A 28-year-old farmer was brought to the hospital emergency department in an unconscious state. The family members stated that he was found collapsed in his agricultural field. On clinical examination, the patient was sweating profusely, salivating heavily, and had bilateral, pinpoint, non-reacting pupils. His breathing was laboured with a distinct, pungent, garlic-like odour coming from his breath. a) Identify the most likely poison and classify it based on its mechanism of action. b) Explain the mechanism of action of this poison that leads to these clinical signs. c) Describe the management and antidote regimen required to treat this patient. d) Describe the post-mortem findings if the patient succumbed to this poisoning. e) Explain how you would differentiate this condition from Acute Morphine poisoning based on clinical findings. (2 + 4 + 4 + 2 + 3 = 15)
Organophosphate Poisoning - Complete Answer
a) Identify the Poison and Classify It (2 marks)
- Farmer found collapsed in an agricultural field
- Profuse sweating (diaphoresis) and heavy salivation
- Bilateral pinpoint, non-reacting pupils (miosis)
- Laboured breathing (bronchospasm/bronchorrhea)
- Garlic-like odour from breath - a characteristic hallmark of organophosphate compounds (due to the sulfur-containing aromatic ring in compounds like parathion)
- Class Ia (extremely hazardous): Parathion, aldicarb
- Class Ib (highly hazardous): Methyl parathion, monocrotophos
- Class II (moderately hazardous): Malathion, chlorpyrifos
b) Mechanism of Action Explaining Clinical Signs (4 marks)
1. Muscarinic effects (parasympathetic/exocrine glands) - "SLUDGE/DUMBELS"
| Sign in Case | Mechanism |
|---|---|
| Profuse salivation | ACh on M3 receptors in salivary glands |
| Diaphoresis (sweating) | ACh on muscarinic receptors in eccrine sweat glands |
| Bilateral pinpoint miosis | ACh on M3 of iris sphincter - causes constriction |
| Laboured breathing | Bronchospasm (M3) + bronchorrhea (M2/M3) - airway obstruction |
| Unconsciousness (indirect) | Hypoxia from respiratory failure + CNS effects |
2. Nicotinic effects (neuromuscular junction + sympathetic ganglia)
- Muscle fasciculations, weakness, and eventually paralysis
- Tachycardia, hypertension (early nicotinic stimulation before muscarinic dominates)
- Skeletal muscle respiratory paralysis contributes to laboured breathing
3. Central effects (CNS cholinergic receptors)
- Anxiety, confusion, seizures, coma (unconscious state in this patient)
- Central respiratory depression worsening the already compromised breathing
c) Management and Antidote Regimen (4 marks)
Step 1 - Decontamination
- Remove all contaminated clothing; wash skin thoroughly with soap and water
- Protect healthcare workers: use gloves, protective suits, face masks (Level C PPE)
- Gastric lavage is of limited value once symptoms have begun (rapid absorption)
- Activated charcoal not routinely recommended if already symptomatic
Step 2 - Stabilisation and Supportive Care
- Airway first: Suction secretions; intubate if needed
- Prefer rocuronium 1 mg/kg (non-depolarising) for rapid-sequence intubation - avoid succinylcholine (metabolised by cholinesterases; prolonged paralysis of 4-6 hours in OP poisoning)
- Mechanical ventilation if respiratory failure
- IV access, continuous cardiac monitoring, pulse oximetry
- Benzodiazepines (diazepam/lorazepam) for seizures and agitation
- Correct metabolic acidosis and electrolyte imbalances
Step 3 - Antidote 1: ATROPINE (muscarinic antagonist)
- Initial dose: 2-4 mg IV (0.05 mg/kg in children); double dose every 5 minutes
- In severe poisoning: 10-20 mg in first hour; some cases require 200-500 mg in the first hour
- Endpoint ("atropinisation"): Drying of secretions, easing of respiratory effort, heart rate >80/min
- Once stabilised, give 10-20% of total loading dose per hour as infusion
- Tachycardia and mydriasis at therapeutic doses are expected - do NOT stop atropine for these
- Atropine does not reverse the underlying AChE inhibition
Step 4 - Antidote 2: PRALIDOXIME (2-PAM) - AChE reactivator
- Adult dose: 1-2 g IV over 15-30 minutes; repeat in 1 hour if needed; then 0.5 g/h infusion
- Must be given EARLY - before "aging" of the phosphoryl-AChE bond occurs (within minutes to hours, varies by compound)
- Less effective for some agents (e.g., dimethoate) where aging is rapid
- Pralidoxime reverses nicotinic effects (fasciculations, muscle weakness) that atropine cannot
