40% of hospital patients).
Pathophysiology:
- Chronic inflammation ↑ IL-6 → ↑ hepcidin → ferroportin degradation → impaired iron release from macrophages and reduced intestinal absorption
- Inflammatory cytokines (TNF) also suppress EPO production and erythropoiesis directly
Lab:
- Typically normocytic (sometimes mildly microcytic, MCV rarely < 75 fL)
- Low serum iron AND low TIBC (distinguishes from IDA where TIBC is high)
- Ferritin normal or ↑ (acute phase reactant)
- Low reticulocyte count
Treatment: Treat underlying disease; IV iron ± ESAs (erythropoiesis-stimulating agents) in renal/cancer contexts.
🔵 Hemolytic Anemias
Accelerated RBC destruction → shortened lifespan (< 120 days normal). Hallmarks: ↑ reticulocytes, ↑ LDH, ↓ haptoglobin, indirect hyperbilirubinemia, splenomegaly.
Extravascular vs. Intravascular Hemolysis
| Feature | Extravascular | Intravascular |
|---|---|---|
| Mechanism | Splenic macrophage phagocytosis | RBC lysis within vessels |
| Hemoglobinuria | Absent | Present |
| Hemoglobinemia | Absent | Present |
| Jaundice | Yes | Less prominent |
| Haptoglobin | ↓ | ↓↓ |
| Iron deficiency | No | Yes (iron lost in urine) |
| Splenomegaly | Common | Less common |
Classification by Cause
Intrinsic (Intracorpuscular) Defects:
| Category | Disease |
|---|---|
| Membrane defects | Hereditary spherocytosis (AD; spectrin/ankyrin mutations), hereditary elliptocytosis |
| Enzyme defects | G6PD deficiency (X-linked; oxidative stress triggers hemolysis), pyruvate kinase deficiency |
| Hemoglobinopathies | Sickle cell disease (HbS polymerization → vaso-occlusion), unstable hemoglobins |
| Deficient globin synthesis | Thalassemia syndromes (α and β) |
| Acquired (PNH) | Paroxysmal nocturnal hemoglobinuria (GPI-anchor deficiency → complement-mediated lysis) |
Extrinsic (Extracorpuscular) Defects:
| Category | Examples |
|---|---|
| Autoimmune | Warm AIHA (IgG, Coombs+), Cold agglutinin disease (IgM) |
| Microangiopathic (MAHA) | TTP, HUS, DIC, malignant hypertension — schistocytes on smear |
| Infections | Malaria, babesiosis, clostridial sepsis |
| Mechanical | Prosthetic valve hemolysis, march hemoglobinuria |
Diagnostic workup: Direct antiglobulin test (DAT/Coombs), peripheral smear, osmotic fragility, G6PD assay, Hb electrophoresis, flow cytometry (PNH).
⚪ Aplastic Anemia
Bone marrow failure with pancytopenia (anemia + thrombocytopenia + neutropenia). Marrow is markedly hypocellular.
Pathogenesis:
- Immune-mediated (70–80%): Autoreactive T-cells destroy hematopoietic stem cells; responds to immunosuppression
- Intrinsic stem cell defect: Telomerase mutations (5–10%), short telomeres (50% of cases)
- Precipitants: drugs (chloramphenicol, benzene, carbamazepine), viral infections, radiation; often idiopathic
Clinical: Insidious onset of weakness, pallor, petechiae (thrombocytopenia), recurrent infections (neutropenia). No splenomegaly (distinguishes from other causes).
Treatment:
- < 40 years, suitable donor → hematopoietic stem cell transplantation (HSCT) — often curative
- Not transplant candidates → immunosuppression (anti-thymocyte globulin + cyclosporine); restores hematopoiesis in 60–70%
🟤 Myelophthisic Anemia
Space-occupying marrow lesions (metastatic breast/lung/prostate cancer, TB, granulomas) displace normal hematopoiesis.
Peripheral smear: Leukoerythroblastosis — teardrop cells, nucleated RBCs, immature granulocytes. Requires bone marrow biopsy for diagnosis.
Diagnostic Approach
↓ Hb / Hct
│
┌───────────────┼───────────────┐
Microcytic Normocytic Macrocytic
(MCV <80) (MCV 80–100) (MCV >100)
│ │ │
Iron studies Reticulocyte count B12, folate,
Ferritin, TIBC │ TFTs, LFTs
│ ┌────┴────┐
│ Elevated Low/Normal
│ │ │
│ Hemolysis Aplastic/ACD/
│ workup Renal/Marrow Rx
┌─────┴──────┐
Low ferritin Normal/↑ ferritin
= IDA ↑ TIBC → IDA
Normal TIBC → ACD
↑ TIBC → Thalassemia trait
Key labs to order:
- CBC with differential and reticulocyte count
- Peripheral blood smear (mandatory)
- Iron studies: serum Fe, ferritin, TIBC, transferrin saturation
- B12, folate, LDH, haptoglobin
- Direct Coombs (if hemolysis suspected)
- Bone marrow biopsy (if cause unclear or pancytopenia)
Clinical Features (General)
| Severity | Hb | Symptoms |
|---|---|---|
| Mild | 10–12 g/dL | Often asymptomatic; fatigue on exertion |
| Moderate | 8–10 g/dL | Fatigue, palpitations, dyspnea on exertion, pallor |
| Severe | < 8 g/dL | Rest dyspnea, tachycardia, angina, heart failure |
| Very severe | < 6 g/dL | High-output cardiac failure, altered consciousness |
Specific signs: conjunctival pallor, koilonychia (spoon nails — IDA), glossitis, angular cheilitis, jaundice (hemolysis), splenomegaly (hemolysis, thalassemia), neurological signs (B12 deficiency).
Treatment Summary
| Type | First-line Treatment |
|---|---|
| Iron deficiency | Oral/IV iron; treat cause |
| B12 deficiency | IM cyanocobalamin (if pernicious anemia); oral B12 |
| Folate deficiency | Oral folic acid 1–5 mg/day |
| ACD/AI | Treat underlying disease; IV iron ± ESAs |
| Hemolytic (AIHA warm) | Corticosteroids → rituximab → splenectomy |
| Aplastic anemia | HSCT (young) or immunosuppression (ATG + CsA) |
| Sickle cell | Hydroxyurea, transfusion support, HSCT |
| Thalassemia | Transfusions, iron chelation, HSCT |
Sources:
- Harrison's Principles of Internal Medicine 22E, Ch. 66 (Anemia Definition & Classification)
- Robbins & Kumar Basic Pathology, Ch. 10 (Red Cell Disorders — Iron Deficiency, Hemolytic Anemias, Aplastic Anemia)
- Goldman-Cecil Medicine, Ch. 144–151 (Anemias)
- Recent meta-analyses (PMID 40159279 — IV iron in heart failure + iron deficiency; PMID 40392014 — mixed AIHA)
How will you clinically classify anemia by looking pallor , and give differential diagnosis of pallor with discussion
Finding Sources
Finding Sources
Searching the Web
clinical classification anemia by pallor conjunctival palmar differential diagnosis pallor
Finding Sources
Finding Sources
Reading Web Page
https://epomedicine.com/clinical-medicine/clinical-examinati…
Finding Sources
Finding Sources
Searching Images
conjunctival pallor clinical examination anemia palpebral conjunctiva
Finding Sources
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.