Shock
Reading File
Finding Sources
Searching PubMed
"shock" AND "classification" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed answer on Shock.
Shock
Shock is defined as a state of systemic tissue hypoperfusion - either from reduced cardiac output or reduced effective circulating blood volume - that leads to cellular hypoxia. At the outset, the cellular injury is reversible; prolonged shock leads to irreversible tissue injury and is often fatal.
(Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology)
Types / Classification
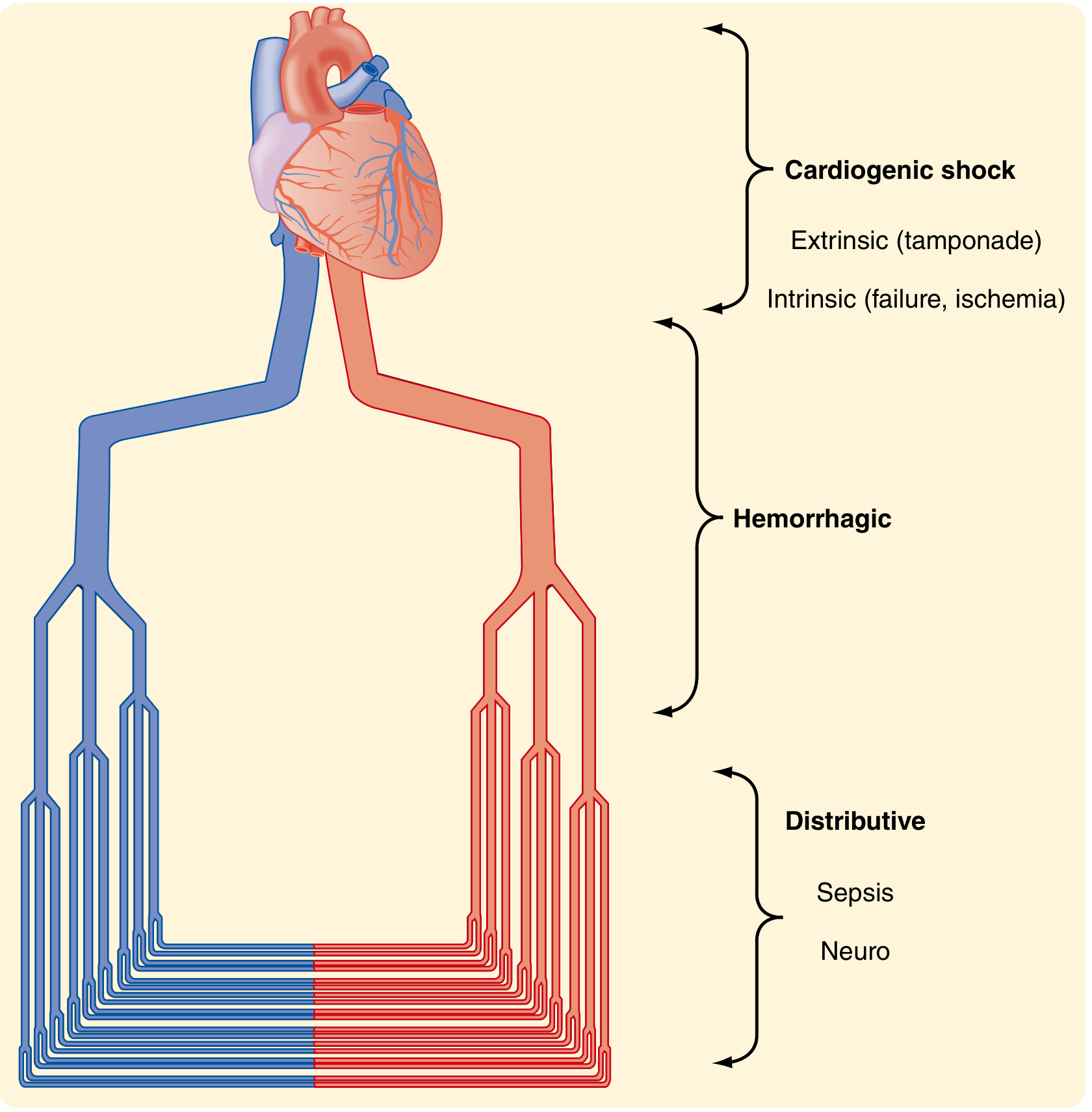
Figure: Types of shock - Sabiston Textbook of Surgery
1. Cardiogenic Shock
- Mechanism: Failure of myocardial pump - low cardiac output despite adequate blood volume
- Causes:
- Intrinsic myocardial damage: MI, myocarditis
- Ventricular arrhythmias
- Extrinsic compression: cardiac tamponade
- Outflow obstruction: pulmonary embolism
- Characterized by: low CO, high SVR (compensatory), elevated filling pressures (PCWP), cool/clammy skin
2. Hypovolemic Shock
- Mechanism: Inadequate blood/plasma volume leading to low cardiac output
- Causes: Hemorrhage, vomiting, diarrhea, burns, trauma, third-spacing
- Most commonly studied form; basis for ATLS classification
3. Septic Shock (Distributive)
- Mechanism: Dysregulated host response to infection causing peripheral vasodilation and maldistribution of blood flow
- Sepsis = life-threatening organ dysfunction from dysregulated host response to infection
- Septic shock = subset with profound circulatory, cellular, and metabolic abnormalities + greater mortality than sepsis alone
- Most commonly triggered by: gram-positive bacteria > gram-negative bacteria > fungi
- Hemodynamics: high CO (early), low SVR, warm/flushed skin ("warm shock")
4. Neurogenic Shock (Distributive)
- Loss of sympathetic vascular tone after spinal cord injury or high spinal anesthesia
- Acute vasodilation leads to hypotension and tissue hypoperfusion
- Characterized by bradycardia (unlike other shock types) + hypotension
5. Anaphylactic Shock (Distributive)
- IgE-mediated hypersensitivity reaction
- Systemic vasodilation + increased vascular permeability
- Bronchospasm, urticaria, angioedema accompanying hypotension
6. Obstructive Shock
- Obstruction to cardiac output despite normal pump and volume: massive PE, tension pneumothorax, cardiac tamponade
ATLS Classification of Hemorrhagic Shock
| Class I | Class II | Class III | Class IV | |
|---|---|---|---|---|
| Blood loss (%) | 0-15 | 15-30 | 30-40 | >40 |
| CNS | Slightly anxious | Mildly anxious | Anxious / confused | Confused / lethargic |
| Pulse (bpm) | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20/min | 20-30/min | 30-40/min | >35/min |
| Urine (mL/hr) | >30 | 20-30 | 5-15 | Negligible |