Step 5 - Additional measures
- Benzodiazepines for seizure control (OP-related seizures do not respond well to phenytoin)
- Monitor RBC cholinesterase and plasma cholinesterase levels
- Watch for intermediate syndrome (24-96 hours post-acute phase): proximal limb weakness, neck flexor weakness, respiratory paralysis - does not respond to atropine/pralidoxime
d) Post-mortem Findings (2 marks)
- Body odour: garlic-like smell (characteristic)
- Excessive secretions from mouth and nostrils (frothy fluid)
- Cyanosis of lips and nail beds (from hypoxia/respiratory failure)
- Miosis (pinpoint pupils) persists after death
- Skin: may show evidence of contact dermatitis at exposure sites
- Lungs: Pulmonary oedema and congestion (most prominent finding) - frothy fluid in airways from bronchorrhea; features of aspiration pneumonia may be present
- Brain: Cerebral oedema with petechial haemorrhages (anoxic encephalopathy)
- Heart: Subepicardial and subendocardial haemorrhages; evidence of hypoxic myocardial damage
- Stomach: Garlic-like smell on opening; corrosive erosions/haemorrhagic gastritis if ingested directly
- Liver and kidneys: Congestion and degenerative changes from hypoxia
- Visceral congestion throughout
- Muscle necrosis (particularly respiratory muscles)
- Neuronal degeneration in the brain
- Reduced or absent RBC cholinesterase and plasma cholinesterase activity in blood
- Detection of OP compound or its metabolites in gastric contents, blood, urine, liver
e) Differentiation from Acute Morphine Poisoning (3 marks)
| Feature | Organophosphate Poisoning | Acute Morphine Poisoning |
|---|---|---|
| Pupils | Pinpoint, non-reacting (bilaterally fixed) | Pinpoint, but reactive to light (preserved light reflex) |
| Secretions | Profuse - salivation, lacrimation, bronchorrhea, diaphoresis | Dry - no excessive secretions; skin dry |
| Sweating | Profuse diaphoresis (hallmark muscarinic effect) | Absent or minimal |
| Breath odour | Garlic/petroleum-like odour (OP compound) | No characteristic odour |
| Muscle activity | Fasciculations, twitching, muscle weakness | Flaccidity, no fasciculations |
| Bowel sounds | Hyperactive (increased GI motility, diarrhea) | Decreased/absent (opioids cause constipation and ileus) |
| Bradycardia | Present (muscarinic effect) | Present (also bradycardia common) |
| Bronchospasm | Severe (life-threatening bronchorrhea + bronchospasm) | Mild respiratory depression (CNS-mediated, not bronchospasm) |
| Response to naloxone | No response | Dramatic reversal of unconsciousness, miosis, and respiratory depression |
| Response to atropine | Dramatic improvement in secretions, breathing | No response |
| Skin | Wet, sweaty | Dry |
| Needle marks | Absent (agricultural exposure) | May be present (IV drug use) |
| History | Exposure to insecticides/agricultural chemicals | History of opioid use or access to narcotics |
| GI symptoms | Vomiting, diarrhea, cramps | Nausea/vomiting (but constipation more common) |
| Seizures | Common | Rare (except meperidine/tramadol) |
Which bed side chemical tests do you prefer to confirm the clinical diagnosis? How that test is performed and its interpretation? 4mrk Explain why mydriasis is not the therapeutic end point of Atropinisation 4mrk What will be your duties in the management in this case? (6 Marks) Identify the chemical class of the poison and explain its biochemical mechanism of action on the human.3 mrk
bedside chemical test organophosphate poisoning atropine challenge test spot test performance interpretation
mydriasis not therapeutic endpoint atropinisation organophosphate poisoning why pupil dilation unreliable
Complete Answers - Organophosphate Poisoning (Continued)
1. Bedside Chemical Tests to Confirm the Diagnosis (4 marks)
A. Atropine Challenge Test (Clinical Bedside Test)
- Establish baseline vitals: heart rate, pupil size, skin moisture, secretions
- Administer 1 mg of atropine IV (some protocols use 0.6-1 mg IV)
- Observe the patient for 15-20 minutes
- Note: No premedication or other anticholinergics should be given before the test
- Positive test (OP poisoning likely): No anticholinergic features appear at this dose - no mydriasis, no tachycardia, no drying of secretions, no flushing. The cholinergic excess from OP poisoning neutralises the small atropine dose. The patient requires therapeutic atropine.
