Collapse of lung lobes and thier findings in x ray and ct With images and explaination
Reading File
Finding Sources
Finding Sources
Searching the Web
lobar collapse lung lobe atelectasis X-ray CT findings images radiology
Finding Sources
Finding Sources
Reading Web Page
https://radiopaedia.org/articles/lobar-lung-collapse?lang=us
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and images. Let me compile the complete answer now.
Lobar Collapse of the Lung - Imaging Findings (X-Ray & CT)
Source: Grainger & Allison's Diagnostic Radiology
What Is Lobar Collapse?
Lobar collapse (atelectasis) refers to loss of volume within an entire lung lobe. The two terms are often used interchangeably - "collapse" typically denotes complete loss of volume, while "atelectasis" is broader and includes partial or subsegmental forms.
Causes:
- Endobronchial obstruction (intrinsic): Bronchogenic carcinoma (most common in older smokers), mucous plugs, carcinoid, metastases, foreign bodies, granulomatous disease (TB, sarcoidosis)
- Extrinsic compression: Enlarged lymph nodes, aortic aneurysm, mediastinal masses
- Non-obstructive: Pleural effusion (passive/compressive atelectasis), pneumothorax, loss of surfactant (ARDS)
General Radiographic Signs of Lobar Collapse
Direct signs (volume loss):
- Fissure displacement - the key direct sign; fissures shift toward the collapsed lobe
- Displacement of pulmonary vessels and bronchi toward the collapsed area
Indirect signs (compensatory changes):
- Hyperinflation of remaining ipsilateral and contralateral lobes
- Ipsilateral hemidiaphragm elevation
- Mediastinal/tracheal shift toward the collapse
- Hilar displacement (upward for upper lobe, downward for lower lobe)
- Increased rib cage intercostal space narrowing ipsilaterally
The increased opacity of the affected lobe with volume loss is the cardinal feature on any radiograph.
Schematic overview of all lobar collapses

Diagrammatic summary: RUL, RML, RLL, LUL, LLL, and combined RML+RLL atelectasis patterns on frontal (top row) and lateral (bottom row) views
1. Right Upper Lobe (RUL) Collapse
X-Ray Findings:
- Frontal: Opacity in the right upper zone with upward displacement of the minor (horizontal) fissure. The hilum is pulled upward. The superior mediastinum shifts to the right. The trachea deviates to the right.
- Lateral: The minor fissure moves superiorly and anteriorly; the upper lobe collapses anterosuperiorly.
- "Golden S sign" (S-shaped or reverse S curve): seen when collapse is due to a central hilar mass - the lateral curve of the displaced fissure and the medial convexity of the tumor create the S configuration.
CT Findings:
- Triangular/wedge-shaped density in the anterosuperior right hemithorax
- Elevated minor fissure and mediastinal shift
- Well-demonstrates any endobronchial cause
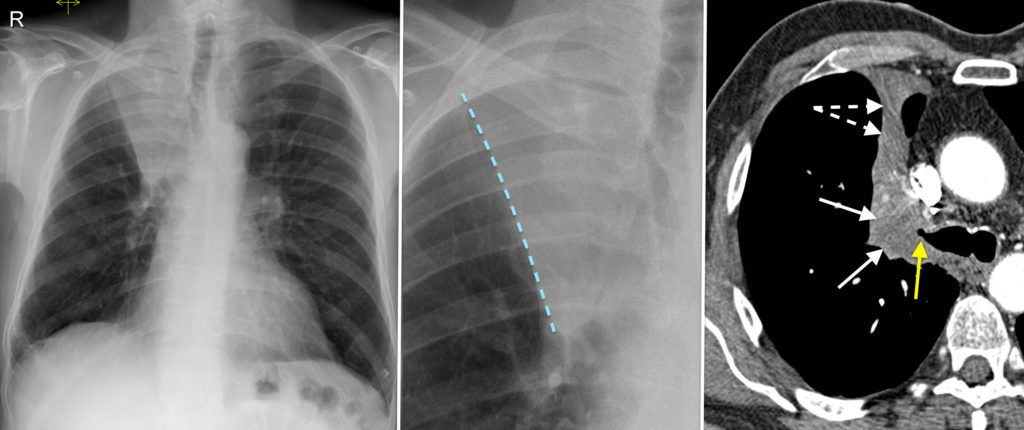
Right Upper Lobe Collapse: PA film (left) - note right upper zone opacity with tracheal/mediastinal shift. Lateral film (centre) - anterosuperior collapse shown by blue dashed fissure line. CT axial (right) - triangular wedge of soft tissue (white arrows) anterior to right mediastinum; yellow arrow = collapsed lobe; dashed arrowheads = displaced fissure
2. Right Middle Lobe (RML) Collapse
X-Ray Findings:
- Frontal: Subtle loss of clarity of the right heart border (silhouette sign) due to the middle lobe lying adjacent to it. Triangular opacity adjacent to the right heart border pointing toward the hilum.
