Factors responsible for Lens transparency
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I now have sufficient information from the textbooks to give a thorough, well-structured answer.
Factors Responsible for Lens Transparency
The lens is one of the most optically clear tissues in the body. Its transparency depends on several interrelated structural, biochemical, and physiological factors.
1. Unique Structural Organization of Lens Fibers
Lens fibers are highly elongated, terminally differentiated cells (7-10 mm long, ~2 x 8 µm cross-section) that are packed tightly together in a precise, regular arrangement. This regular packing prevents light scattering. During maturation, each lens fiber:
- Fills its cytoplasm with crystallin proteins
- Undergoes autophagy of all organelles and the nucleus
- Loses all intracellular membrane-bound structures
The absence of nuclei, mitochondria, ribosomes, and other organelles in mature lens fibers (the mature lens fiber zone, MLF) eliminates internal scattering interfaces, which is a key physical requirement for transparency.

2. Crystallin Proteins
Crystallins are a specialized group of structural proteins that fill the cytoplasm of lens fibers. They account for >90% of the total lens protein and are responsible for:
- Maintaining a uniform refractive index across the lens
- Short-range order: Crystallins are organized at high concentration but in a way that minimizes light scattering at short distances
- Stability: They are extremely long-lived proteins; once laid down, they are not replaced
The two main families are alpha-crystallins (which also function as molecular chaperones, preventing aggregation of damaged proteins) and beta/gamma-crystallins (structural proteins). With aging or stress, crystallins can denature and aggregate, scattering light and causing cataract.
3. Avascularity
The lens is entirely avascular - it contains no blood vessels. This is essential because:
- Blood vessels themselves scatter light
- The absence of vasculature removes the optical heterogeneity that would otherwise disrupt the passage of light
Nutrition is delivered entirely via diffusion from the aqueous humor (anteriorly) and vitreous humor (posteriorly).
4. Absence of Connective Tissue
The lens contains no connective tissue elements (collagen fibers, fibroblasts, etc.) within its substance. These would create optical interfaces that scatter light. The only extracellular matrix present is the lens capsule - a type IV collagen/proteoglycan basement membrane that surrounds the lens externally and does not interfere with the light path.
5. Ion and Water Homeostasis (Pump-Leak System)
The lens maintains precise control of its intracellular water content through the "pump-leak" mechanism:
- Na⁺/K⁺-ATPase on the anterior epithelium actively pumps Na⁺ out and K⁺ in, maintaining osmotic balance
- Aquaporin-0 (MIP26) water channels in lens fiber membranes regulate water flux
- Gap junctions (connexins 46 and 50) facilitate intercellular communication and ion/metabolite circulation between lens fibers
Disruption of this balance (e.g., influx of aqueous humor through a capsular rupture) causes hydration of lens fibers and opacification - the basis of traumatic cataract.
6. Antioxidant Defense Systems
The lens is exposed to cumulative oxidative stress from UV radiation and metabolic byproducts. Several antioxidant systems protect protein integrity:
- Glutathione (GSH): Present in very high concentrations; neutralizes reactive oxygen species (ROS) and maintains protein -SH groups in the reduced state, preventing disulfide cross-linking and protein aggregation
- Ascorbic acid (Vitamin C): Present in aqueous humor; acts as a UV filter and antioxidant
- Superoxide dismutase, catalase, glutathione peroxidase: Enzymatic antioxidant defenses
- Alpha-crystallin (chaperone function): Binds and suppresses aggregation of oxidatively damaged proteins
Depletion of glutathione with age or disease is a major pathway to cataract formation. - Robbins & Kumar Pathologic Basis of Disease
7. Anaerobic Metabolism (Low Oxygen Tension)
The lens is maintained in a low-oxygen environment. It relies predominantly on anaerobic glycolysis (the hexose monophosphate shunt and Embden-Meyerhof pathway) for energy. This minimizes ROS generation from mitochondrial oxidative phosphorylation. The lens also uses the sorbitol (polyol) pathway, which, when overactive (e.g., in diabetes mellitus), causes sorbitol accumulation, osmotic swelling, and cataract.