| Fluid | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
(Sabiston Textbook of Surgery)
Note: These classes were arbitrarily generated and not rigorously validated. Children compensate with large blood loss (showing mainly tachycardia until a tipping point), while elderly patients decompensate earlier.
Stages of Shock
Shock progresses through three general stages (best documented in hypovolemic shock):
Stage 1: Nonprogressive (Compensated)
Reflex compensatory mechanisms activated; vital organ perfusion maintained:
- Baroreceptor reflexes activated
- Catecholamine + ADH release
- Renin-angiotensin-aldosterone axis activation
- Generalized sympathetic stimulation
- Result: Tachycardia, peripheral vasoconstriction, renal fluid conservation
- Skin: cool, pale (cutaneous vasoconstriction shunts blood to heart and brain)
- Exception: Septic shock may initially cause warm, flushed skin from vasodilation
Stage 2: Progressive
Underlying causes not corrected; widespread tissue hypoxia ensues:
- Aerobic respiration replaced by anaerobic glycolysis → lactic acid accumulation
- Metabolic lactic acidosis blunts vasomotor response → arterioles dilate
- Blood pools in microcirculation → worsening cardiac output
- Endothelial anoxic injury → risk of DIC
- Vital organs begin to fail
Stage 3: Irreversible
- Severe widespread cell injury with lysosomal enzyme leakage
- Myocardial contractile function worsens (increased NO synthesis)
- Ischemic bowel allows intestinal flora to enter circulation → superimposed bacteremic shock
- Renal failure from ischemic tubular injury (ATN)
- Downward spiral culminating in death despite best therapeutic interventions
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
Pathogenesis of Septic Shock
Five major mechanisms:
1. Inflammatory and counterinflammatory responses
- Microbial PAMPs engage TLRs, G-protein-coupled receptors, C-type lectin receptors
- Trigger massive proinflammatory cytokine (TNF, IL-1, IL-6, IL-12) and anti-inflammatory (IL-10, TGF-β) responses simultaneously
2. Endothelial activation and injury
- Cytokines loosen tight junctions → protein-rich edema throughout body
- Upregulated NO and vasoactive mediators (C3a, C5a, PAF) → systemic vasodilation and hypotension
- Microvascular dysfunction: heterogeneous capillary flow, loss of autoregulation → oxygen delivery/need mismatch
3. Induction of procoagulant state
- Increased tissue factor on monocytes and endothelium
- Decreased anticoagulant factors (TFPI, thrombomodulin, protein C)
- Increased PAI-1 → impaired fibrinolysis
- Neutrophil extracellular traps (NETs) promote coagulation
- → Systemic thrombin activation → DIC in up to 50% of patients
4. Metabolic abnormalities
- Insulin resistance and hyperglycemia (cytokines + stress hormones suppress insulin, induce gluconeogenesis)