- Lateral (most useful view!): Classic "bowtie" or triangular band of opacity between the minor fissure (superiorly) and the major fissure (inferiorly). The two fissures converge anteriorly.
CT Findings:
- Flat/triangular collapsed lobe adjacent to the right heart border
- Both major and minor fissures approximate toward each other
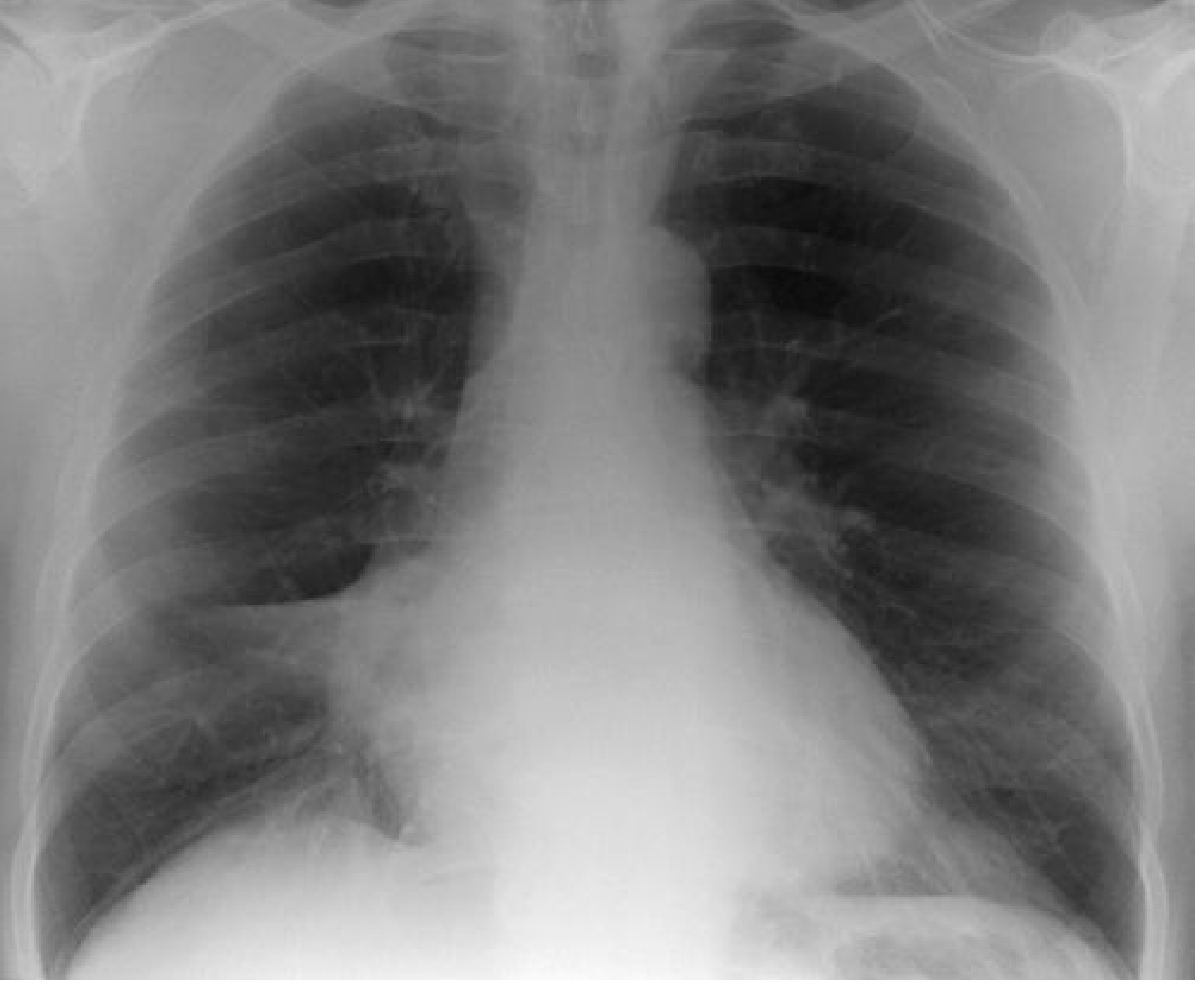
Fig. 7.26 (Grainger & Allison's) - Right Middle Lobe Collapse showing characteristic triangular density adjacent to the right heart border
3. Right Lower Lobe (RLL) Collapse
X-Ray Findings:
- Frontal: Triangular density behind the heart and right hemidiaphragm. The right hemidiaphragm outline may be partially preserved (because middle lobe remains between collapsed lower lobe and diaphragm). The right lower lobe pulmonary artery is not visible (no longer outlined by aerated lung).
