Tuberculosis types with xray and findings
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I have all the key images and content I need. Now let me compile the comprehensive answer.
Tuberculosis: Types, X-ray Findings & Radiological Features
Overview - Natural History
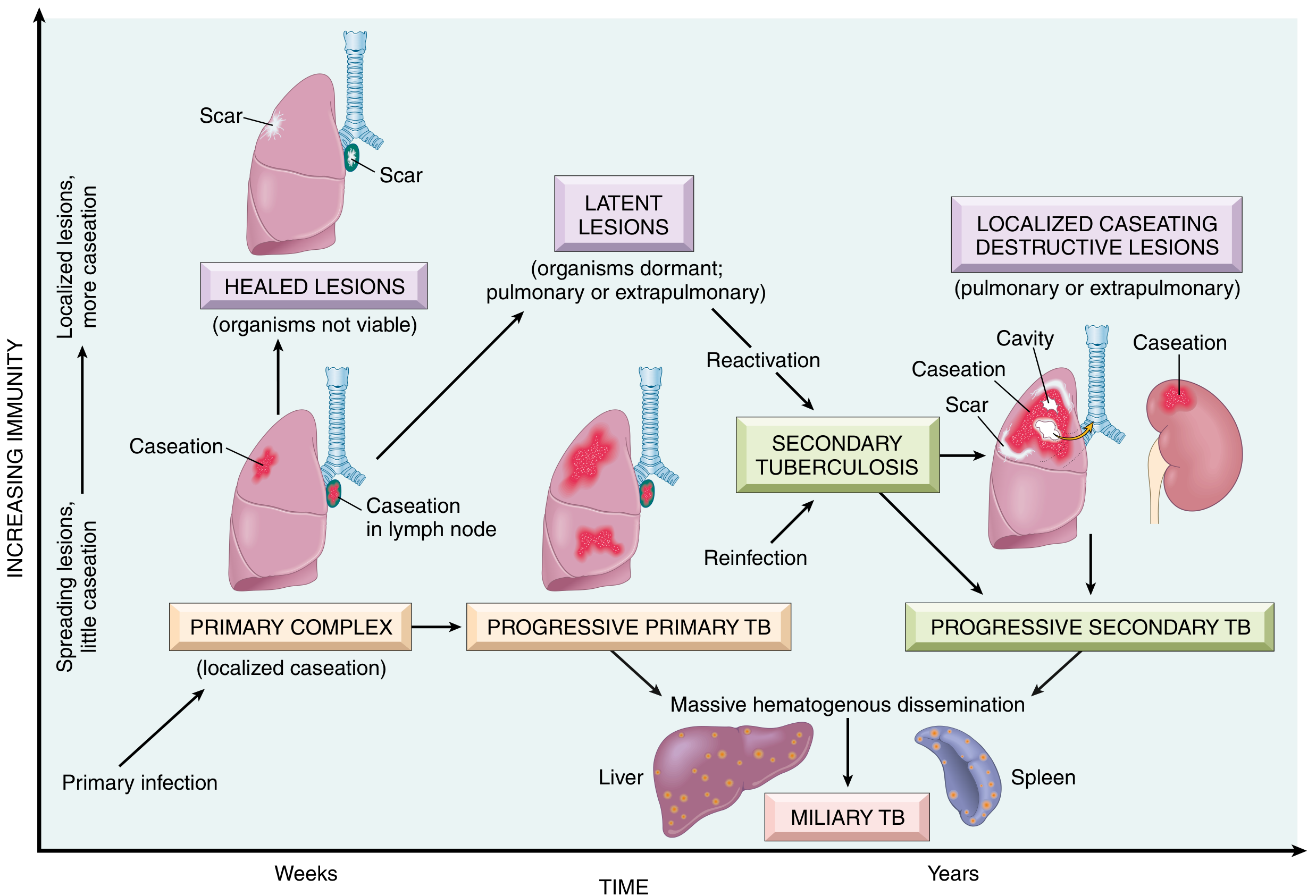
The natural history of TB - Primary Complex → Progressive Primary TB / Latent Lesions → Secondary (Reactivation) TB / Miliary TB (from Robbins & Kumar Basic Pathology)
1. Primary Tuberculosis
Definition: Results from the initial infection with Mycobacterium tuberculosis in a host with no prior immunity.