- Elevated blood glucose, triglycerides, and lactate
- Hyperglycemia suppresses neutrophil bactericidal activity
- Adrenal insufficiency (from DIC causing adrenal necrosis = Waterhouse-Friderichsen syndrome, or suppressed synthesis)
- Lactic acidosis from reduced oxidative phosphorylation
5. Organ dysfunction
- Hypotension + interstitial edema + microvascular dysfunction + small vessel thrombosis
- Mitochondrial damage from oxidative stress impairs oxygen utilization
- High cytokines/mediators diminish myocardial contractility → ARDS, ATN, hepatic failure
Morphologic Changes (Organs Affected)
The cellular effects of shock are essentially hypoxic injury + microvascular thrombosis:
| Organ | Changes |
|---|---|
| Brain | Ischemic encephalopathy; watershed infarcts |
| Heart | Subendocardial hemorrhage/necrosis; focal myocyte necrosis (contraction band necrosis) |
| Kidneys | Acute tubular necrosis (ATN) - most common cause of ARF in shock |
| Adrenals | Cortical lipid depletion (increased steroid synthesis from stress) |
| GI tract | Hemorrhagic enterocolitis; mucosal ulcerations; bacterial translocation |
| Liver | Centrilobular necrosis (zone 3 - farthest from blood supply) |
| Lungs | Resistant in pure hypovolemic shock; but ARDS in septic/traumatic shock |
Fibrin microthrombi most readily seen in kidney glomeruli.
(Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease)
Lactate in Shock
- Traditionally viewed as a byproduct of anaerobic metabolism (oxygen debt marker)
- Current evidence shows lactate is also an active metabolite / energy shuttle - transferred between tissues and oxidized as fuel in heart, brain, liver, and kidney
- Elevated lactate in shock can result from: anaerobic glycolysis, high adrenergic state, and impaired hepatic clearance
- Lactate remains a key clinical marker of injury severity and resuscitation adequacy, despite evolving understanding of its role
- Base deficit is a complementary marker
(Sabiston Textbook of Surgery)
Prognosis
| Type | Mortality |
|---|---|
| Hypovolemic (young, healthy) | <10% with appropriate management |
| Septic shock | 20-40% |
| Cardiogenic shock | High, even with state-of-the-art care |
Key Concepts (Summary)
- Shock = systemic tissue hypoperfusion → cellular hypoxia → organ failure
- Three major types: cardiogenic, hypovolemic, septic (+ neurogenic, anaphylactic, obstructive)
- Evolves through: nonprogressive → progressive → irreversible stages
- Septic shock: endothelial injury + vasodilation + DIC + metabolic derangements
- ATLS classifies hemorrhagic shock in 4 classes based on blood loss and clinical signs
- Organs most vulnerable: brain, heart, kidneys, adrenals, GI tract
- Lactate and base deficit are key clinical markers of shock severity
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.