Pulmonary Edema
Reading File
Finding Sources
Searching PubMed
"pulmonary edema"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
pulmonary edema chest X-ray radiograph
Reading File
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile a comprehensive answer.
Pulmonary Edema
Definition
Pulmonary edema is the abnormal accumulation of fluid in the extravascular spaces of the lung — initially in the pulmonary interstitium, and in severe cases flooding the alveoli. It results when any factor increases fluid filtration out of pulmonary capillaries or impedes lymphatic drainage, causing interstitial fluid pressure to rise from the negative range into the positive range. — Guyton and Hall Textbook of Medical Physiology
Classification & Causes
Pulmonary edema is broadly divided into two categories: — Robbins Pathologic Basis of Disease
1. Hemodynamic (Cardiogenic) Pulmonary Edema
Caused by increased hydrostatic pressure:
- Left-sided heart failure (most common) — elevated pulmonary venous pressure drives fluid into interstitium
- Mitral valve disease (stenosis or regurgitation)
- Volume overload (e.g., CKD/ESRD, aggressive IV fluids)
- Pulmonary vein obstruction
Decreased oncotic pressure (less common):
- Hypoalbuminemia (nephrotic syndrome, liver disease, protein-losing enteropathies)
Lymphatic obstruction (rare)
2. Increased Permeability (Noncardiogenic) Pulmonary Edema
Caused by microvascular or epithelial injury:
| Mechanism | Examples |
|---|---|
| Direct lung injury | Bacterial pneumonia, inhaled gases (O₂ toxicity, smoke), aspiration of gastric contents, near-drowning, radiation, trauma |
| Indirect (systemic) | Sepsis (SIRS), burns, pancreatitis, extensive trauma, blood transfusion-related |
| Drugs/chemicals | Bleomycin, methadone, amphotericin B, heroin, cocaine, paraquat |
| Other | High altitude, neurogenic (CNS trauma/SAH) |
3. Mixed/Special Forms
- Neurogenic pulmonary edema — follows subarachnoid hemorrhage; autonomically mediated increased pulmonary arterial pressure and vascular permeability
- High-altitude pulmonary edema (HAPE) — increased capillary permeability at altitude
- Negative-pressure pulmonary edema — after acute upper airway obstruction
Pathophysiology
Starling Forces & Safety Factors
Pulmonary capillary pressure normally must rise to at least equal the plasma colloid osmotic pressure (~25–28 mmHg) before significant edema occurs. With a normal capillary pressure of ~7 mmHg, the acute safety factor against pulmonary edema is approximately 21 mmHg.
In chronic elevations of pulmonary capillary pressure (≥2 weeks), lymphatic vessels expand their capacity up to 10-fold. Patients with chronic mitral stenosis may tolerate pressures of 40–45 mmHg without lethal edema. — Guyton and Hall
In acute left-sided heart failure, capillary pressure can reach 50 mmHg — death may occur within 30 minutes.
Sequence of Fluid Accumulation
- Interstitial space fills first (interstitial edema)
- Peribronchial cuffing and Kerley B lines develop
- Alveolar flooding occurs when interstitial capacity is overwhelmed
- Surfactant disruption → alveolar collapse
Pathology (Cardiogenic)
- Alveolar capillaries engorged; finely granular pale pink alveolar transudate
- Alveolar microhemorrhages → hemosiderin-laden macrophages ("heart failure cells")
- Chronic congestion → brown induration (firm, fibrotic lungs with abundant hemosiderin) — Robbins
ARDS (Severe Noncardiogenic)
Severe capillary-alveolar membrane injury destroys type II pneumocytes → loss of surfactant production → alveolar collapse. Releases secondary inflammatory mediators → pulmonary vasoconstriction, inhibited hypoxic vasoconstriction, alveolar flooding. An exudative phase may be followed by a fibrotic phase (fibrosing alveolitis). PaO₂:FiO₂ ratio ≤300 = acute lung injury; <200 = ARDS. — Morgan & Mikhail's Clinical Anesthesiology