Pathology
- The inhaled bacilli settle in the mid/lower lung zones and form the Ghon focus (area of consolidation).
- Draining lymphatics carry bacilli to the ipsilateral hilar nodes → together these form the Ghon complex (primary complex).
- In most immunocompetent individuals, the infection is controlled; the lesions undergo caseous necrosis, calcification, and scarring.
- If immunity fails to contain it → Progressive Primary TB (see below).
Chest X-ray Findings
- Middle or lower lung zone opacity/consolidation (unlike reactivation TB, which is upper lobe)
- Ipsilateral hilar/paratracheal lymphadenopathy - this is the most characteristic feature
- Possible pleural effusion
- Possible atelectasis from lymph node compression of airways
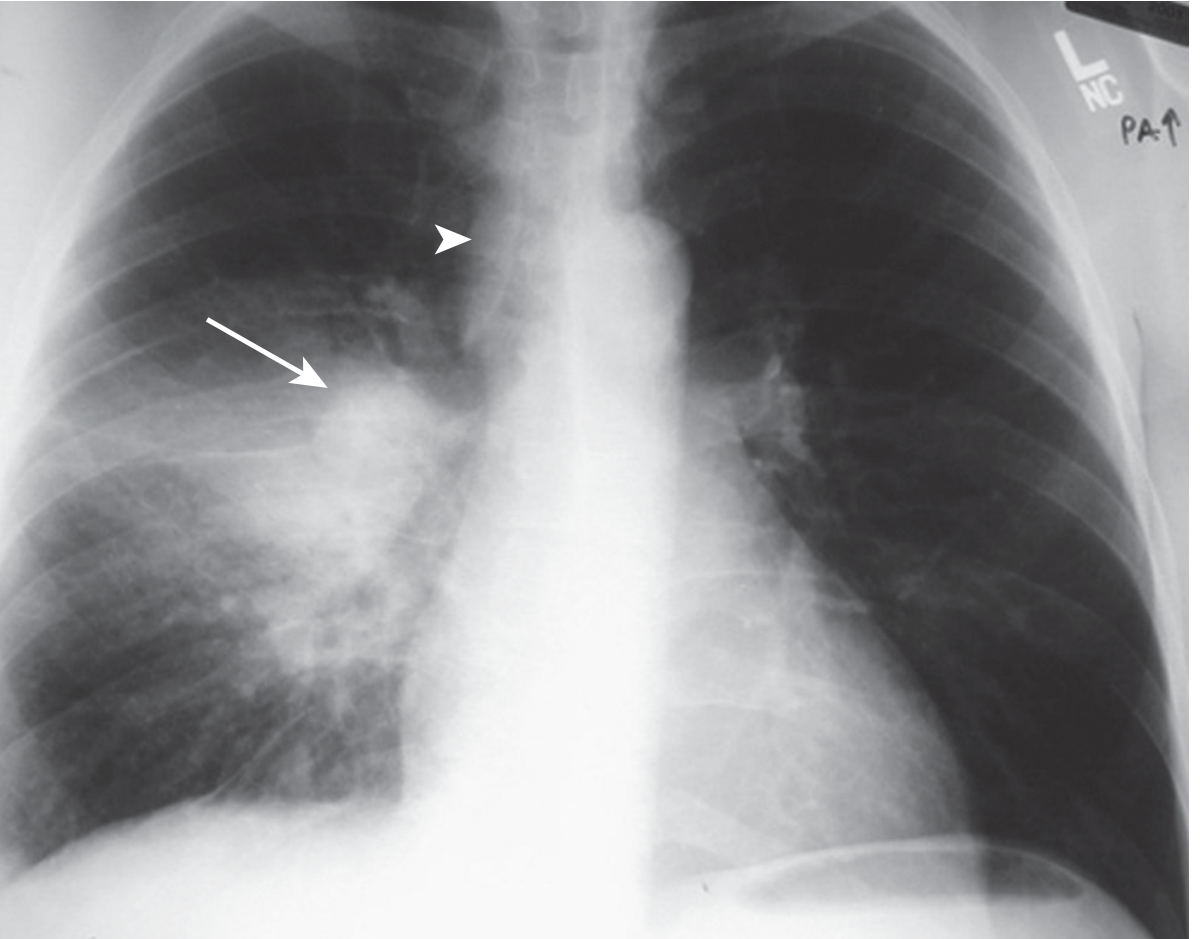
Figure 53.1 - Primary TB: Right lower lobe consolidation + right hilar lymphadenopathy (arrow) + right paratracheal lymph node enlargement (arrowhead). (Murray & Nadel's Respiratory Medicine)
From Grainger & Allison (shown below), primary TB in a child with hilar adenopathy:
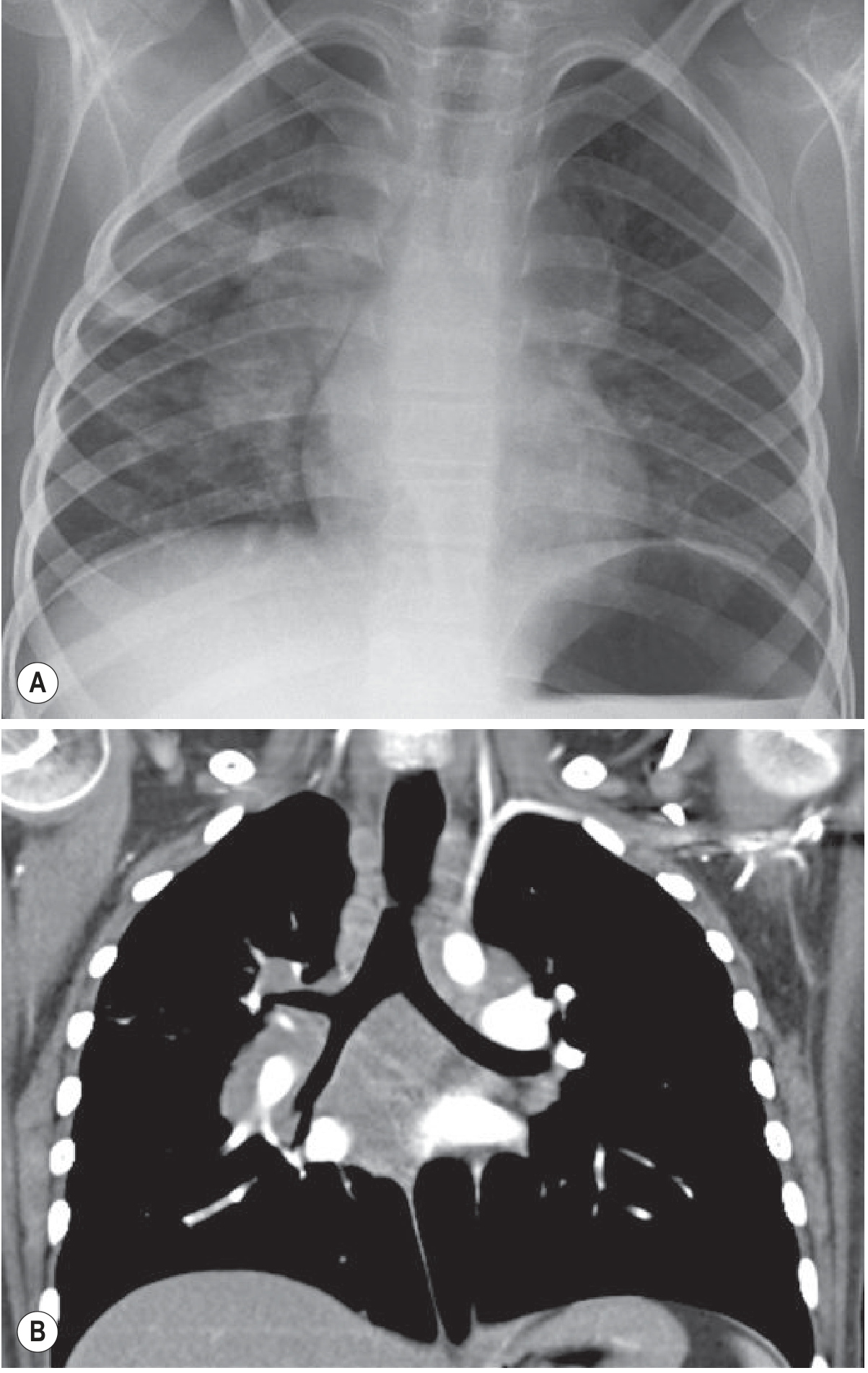
Fig. 70.28 Primary Tuberculosis - CXR (A) and coronal CT (B) demonstrating hilar adenopathy. (Grainger & Allison's Diagnostic Radiology)
2. Progressive Primary Tuberculosis
Definition: Primary infection that fails to be contained by developing cell-mediated immunity. More common in children, the elderly, and immunosuppressed.