- Lateral: Increased density in the posterior costophrenic angle; loss of silhouette of the right hemidiaphragm posteriorly.
- Superior triangle sign: Triangular density to the right of mediastinum (from displacement of anterior junctional structures) - do not confuse with RUL collapse.
- Rightward hilar displacement
CT Findings:
- Collapsed lobe lies posteromedially in the right hemithorax
- Fissure displaced posteriorly and medially
- CT mucous bronchogram sign: tubular low-attenuation branching structures within enhancing collapsed lobe
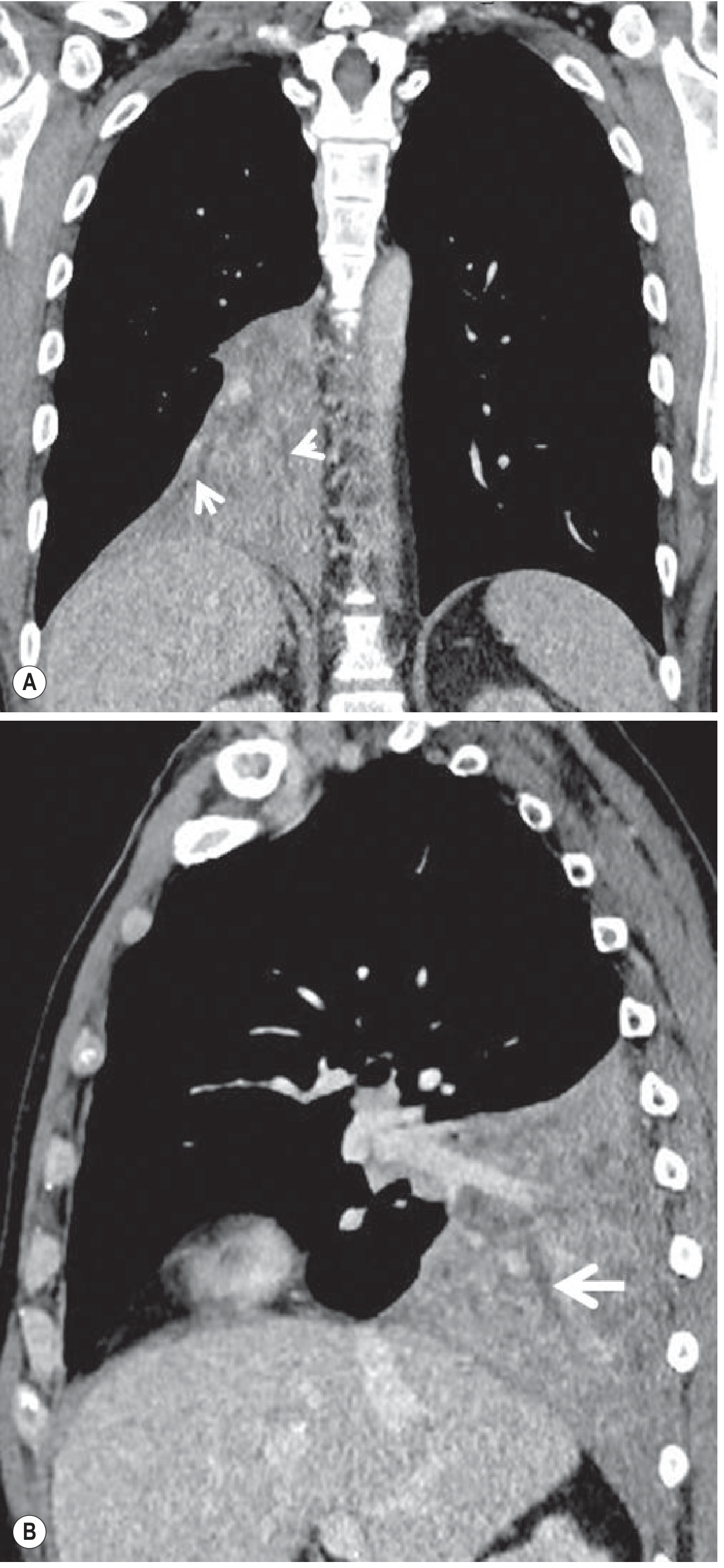