- Negative test (OP poisoning unlikely): Classical anticholinergic features appear - tachycardia (HR >120/min), mydriasis, dry mouth, flushing - indicating normal or near-normal AChE activity.
- False-negative possible in very severe poisoning (may require much higher doses)
- Results must be interpreted alongside clinical context
B. Spot Test for Cholinesterase Inhibition (Dithiobisnitrobenzoic acid / Ellman's test - rapid colorimetric)
- Collect a few drops of whole blood or serum on filter paper
- Apply the reagent substrate (acetylthiocholine + DTNB)
- Observe colour development within a few minutes
- Normal result: Bright yellow colour develops (enzyme is active, hydrolysis occurring)
- Positive for OP poisoning: No or pale yellow colour (enzyme is inhibited, no hydrolysis)
- The degree of colour inhibition correlates roughly with severity of poisoning
- Plasma (pseudo) cholinesterase (BuChE): Drops first in acute poisoning; recovers in 4-6 weeks. Less specific (also low in liver disease, malnutrition)
- RBC acetylcholinesterase (true AChE): More specific; recovers in 12 weeks. Better marker of severity
In practice in Indian emergency departments, the atropine challenge test is the most accessible bedside test as it requires no special equipment and provides an immediate therapeutic decision.
2. Why Mydriasis is NOT the Therapeutic Endpoint of Atropinisation (4 marks)
Reason 1 - Atropine only blocks MUSCARINIC receptors; the pupil involves additional pathways
Reason 2 - The lethal effect is bronchospasm + bronchorrhea, not miosis
Reason 3 - Mydriasis can appear prematurely (over-atropinisation)
- Stop dosing prematurely - bronchorrhea and bronchospasm persist, patient dies of respiratory failure
- Or conversely, chase mydriasis with excessive doses, causing atropine toxicity: hyperthermia, agitation, delirium, urinary retention, ileus, dangerous tachyarrhythmias
Reason 4 - Atropine does NOT reverse nicotinic effects
The Correct Endpoint of Atropinisation:
- Drying of secretions (most important - clear breath sounds, no bronchorrhea)
- Easing of respiratory effort, normalisation of respiratory rate
- Heart rate >80/min (but tachycardia alone should not stop dosing)
- Adequate oxygenation
- NOT: mydriasis, flushing, dry skin - these are signs of over-atropinisation
"The endpoint of atropinisation is drying of respiratory secretions, easing of respiratory effort, and normalisation of respiratory rate." - Rosen's Emergency Medicine, 10th Ed.
3. Duties of a Doctor in the Management of This Case (6 marks)
A. Clinical Duties (Treatment Duties)
- Immediate stabilisation (ABC): Secure airway, give oxygen, establish IV access, connect cardiac monitor and pulse oximetry
- Decontamination: Instruct nursing staff to remove all contaminated clothing; flush skin with soap and water; protect healthcare workers with gloves/PPE
- Administer antidotes: Start atropine IV immediately with escalating doses (1-3 mg, doubling every 5 min until secretions dry); add pralidoxime 1-2 g IV as early as possible