8. Lens Epithelium Integrity
The single-layered cuboidal lens epithelium on the anterior surface:
- Serves as the metabolic "powerhouse" of the lens (contains all mitochondria)
- Maintains ion gradients and water balance
- Serves as the source of new lens fiber cells (cells at the equator divide and differentiate into lens fibers throughout life)
Fibrous metaplasia of the lens epithelium (e.g., from posterior synechiae in uveitis) directly causes anterior subcapsular cataract.
Summary Table
| Factor | Mechanism of Transparency |
|---|---|
| Regular fiber packing | Minimizes light scattering |
| Crystallin proteins | Uniform refractive index; chaperone activity |
| Avascularity | No optical interfaces from blood vessels |
| No organelles in mature fibers | Eliminates intracellular scattering |
| Ion/water pump-leak system | Prevents excess hydration |
| Antioxidant systems (GSH, Vit C) | Prevents protein oxidation/aggregation |
| Anaerobic metabolism | Minimizes ROS generation |
| Intact lens epithelium | Maintains metabolic homeostasis |
Clinical relevance: Any factor that disrupts these mechanisms leads to cataract. Common causes include aging (crystallin denaturation, GSH depletion), diabetes mellitus (sorbitol accumulation), UV radiation (oxidative damage), corticosteroids (posterior subcapsular cataract), and trauma (capsular rupture with aqueous influx).
- Junqueira's Basic Histology, 17e
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Kanski's Clinical Ophthalmology, 10th ed.
Factors responsible for corneal transparency
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook coverage from three authoritative sources. Here is the full answer:
Factors Responsible for Corneal Transparency
The cornea is the most powerful refracting surface of the eye (~43 D of its ~60 D total power) and must be perfectly transparent. It is only 0.5 mm thick centrally and 1 mm peripherally, yet achieves near-complete transparency through a combination of structural, cellular, biochemical, and physiological factors.
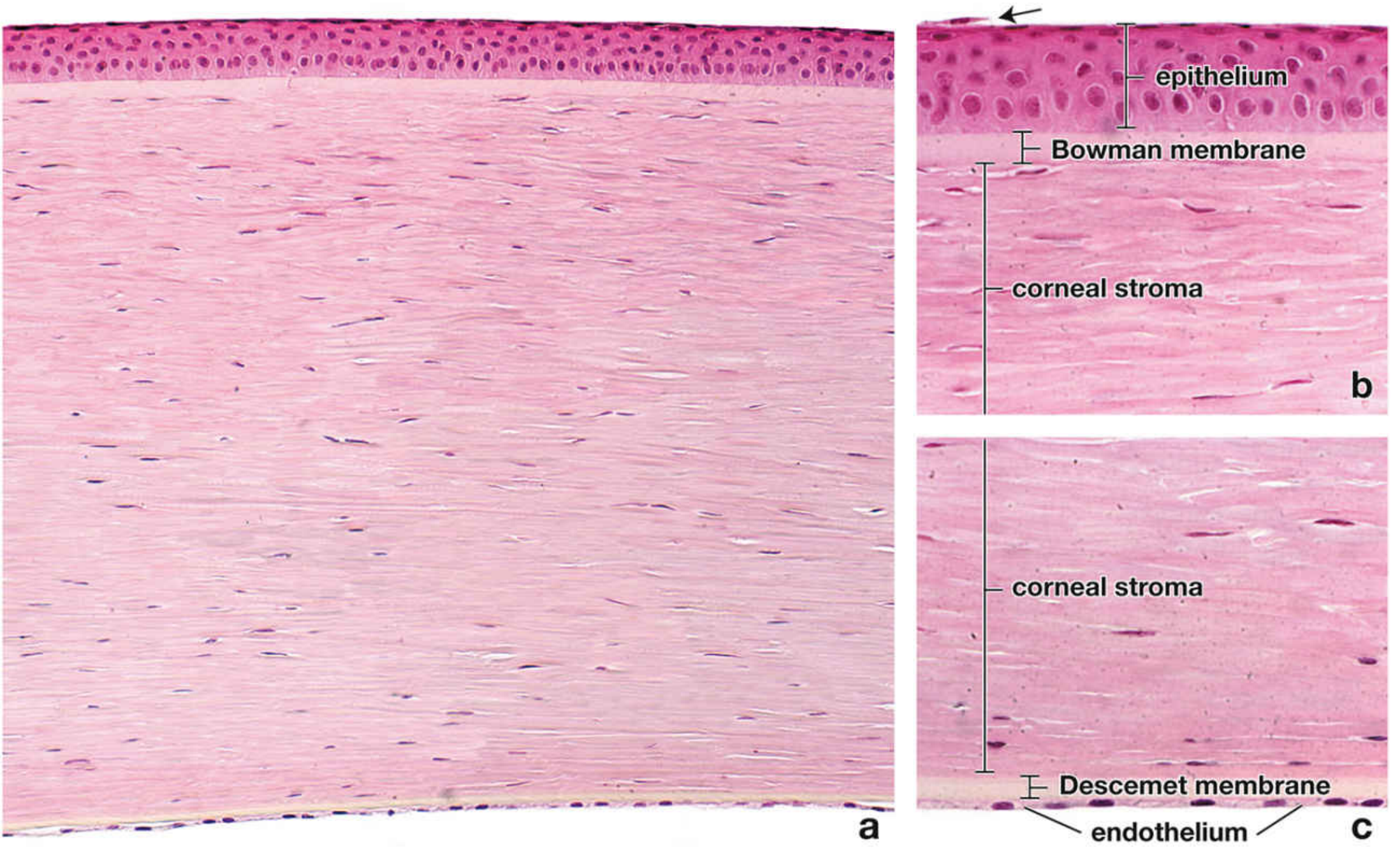
1. Precise Organization of Stromal Collagen (Most Important Factor)
The stroma constitutes 90% of corneal thickness and is the primary determinant of transparency. Its key features:
- Composed of approximately 60 thin lamellae, each made of parallel bundles of type I collagen fibrils
- Adjacent lamellae are oriented at right angles to each other (orthogonal array)
- Collagen fibrils are remarkably uniform in diameter (~23 nm) and uniformly spaced
- Fibrils are as long as 1 cm but have a diameter far smaller than the wavelength of visible light
The critical principle: Corneal transparency is achieved because the spaces between collagen fibrils are smaller than one-half the wavelength of visible light (~200-225 nm). When inter-fibrillar spaces are smaller than λ/2, destructive interference of scattered light waves occurs, canceling out scattering - and the tissue becomes transparent. In contrast, the sclera is opaque precisely because its collagen bundles are irregular in diameter and arrangement, preventing this destructive interference.