X-ray Findings
- Rapidly enlarging pulmonary consolidation (lobar pattern)
- Cavitation can form in the primary focus
- Prominent hilar/mediastinal adenopathy
- May be indistinguishable from acute bacterial lobar pneumonia
3. Secondary (Reactivation) Tuberculosis
Definition: Develops when a previously infected individual undergoes reactivation of latent TB - either spontaneously (due to waning immunity) or through reinfection. This is the most common form in adults.
Pathology
- Reactivation driven by falling cell-mediated immunity (HIV, malnutrition, steroids, DM, old age, TNF inhibitors)
- Localizes to the lung apices because of higher oxygen tension there
- Hallmark: caseous necrosis with cavity formation
- Bronchogenic spread can carry infected material to other parts of the lung
Chest X-ray Findings
- Upper lobe involvement - predominantly apical and posterior segments of the right upper lobe (most common site), also apical-posterior segment of the left upper lobe
- Cavitation - thick-walled cavities, often in the upper lobes (highly characteristic)
- Fibronodular or patchy consolidation
- Volume loss and fibrosis with superior hilar retraction (old healed disease)
- Calcifications in healed lesions (Ranke complex)
- Bronchogenic spread pattern: new acinar/nodular opacities ("tree-in-bud") in ipsilateral lower lobe or contralateral lung
- Absence of hilar adenopathy (in contrast to primary TB)
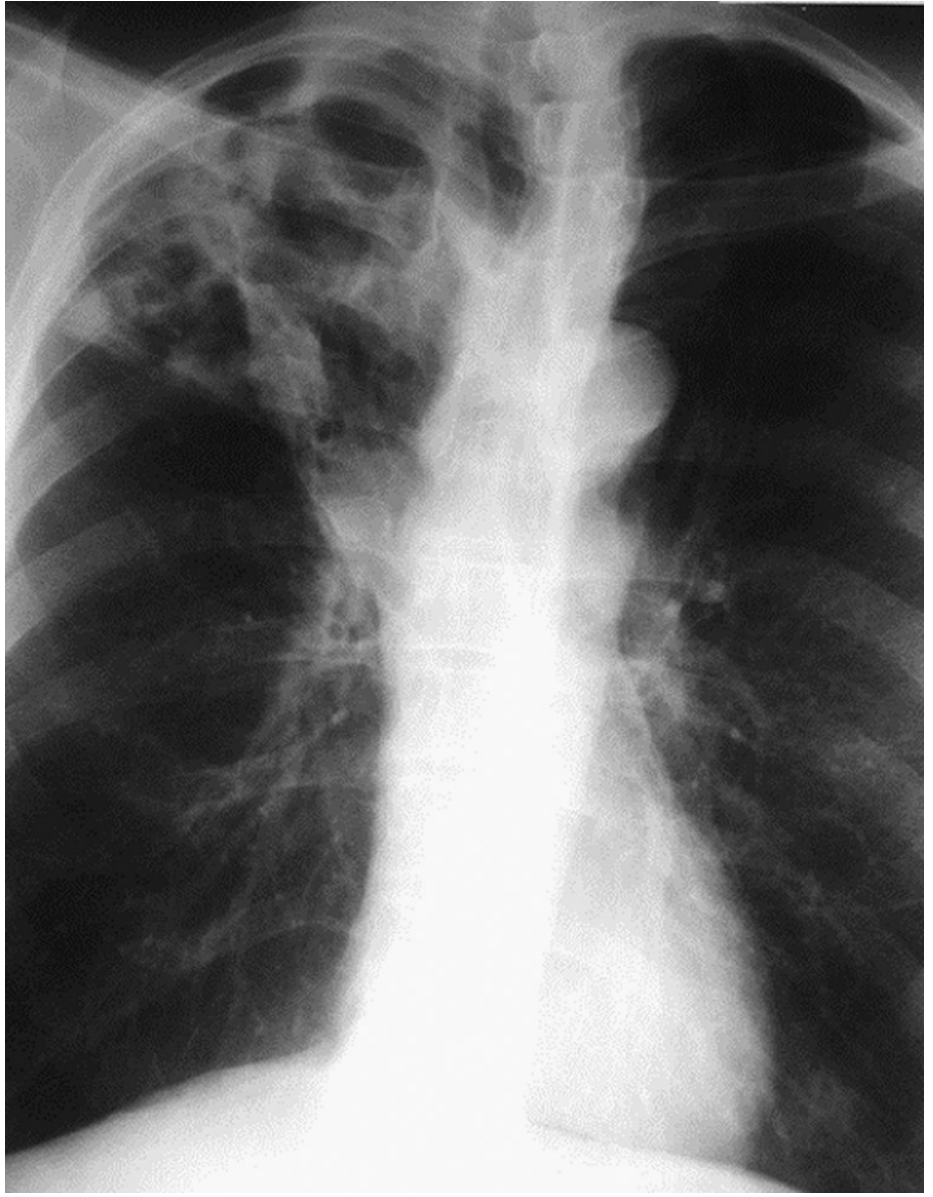
Figure 53.2 - Cavitary (Reactivation) TB: Extensive right upper lobe cavitation. (Murray & Nadel's Respiratory Medicine)
4. Miliary Tuberculosis