Fig. 7.11 (Grainger & Allison's) - Contrast-enhanced coronal (A) and sagittal (B) CT of right lower lobe collapse due to squamous cell carcinoma. Arrows show the CT mucous bronchogram sign (linear low-attenuation airways within the enhancing lobe)
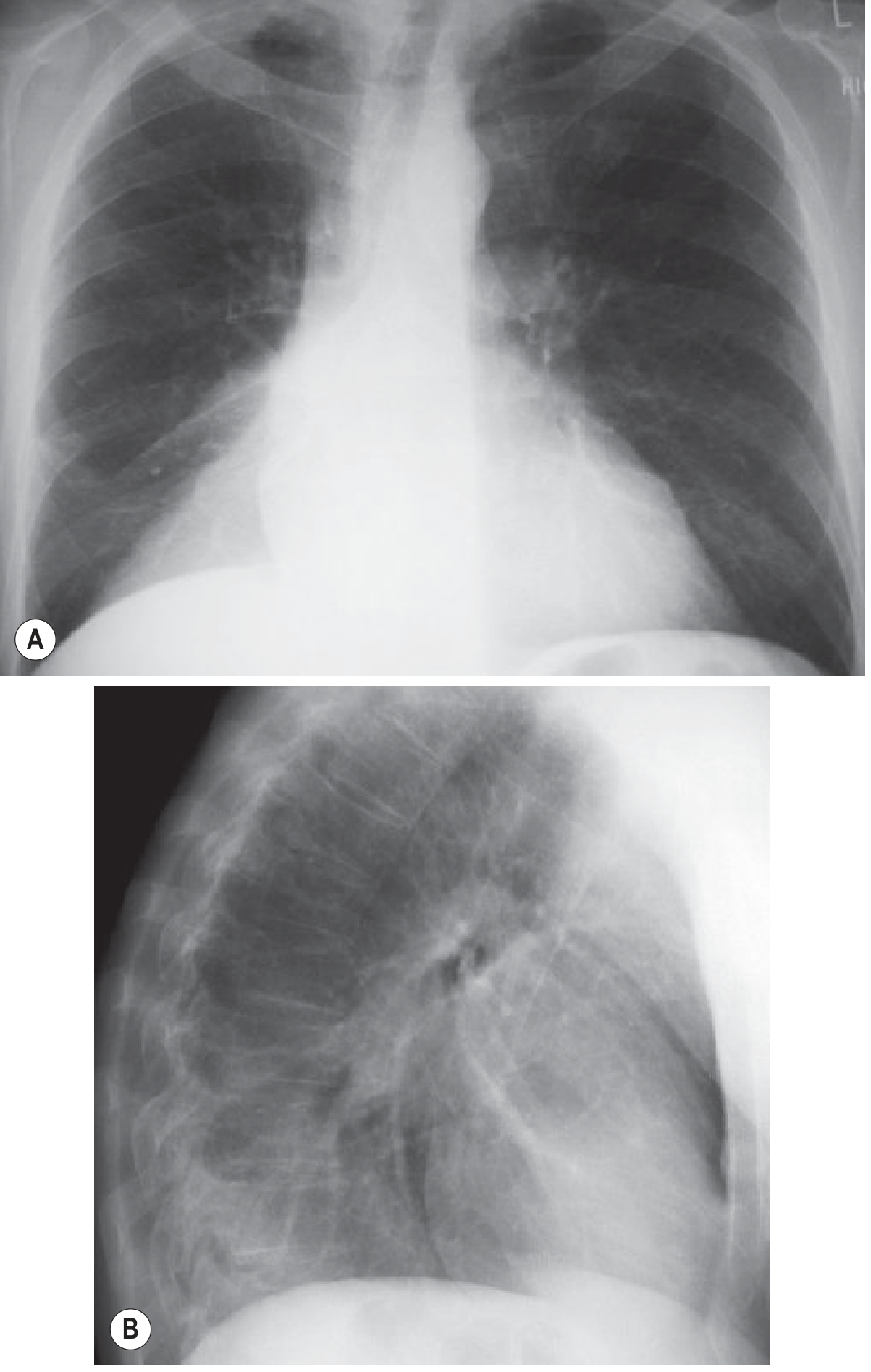
Fig. 7.27 (Grainger & Allison's) - Right Lower Lobe Collapse: (A) Frontal - triangular density, hemidiaphragm silhouette partly preserved. (B) Lateral - posterior CP angle opacity with loss of right diaphragm posteriorly
4. Left Upper Lobe (LUL) Collapse
The left upper lobe has no minor fissure (only the oblique/major fissure), so it collapses anteriorly rather than superiorly - this creates a very different pattern from right upper lobe collapse.