- Supportive care: Intubate if respiratory failure (use rocuronium, not succinylcholine); ventilatory support; treat seizures with benzodiazepines
- Monitoring: Continuously monitor HR, BP, SpO2, RR, GCS, pupil size, skin moisture; send blood for RBC cholinesterase, ABG, blood glucose, electrolytes, renal and liver function
- Watch for intermediate syndrome: Alert clinical staff to watch for delayed onset (24-96 h) proximal limb/respiratory weakness
B. Medico-Legal Duties
-
Notification/Reporting: Poisoning cases (especially agricultural and suicidal) are medico-legally significant. The doctor must:
- Inform the police as per local law (Section 174 CrPC in India requires notification of suspicious/unnatural illness)
- Send an MLC (Medico-Legal Case) report to the jurisdictional police
- Document everything accurately and contemporaneously in the case records
-
Documentation: Record a detailed history of the circumstances of the case (as given by family - "found collapsed in field"), time of discovery, clinical findings, investigations ordered, treatment given with doses and timing, response to treatment, and condition on admission in the case notes
-
Preservation of evidence: Collect and label specimens for forensic/toxicological analysis:
- Blood (for cholinesterase assay, toxicology screen)
- Urine (metabolites of OP compounds)
- Gastric lavage contents/vomitus (if ingested)
- Send specimens to FSL (Forensic Science Laboratory) under proper chain of custody (sealed, labelled, countersigned)
-
Statement to police (Section 39 CrPC): Cooperate with police if they arrive to record the patient's statement or conduct inquiry; do not obstruct investigation
-
Dying declaration (if patient is in extremis): If the patient regains consciousness and is lucid but death is anticipated, the doctor must facilitate and witness a dying declaration in the presence of a magistrate, which carries evidentiary value in legal proceedings
-
Maintain confidentiality while fulfilling statutory reporting obligations; do not disclose information to media or unauthorised persons
4. Chemical Class and Biochemical Mechanism of Action (3 marks)
Chemical Class
- Phosphates: e.g., TEPP (tetraethyl pyrophosphate)
- Phosphorothioates (thion): e.g., parathion, malathion (P=S; activated in vivo to P=O oxon form by cytochrome P450 - the oxon is the active AChE inhibitor)
- Phosphoramidates: e.g., methamidophos
Biochemical Mechanism of Action
- Normally: ACh binds → ACh is hydrolysed → enzyme is regenerated (in microseconds)
- With OP: The phosphoryl bond is stable and does not hydrolyse spontaneously → enzyme permanently blocked
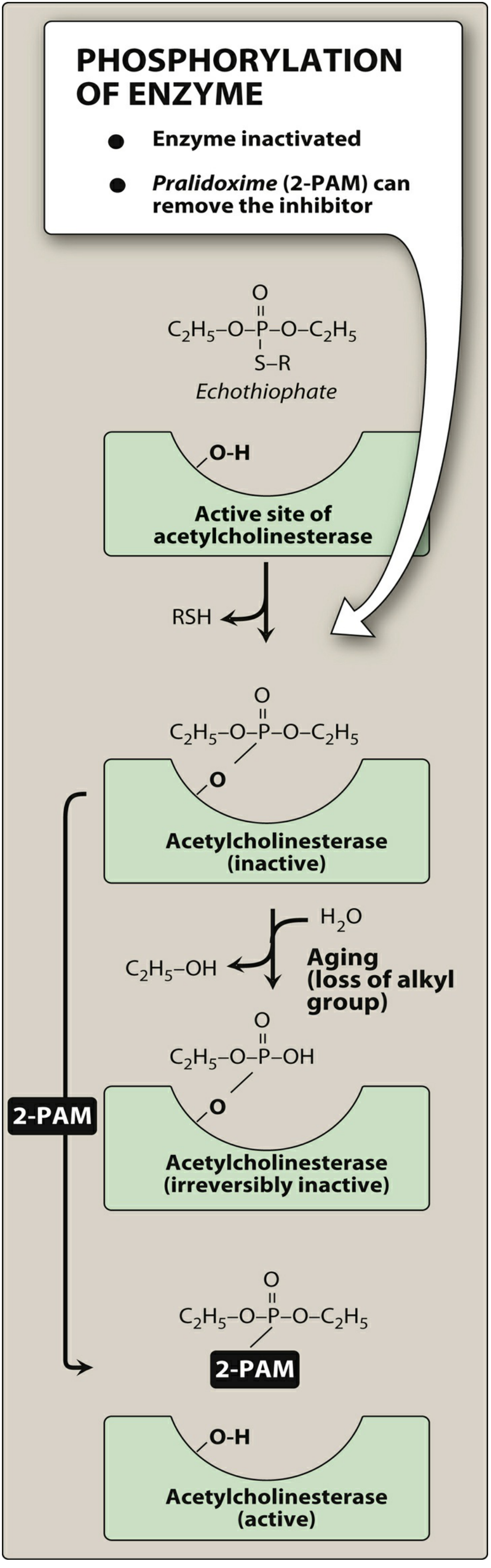
| Step | Normal AChE | OP-inhibited AChE |
|---|---|---|
| Substrate binding | ACh binds serine | OP binds serine (covalent) |
| Hydrolysis | ACh split in microseconds | No hydrolysis - bond stable |
| Enzyme fate | Regenerated immediately | Inactivated (irreversible after aging) |
| ACh fate | Destroyed | Accumulates - continuous stimulation |