Definition: Results from massive hematogenous dissemination of M. tuberculosis - can occur as a complication of either primary or reactivation TB. The term "miliary" comes from the radiographic appearance resembling millet seeds (1-5 mm each).
At-risk groups
Children, elderly, immunocompromised (HIV, organ transplant, corticosteroids). Mortality rate is 20-30%.
Chest X-ray Findings
- Diffuse, bilateral, uniformly distributed tiny nodules (1-3 mm) throughout both lung fields
- Nodules are randomly distributed - no zone predilection
- "Snow-storm" or "millet seed" appearance
- May be subtle early on; CT is far more sensitive

Figure 53.3 - Miliary TB: Numerous small, randomly distributed bilateral nodules ("miliary pattern"). (Murray & Nadel's Respiratory Medicine)
5. Tuberculosis in HIV/Immunocompromised Patients
The radiographic pattern depends on the degree of CD4 depletion:
| CD4 count | Pattern |
|---|---|
| Early HIV (CD4 relatively preserved) | Typical pattern - upper lobe infiltrates, cavitation |
| Advanced HIV (low CD4 / AIDS) | Atypical pattern - lower zone or diffuse opacities, prominent hilar/mediastinal adenopathy, NO cavitation |
| Some HIV patients | Normal chest radiograph despite active TB |
X-ray Findings (Advanced HIV)
- Bilateral hilar lymphadenopathy (prominent, unlike immunocompetent reactivation)
- Diffuse nodular or consolidative opacities
- Lower lung zone involvement
- Cavitation uncommon
- Pleural effusion more frequent
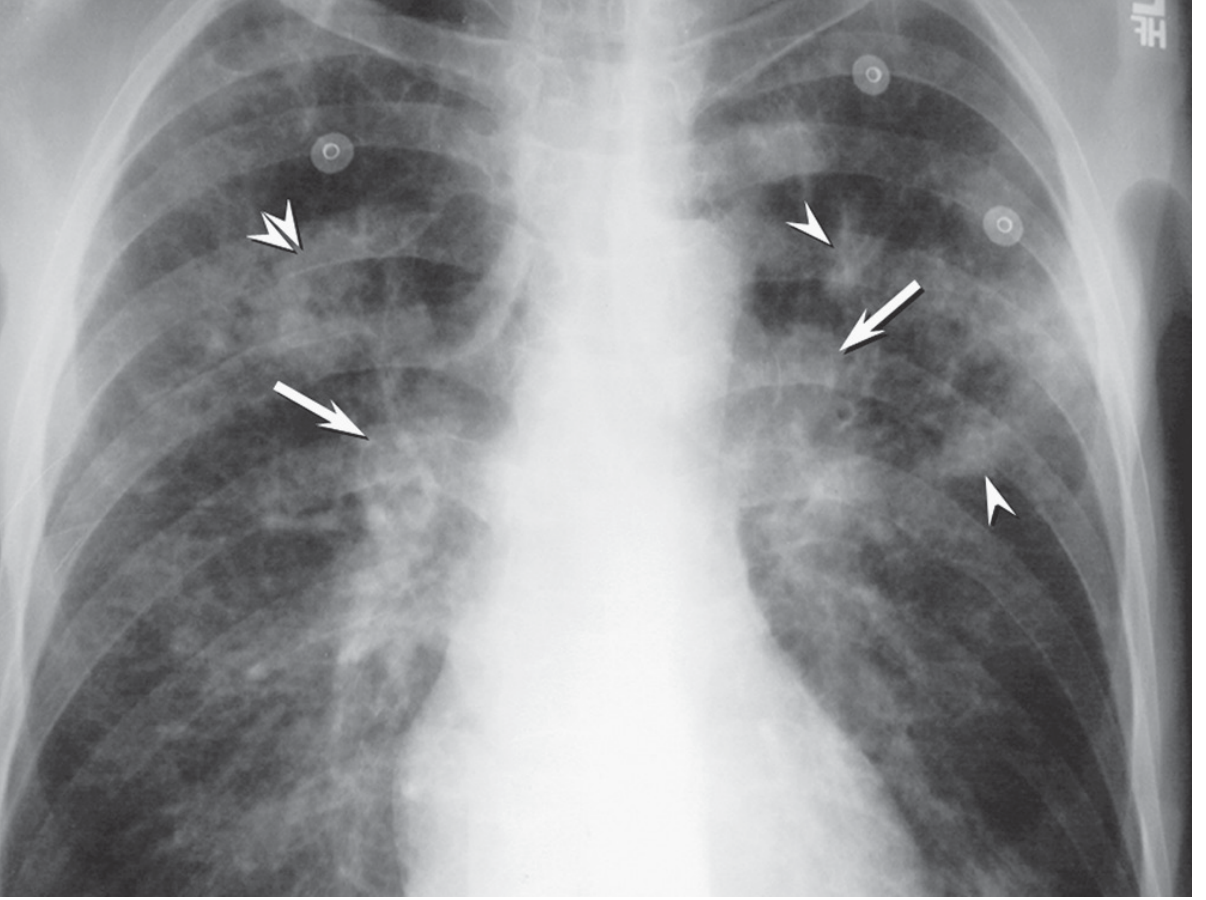
Figure 53.4 - TB + HIV: Bilateral hilar lymph node enlargement (arrows) + nodular opacities (arrowheads) + nodular consolidation (double arrowheads). (Murray & Nadel's Respiratory Medicine)
