Obstructive vs restrictive pulmonology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compose the full answer.
Obstructive vs. Restrictive Pulmonary Disease
These are the two fundamental physiological categories of diffuse lung disease, distinguished primarily by their patterns on pulmonary function testing (PFT).
Core Definitions
| Obstructive | Restrictive | |
|---|---|---|
| Mechanism | Increased resistance to airflow - partial or complete obstruction at any airway level | Reduced expansion of lung parenchyma - the lungs are "stiff" or the chest wall/neuromuscular apparatus limits inflation |
| Problem | Air can't get out fast enough | The lungs can't get big enough |
Robbins & Kumar Basic Pathology: "Obstructive disease [is] characterized by an increase in resistance to airflow... restrictive disease [is] marked by reduced expansion of lung parenchyma and decreased total lung capacity."
Causes
Obstructive:
- COPD (emphysema + chronic bronchitis) - most common; ~80% attributable to smoking
- Asthma - airway narrowing (reversible)
- Bronchiectasis - chronic airway dilation and inflammation
- Bronchiolitis obliterans
Restrictive - two broad categories:
- Intrinsic (parenchymal) - acute or chronic interstitial lung disease
- ARDS (acute)
- Pulmonary fibrosis (IPF), sarcoidosis, pneumoconioses, hypersensitivity pneumonitis (chronic)
- Extrinsic (extraparenchymal) - normal lungs, but restricted expansion
- Neuromuscular disease (Guillain-Barre, ALS, myasthenia gravis)
- Chest wall deformity (kyphoscoliosis)
- Severe obesity
- Pleural disease (effusion, fibrosis)
Pulmonary Function Tests (PFTs)
This is the cornerstone of differentiation:
| Parameter | Obstructive | Restrictive |
|---|---|---|
| FVC | Normal or slightly ↓ | ↓↓↓ |
| FEV₁ | ↓↓↓ | ↓↓ (proportional) |
| FEV₁/FVC ratio | ↓↓↓ (<0.70) | Normal (>0.80) |
| FEF₂₅₋₇₅% | ↓↓↓ | Normal |
| TLC | Normal or ↑ (air trapping) | ↓↓↓ (confirmatory) |
| RV | ↑ (gas trapping) | ↓ (or elevated in extraparenchymal) |
| FRC | Normal or ↑ | ↓↓↓ |
| PEFR | ↓↓ | Normal or ↓ |
| DLCO | ↓ in emphysema (alveolar destruction); normal in pure asthma/bronchitis | ↓ in ILD (thickened membrane); normal/↓ in extraparenchymal |
Bailey and Love's Short Practice of Surgery: "A low ratio indicates obstruction... A normal ratio (FVC and FEV₁ reduced to the same extent) indicates a restrictive pathology."
Key rule: TLC is the gold standard confirmatory test for restriction. Spirometry alone showing a "restrictive pattern" is confirmed only when TLC is below the lower limit of normal. In ~50% of cases where spirometry suggests restriction, lung volumes turn out to be normal (pseudorestriction from air trapping) - Murray & Nadel's Textbook of Respiratory Medicine.
Lung Volume Diagram