2. Proteoglycans Regulating Collagen Fibril Spacing
The ground substance of the corneal stroma contains small leucine-rich proteoglycans (SLRPs) with sulfated glycosaminoglycans:
- Lumican (keratan sulfate proteoglycan) - the most important; regulates normal collagen fibril assembly, maintains the highly organized collagenous matrix, and controls fibril diameter and spacing
- Decorin (chondroitin sulfate proteoglycan) - contributes to fibril organization
These proteoglycans physically separate and space the collagen fibrils at precise intervals. Additionally, type V collagen (present in a much higher ratio than in other tissues) works with lumican to regulate the precise diameter of type I collagen fibrils. Loss or disruption of these proteoglycans (e.g., in corneal swelling) causes collagen fibrils to aggregate, expanding inter-fibrillar spaces beyond λ/2, and producing opacification.
3. Stromal Deturgescence - Active Dehydration (Endothelial Pump)
The stroma has a natural tendency to imbibe water (due to the hydrophilic glycosaminoglycans). Transparency requires that this hydration be precisely controlled - a state called deturgescence.
Two epithelia work together to maintain this:
Corneal Endothelium (posterior surface)
- Forms a leaky barrier between the stroma and the anterior chamber
- Aqueous humor passively leaks paracellularly into the stroma (providing nutrients)
- Endothelial cells actively pump ions (Na⁺/K⁺-ATPase on lateral membranes) from the stromal fluid back into the anterior chamber, drawing water with it
- The endothelial cells are rich in mitochondria, reflecting their high metabolic (pumping) activity
- Loss or damage to endothelial cells (e.g., Fuchs' endothelial dystrophy, surgical trauma) immediately causes stromal edema, collagen fibril aggregation, and corneal opacification
- Human corneal endothelium has very limited regenerative capacity - severely damaged endothelium can only be repaired by corneal transplantation
Corneal Epithelium (anterior surface)
- Acts as a physical barrier - prevents evaporation of fluid from the stroma and protects from external damage
- Contributes to stromal deturgescence by preventing excess water entry from the tear film
- Damage to the epithelium (e.g., trauma, dry eye) allows fluid ingress, swelling, and temporary haziness
4. Avascularity
The corneal stroma contains no blood vessels or lymphatics. This is critical for two reasons:
- Optical: Blood vessel walls and red blood cells scatter light; their absence eliminates these interfaces
- Immune privilege: Avascularity limits access of immune cells and antibodies, which is why corneal transplantation has a high success rate. The risk of graft rejection increases when stromal vascularization occurs (e.g., from chronic inflammation or contact lens abuse)
Corneal nutrition is maintained entirely by diffusion - from aqueous humor (posteriorly), tears (anteriorly), and the limbal capillaries peripherally.