X-Ray Findings:
- Frontal: Veil-like hazy opacity over the left upper hemithorax (not a well-demarcated border). The left hilum is elevated and the trachea deviates to the left.
- The aortic knuckle may be obscured (silhouette sign) - the left heart border may be partially preserved if the lingula is spared.
- Horizontal reorientation of the left mainstem bronchus.
- Luftsichel sign (crescent of air): Hyperinflated superior segment of the left lower lobe interposes between the aortic knuckle and the collapsed left upper lobe, creating a lucent crescent at the left apex - highly specific sign for LUL collapse.
CT Findings:
- Anteriorly displaced oblique fissure
- Triangular/slab-like density anterior to the left mediastinum
- "Pita bread" sign on axial CT - the collapsed LUL forms a flat slab anterior to the hilum
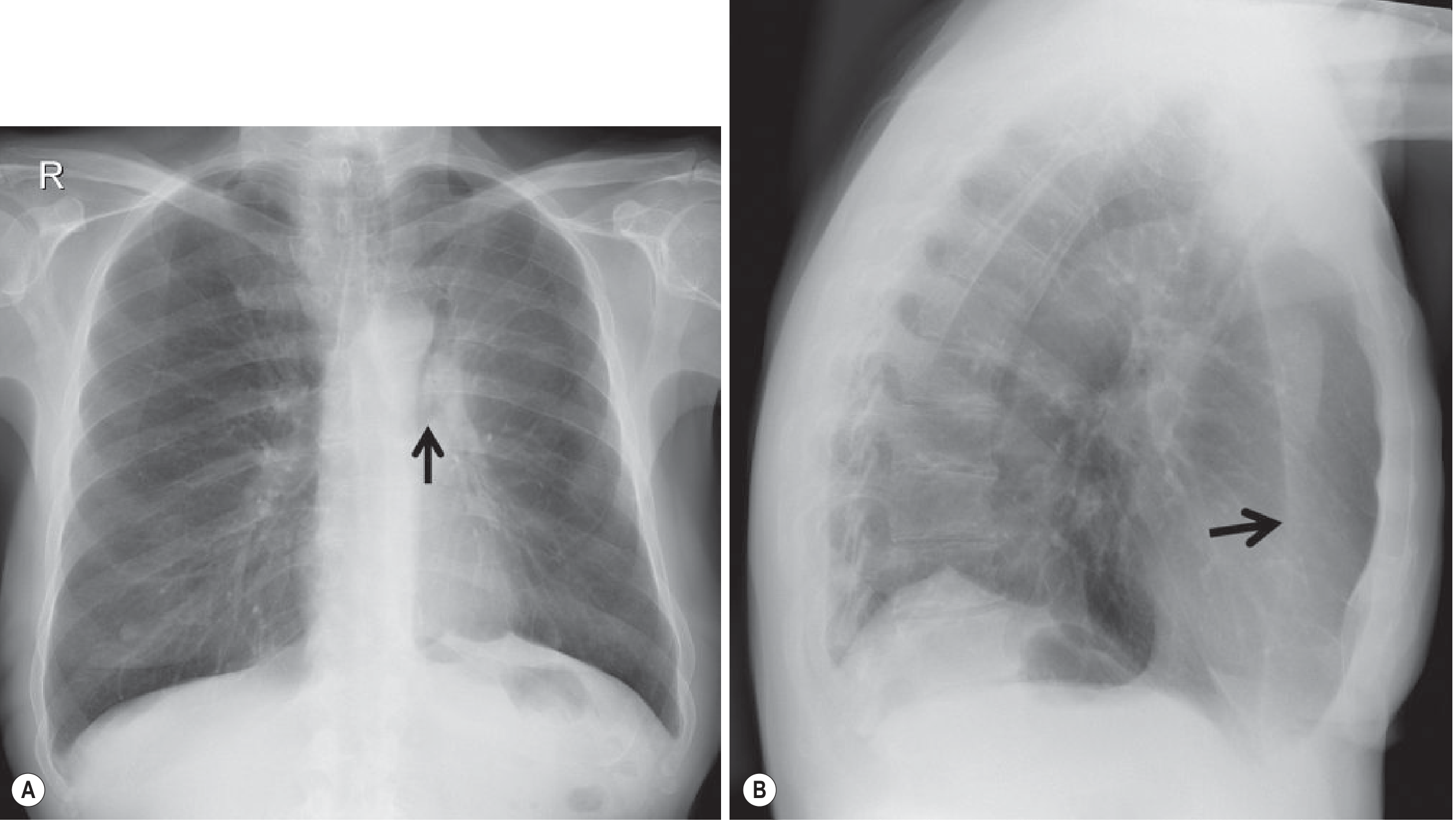
Fig. 7.21 (Grainger & Allison's) - Left Upper Lobe Collapse: (A) PA - increased angulation of left main bronchus (arrow), aortic knuckle visible due to LLL hyperinflation. (B) Lateral - anterior displacement of oblique fissure (arrow) with increased retrosternal lucency