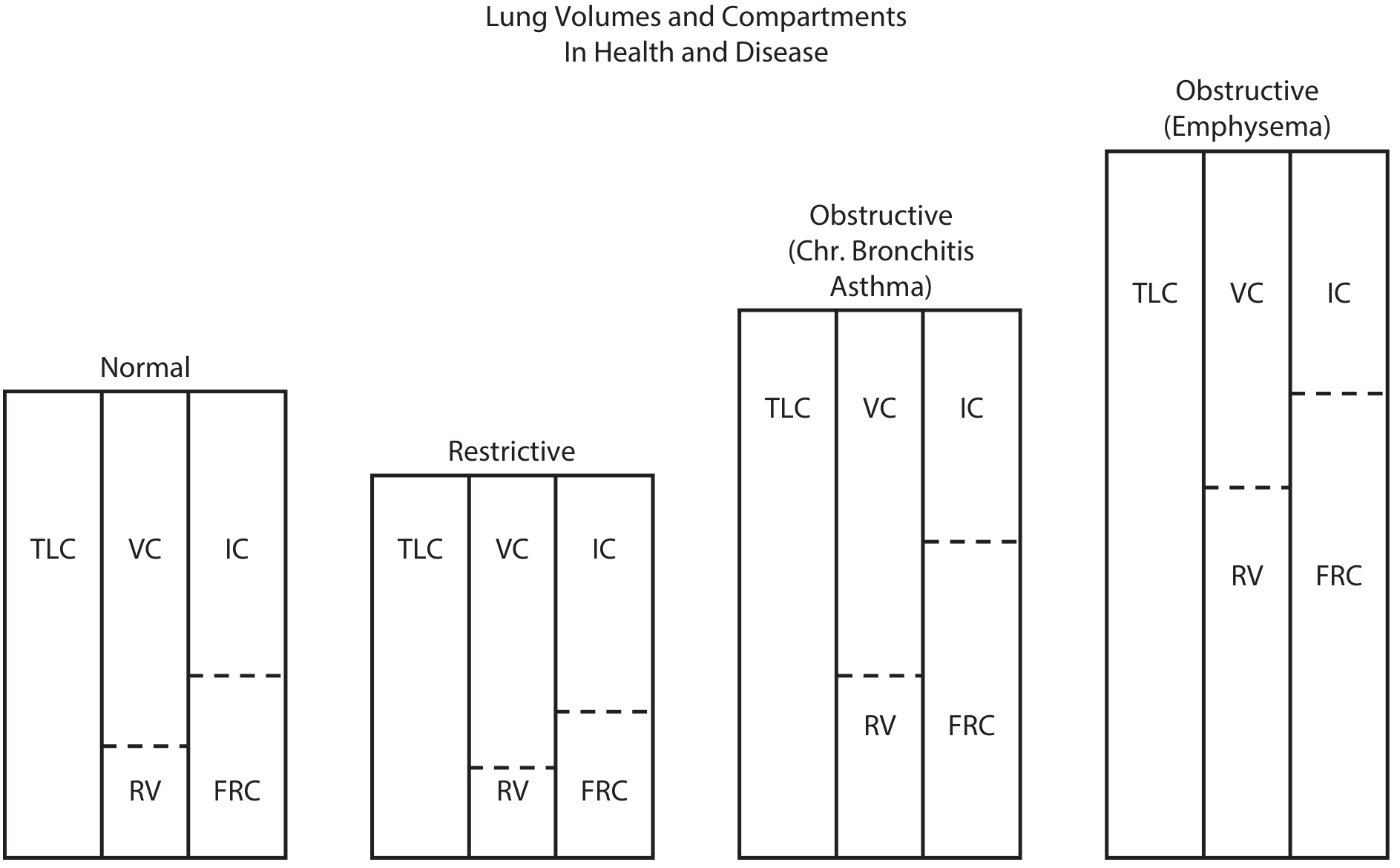
K.J. Lee's Essential Otolaryngology: In restrictive disease, all compartments (TLC, VC, IC, RV, FRC) are uniformly reduced. In obstructive disease - especially emphysema - TLC, RV, and FRC are all increased due to hyperinflation and air trapping.
Flow-Volume Loop Patterns
| Pattern | Shape |
|---|---|
| Normal | Triangular - rapid peak flow, gradual linear descent |
| Obstructive | Concave (scooped-out) expiratory limb - low peak flow, progressive slowing; the entire loop is shifted right (increased RV) |
| Restrictive | Narrow, tall loop - reduced volumes on both axes but the shape is preserved (no scooping); peak flow may actually be elevated relative to FVC |
Pathophysiology of Each Obstruction Mechanism
Emphysema: Permanent enlargement of air spaces distal to terminal bronchioles. Loss of elastic recoil means the airways collapse during forced expiration. The FEV₁ falls not because of intrinsic airway narrowing but because the driving pressure (elastic recoil) is lost.
Asthma: Bronchospasm + mucosal edema + mucus plugging narrows the lumen. Key distinguishing feature: reversibility - FEV₁ improves ≥12% and ≥200 mL after bronchodilator. Spirometry example from Bailey & Love: FEV₁ pre-bronchodilator 1.4 L → post-bronchodilator 2.5 L, FEV₁/FVC 40% → 71%.
Chronic Bronchitis: Hypersecretion and luminal inflammation; defined clinically (productive cough ≥3 months/year for ≥2 years).
Restrictive (ILD): Thickened alveolar walls impair gas diffusion AND reduce compliance - lungs are stiff. DLCO is the most sensitive early marker for ILD.
Mixed Defect
When both FEV₁/FVC and TLC are below the lower limit of normal, a mixed obstructive-restrictive defect is present. The FEV₁ % predicted is used to grade overall severity in these cases. - Murray & Nadel's Textbook of Respiratory Medicine
Quick Clinical Summary
| Feature | Obstructive | Restrictive |
|---|---|---|
| Prototype diseases | COPD, asthma | IPF, sarcoidosis, kyphoscoliosis |
| Symptoms | Wheeze, prolonged expiration, barrel chest (in emphysema) | Dyspnoea on exertion, dry cough, fine crackles (ILD) |
| CXR/CT | Hyperinflation, flat diaphragms (emphysema); bronchial wall thickening (chronic bronchitis) | Reticular pattern, honeycombing (ILD); reduced lung volumes |
| Bronchodilator response | May improve (especially asthma) | No improvement |
| PFT key | FEV₁/FVC < 0.70 | TLC < LLN, FEV₁/FVC normal |
Sources: Robbins & Kumar Basic Pathology; Bailey and Love's Short Practice of Surgery, 28th ed.; Murray & Nadel's Textbook of Respiratory Medicine, 2-Vol.; Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e; K.J. Lee's Essential Otolaryngology.
This is a shared conversation. Sign in to Orris to start your own chat.