5. Absence of Pigment
The normal cornea contains no pigment cells or melanin. Pigment absorbs and scatters light. (Contrast: the choroid and retinal pigment epithelium contain melanin specifically to absorb scattered light posteriorly, but the cornea must remain free of pigment in the optical path.)
6. Smooth Anterior Surface - The Tear Film
The cornea's exposed anterior surface, while microscopically smooth, is made perfectly smooth optically by the tear film:
- The mucin layer (from goblet cells) keeps the film adherent to the corneal epithelium
- The aqueous layer provides a smooth refracting surface
- The lipid layer (from meibomian glands) prevents evaporation
Without an intact tear film, even a structurally normal cornea scatters light (as seen in severe dry eye).
7. Corneal Epithelium - Non-keratinized, Non-pigmented
The non-keratinized stratified squamous corneal epithelium (~50 µm, ~5 cell layers) is:
- Non-keratinized: Keratinized epithelium (like skin) is opaque due to keratin accumulation; the corneal epithelium specifically avoids this
- Has tight junctions (zonulae occludentes) at the surface, providing a barrier
- Rapid turnover (~7 days) with stem cells from the corneolimbal junction ensures constant renewal and maintenance of a smooth, intact surface
8. Acellularity of Bowman's Layer
Bowman's membrane (anterior basement membrane) is an acellular, condensed zone of the anterior stroma. Its acellularity and homogeneous collagen structure prevent light scattering at the epithelium-stroma interface. It also acts as a barrier against penetration of cells (e.g., malignant epithelial cells) into the stroma. Unlike Descemet membrane, Bowman's layer does not regenerate after injury - damage leaves a scar.
Why the Sclera is Opaque (Contrast)
The sclera immediately illustrates what makes the cornea transparent by contrast: scleral collagen bundles are irregular in diameter and cross at multiple angles, so inter-fibrillar spaces vary widely and exceed λ/2, producing the characteristic white opacity. The stroma directly continues into sclera at the limbus, but the precise organization is immediately lost.
Summary Table
| Factor | Mechanism |
|---|---|
| Uniform collagen fibril diameter & spacing | Inter-fibrillar spaces < λ/2 of visible light → destructive interference of scattered rays |
| Orthogonal lamellar arrangement | Regular short-range order minimizes scattering |
| Proteoglycans (lumican, decorin) + type V collagen | Regulate fibril diameter and maintain precise spacing |
| Endothelial pump (Na⁺/K⁺-ATPase) | Active deturgescence - prevents stromal hydration |
| Corneal epithelium barrier | Prevents excess water ingress and evaporation |
| Avascularity | No blood vessel optical interfaces |
| Absence of pigment | No absorption/scattering by melanin |
| Smooth tear film | Corrects minor surface irregularities |
| Non-keratinized epithelium | Avoids opaque keratin deposition |
| Acellular Bowman's layer | No cell scattering at epithelium-stroma interface |
Key clinical correlations:
-
Corneal edema (endothelial failure): excess water expands inter-fibrillar spaces → opacity (Fuchs' dystrophy, bullous keratopathy)
-
Corneal scarring: disrupts regular collagen alignment → permanent opacity
-
Corneal vascularization (trachoma, contact lens hypoxia): introduces light-scattering structures
-
Keratoconus: irregular collagen organization → distorted refraction and haziness
-
Wilson disease: copper deposits in Descemet membrane form the Kayser-Fleischer ring - visible at the limbus but can affect transparency
-
Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina)
-
Medical Physiology (Boron & Boulpaep)
-
Robbins, Cotran & Kumar - Pathologic Basis of Disease
-
Kanski's Clinical Ophthalmology, 10th ed.
This is a shared conversation. Sign in to Orris to start your own chat.