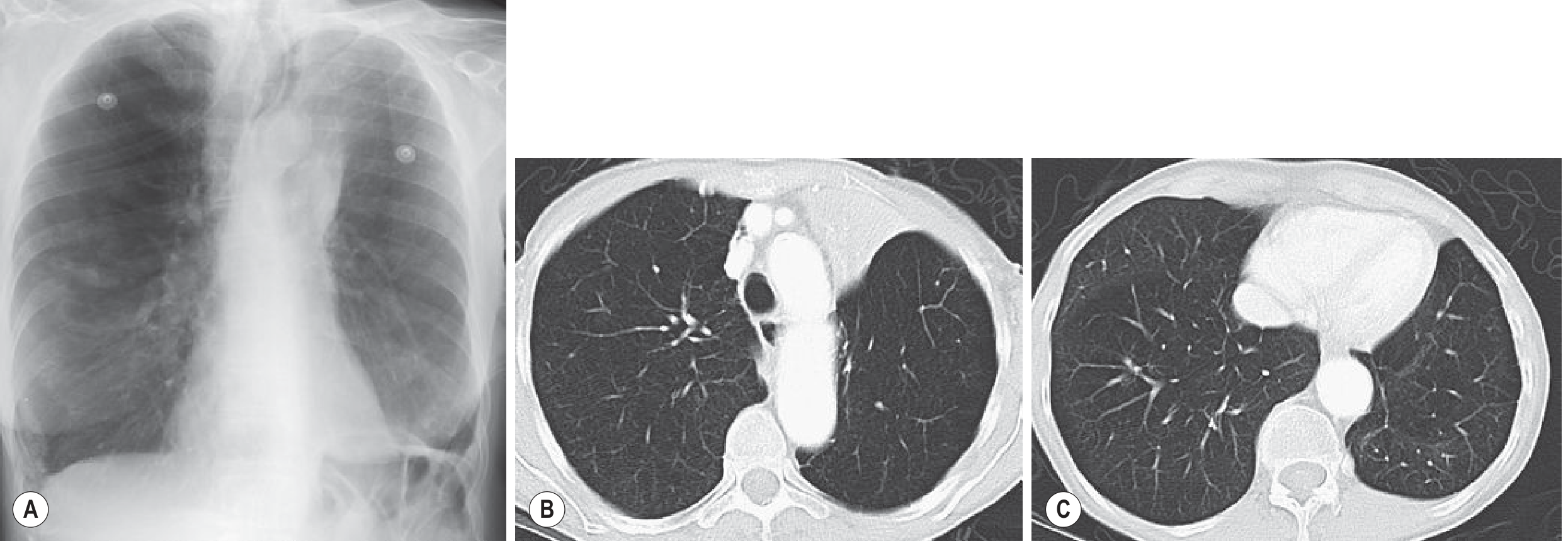
Fig. 7.22 (Grainger & Allison's) - Atypical Left Upper Lobe Collapse with lingular sparing: (A) Frontal X-ray mimics RUL collapse. (B, C) CT shows triangular density left of mediastinum that does not extend along the left heart border - confirming LUL collapse with spared lingula
5. Left Lower Lobe (LLL) Collapse
X-Ray Findings:
- Frontal: Triangular density behind the heart (left-sided equivalent of RLL collapse). The medial left hemidiaphragm outline is lost (silhouette sign). The descending aorta outline may be preserved.
- Flat waist sign: With extensive LLL collapse, there is flattening of the contours of the aortic knuckle and main pulmonary artery due to cardiac rotation/displacement.
- Lateral: Increased density posteriorly; loss of the left hemidiaphragm posteriorly. Vertebral column appears progressively denser inferiorly (opposite of normal where upper vertebrae are denser).