Summary Table
| Type | Location on CXR | Key Feature | Adenopathy | Cavitation |
|---|---|---|---|---|
| Primary TB | Mid/lower zones | Consolidation + hilar LN | Yes (ipsilateral) | Rare |
| Progressive Primary | Any zone, lobar | Rapid consolidation | Yes | Sometimes |
| Latent TB | Normal | No active lesion | No | No |
| Reactivation (Secondary) TB | Upper lobes (apical/posterior) | Cavitary fibronodular | Absent | Common |
| Miliary TB | Diffuse bilateral | 1-3 mm nodules ("millet seeds") | Variable | No |
| TB + HIV | Lower zones / diffuse | Atypical infiltrates | Yes (bilateral) | Uncommon |
Additional Radiological Notes
- Ranke complex: Calcified primary focus (Ghon focus) + calcified hilar lymph node = healed primary TB
- Simon foci: Small calcified apical nodules representing early hematogenous seeding - can reactivate years later
- CT advantages: Sensitivity 96% vs 48% for plain CXR in active TB. CT better detects lymphadenopathy, "tree-in-bud" pattern (bronchogenic spread), and cavity walls.
- "Tree-in-bud" sign on CT: Centrilobular nodules connected by branching linear densities - highly suggestive of endobronchial spread of TB.
- Activity cannot be determined from a single CXR alone - a cavity may be a sterile old lesion, and a fibrotic-appearing area may be active.
Sources: Murray & Nadel's Textbook of Respiratory Medicine, Grainger & Allison's Diagnostic Radiology, Robbins & Kumar Basic Pathology, Goldman-Cecil Medicine, Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.