CT Findings:
- Collapsed lobe lies posteromedially in left hemithorax
- Descending thoracic aorta may create a focal bulge in the contour of the collapsed lobe (Fig. 7.13)
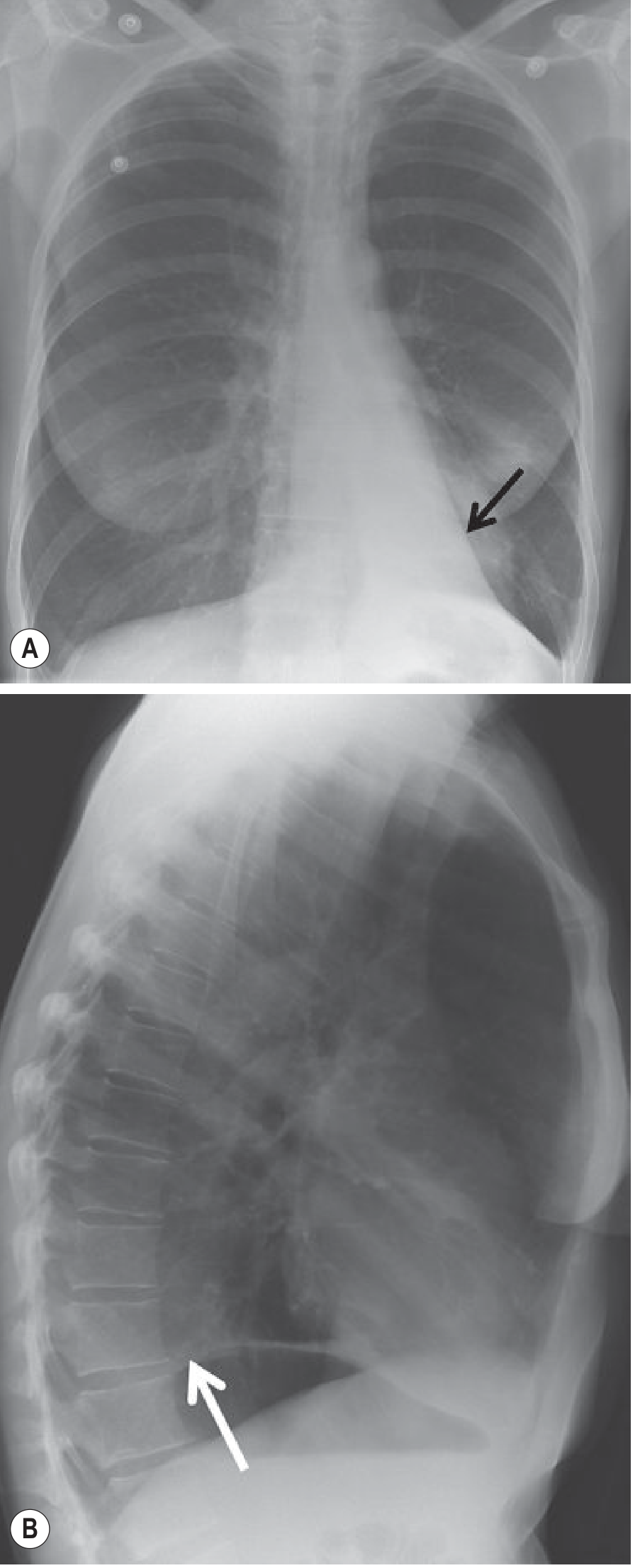
Fig. 7.28 (Grainger & Allison's) - Left Lower Lobe Collapse: (A) Frontal - triangular density behind heart (arrow), medial left hemidiaphragm lost. (B) Lateral - posterior increased density and loss of left hemidiaphragm posteriorly
CT: Special Signs & Advantages
| CT Sign | Significance |
|---|---|
| CT mucous bronchogram | Tubular low-attenuation airways within an enhancing lobe - suggests obstructive cause |
| Dense homogeneous enhancement | Atelectatic lung enhances brightly (vs. pneumonia which enhances poorly) - useful to differentiate |
| Luftsichel (air sickle) | Crescent of hyperaerated LLL around the aortic knuckle - pathognomonic of LUL collapse |
| Golden S sign | S-shaped fissure contour (RUL or LUL) = central mass causing collapse |
| Pita bread sign | Flat slab of LUL against anterior mediastinum on axial CT |
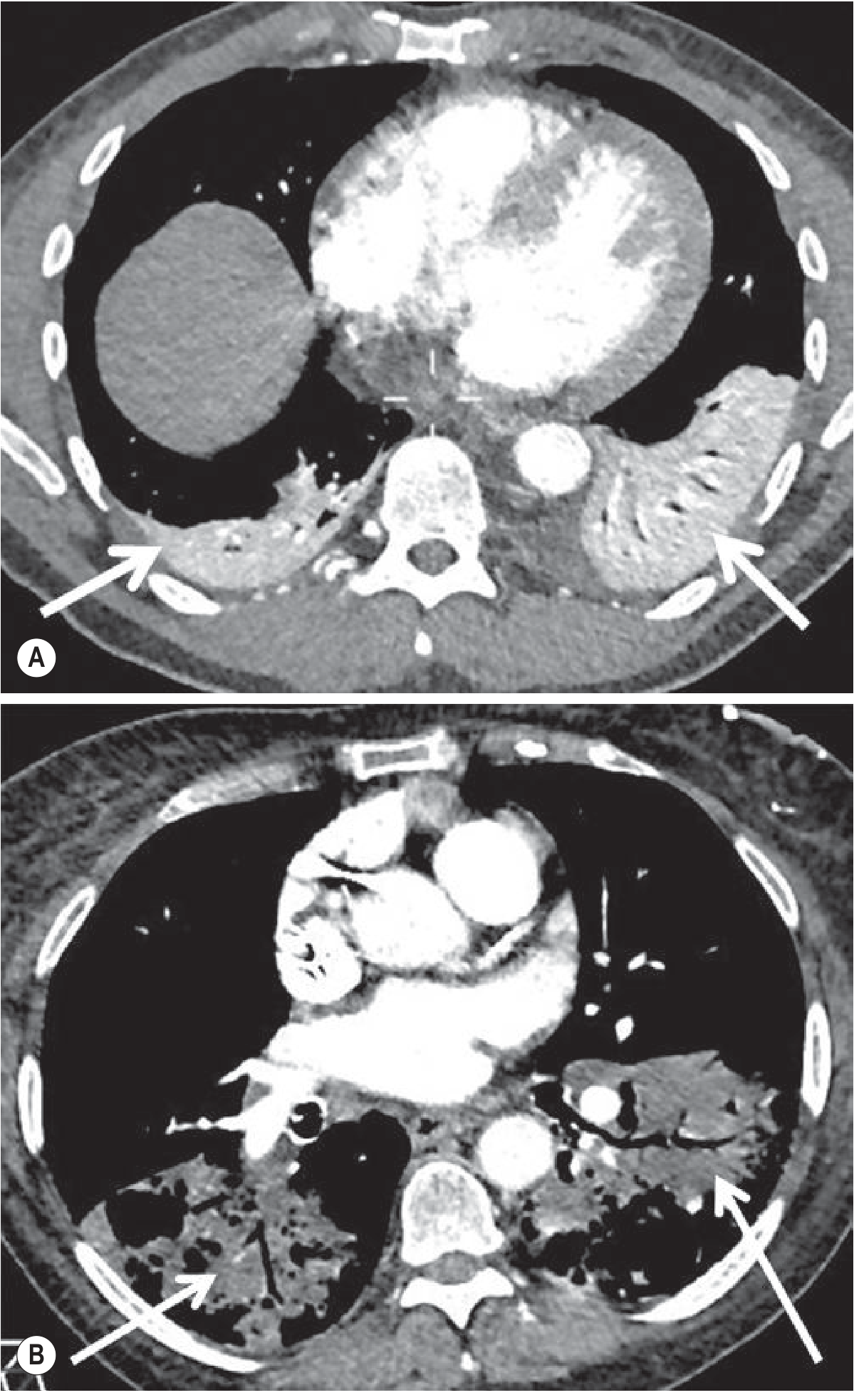
Fig. 7.12 (Grainger & Allison's) - Enhancement patterns: (A) Bilateral lower lobe atelectasis - dense homogeneous enhancement (arrows). (B) Bilateral lower lobe pneumonia - relative lack of enhancement with air bronchograms. This distinction is critical on CECT.
Quick Summary Table
| Lobe | Frontal X-ray | Lateral X-ray | CT |
|---|---|---|---|
| RUL | Opacity upper right zone, minor fissure pulled up, trachea deviates right, Golden S sign if mass | Anterior-superior opacity | Triangular wedge anterosuperiorly |
| RML | Hazy right heart border (silhouette sign), triangular density at heart border | Bowtie/triangular band between converging fissures | Flat triangular mass at right heart border |
| RLL | Triangular density behind heart/right diaphragm, lower lobe artery lost, superior triangle sign | Posterior CP angle opacity, posterior diaphragm lost | Posteromedial triangular opacity, mucous bronchogram |
| LUL | Veil opacity left upper zone, elevated hilum, Luftsichel crescent, silhouette of aortic knuckle/left heart border | Anteriorly displaced major fissure, retrosternal lucency | Anterior slab "pita bread" against mediastinum |
| LLL | Triangular density behind heart, medial hemidiaphragm lost, flat waist sign | Posterior opacity, posterior diaphragm lost, vertebrae denser inferiorly | Posteromedial triangular opacity |
A detailed video walkthrough of all lobar collapses with real radiographs:
Sources: Grainger & Allison's Diagnostic Radiology (7th Ed.); Goldman-Cecil Medicine; Springer Nature Journal of Medical Imaging 2024
This is a shared conversation. Sign in to Orris to start your own chat.