Clinical Features
| Feature | Cardiogenic | Noncardiogenic (ARDS) |
|---|---|---|
| Onset | Hours (acute CHF) or gradual | Hours–days |
| Dyspnea | Orthopnea, PND, exertional | Severe, progressive |
| JVD / S3 | Often present | Absent |
| Dependent edema | Common | Absent |
| Frothy sputum | Pink, frothy | May be present |
| Hemodynamics | ↑ PCWP, ↓ CO | Normal/↓ PCWP |
| Response to diuretics | Rapid | Minimal |
Symptoms: Sudden dyspnea, orthopnea, paroxysmal nocturnal dyspnea (PND), cough with frothy pink sputum, anxiety, diaphoresis
Signs: Tachypnea, tachycardia, rales/crackles (bibasilar), wheeze ("cardiac asthma"), cyanosis, ↓ SpO₂
Signs: Tachypnea, tachycardia, rales/crackles (bibasilar), wheeze ("cardiac asthma"), cyanosis, ↓ SpO₂
Diagnosis
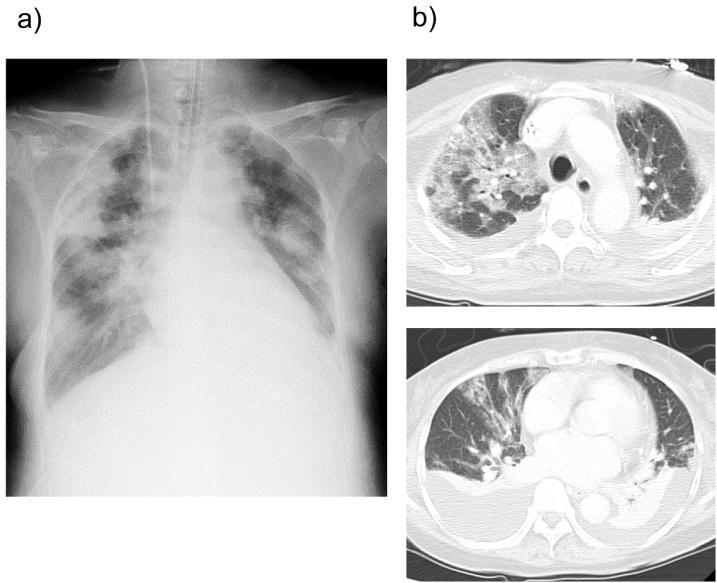
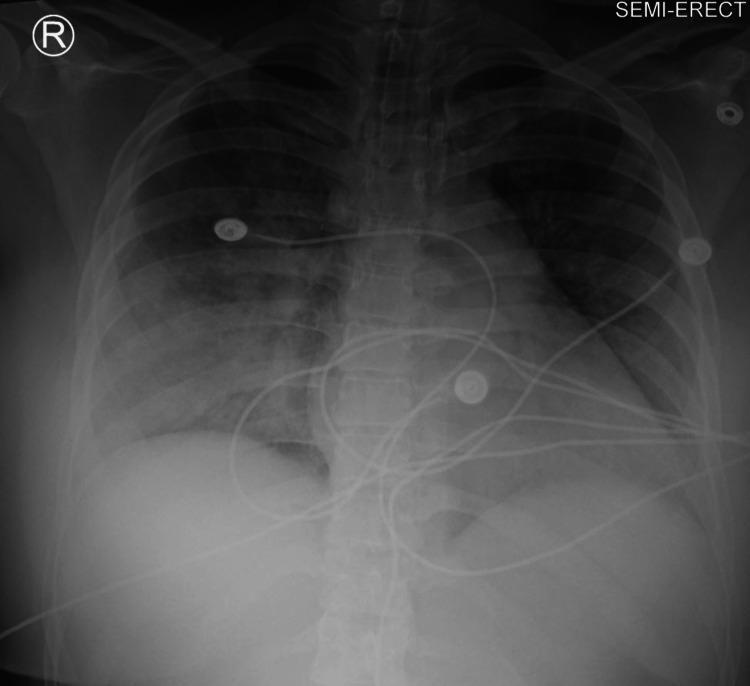
Chest Radiograph
Classic findings of cardiogenic pulmonary edema:
- Cardiomegaly (enlarged cardiac silhouette)
- Cephalization of pulmonary vasculature
- Kerley B lines (interstitial edema)
- Perihilar "bat-wing" or "butterfly" pattern — bilateral confluent alveolar opacities
- Pleural effusions (bilateral)
Point-of-Care Ultrasound (POCUS)
B-lines (≥3 per intercostal space) in bilateral lung zones — highly sensitive and specific for pulmonary edema. Recent systematic review (PMID: 40845678) supports POCUS utility for diagnosis.
Additional Workup
- BNP / NT-proBNP — markedly elevated in cardiogenic; helps differentiate from noncardiogenic
- ABG — hypoxemia ± hypocapnia (early); hypercapnia indicates respiratory fatigue/failure
- ECG — ischemia, arrhythmia, LVH
- Echo — LV/RV function, PCWP estimation, valvular disease
- Labs — CBC, BMP, troponin, LFTs, albumin
Treatment
General Emergency Principles
Immediate goals: preserve airway, ensure adequate oxygenation and ventilation, maintain blood pressure. — Murray & Nadel's Textbook of Respiratory Medicine
Position: Upright (sitting) — reduces preload and improves diaphragm excursion
Oxygen: High-flow O₂ to maintain SpO₂ >94%
Oxygen: High-flow O₂ to maintain SpO₂ >94%
Ventilatory Support
| Modality | Indication |
|---|---|
| CPAP / BiPAP (NIV) | First-line for cardiogenic pulmonary edema; reduces need for intubation, hasten improvement, reduce intubation rate |
| Invasive mechanical ventilation | Refractory hypoxemia, altered consciousness, respiratory failure; use low tidal volume (6 mL/kg IBW) + PEEP strategy in ARDS |
Pharmacotherapy for Cardiogenic Pulmonary Edema
1. Vasodilators (cornerstone of acute therapy):
- Nitrates (nitroglycerin) — most important; IV infusion starting 10–20 μg/min, titrate up; reduces preload (venodilation) and afterload (arteriolar dilation); lowers pulmonary capillary pressure within minutes. Sublingual nitroglycerin acts immediately
- Recent meta-analysis (PMID: 40506079) supports high-dose IV nitroglycerin for sympathetic crashing acute pulmonary edema
- Nitroprusside — mixed vasodilator; useful in severe hypertension with pulmonary edema
- Nesiritide — BNP analog; vasodilator; use with caution with loop diuretics (renal function)
2. Diuretics:
- Furosemide IV (typically 40–100 mg) — loop diuretic; initial vasodilatory effect (rapid), then diuresis decreases LV volume and PCWP
- Goal: Net negative fluid balance
- Caution: Avoid if hypotensive or cardiogenic shock (poor renal perfusion limits effect)
- Equivalent alternatives: bumetanide, torsemide, ethacrynic acid
3. ACE Inhibitors / ARBs: Afterload reduction; beneficial in systolic dysfunction
4. Inotropes (cardiogenic shock only):
- Dobutamine — β₁ agonist; increases contractility
- Dopamine — at higher doses for BP support
- Milrinone — phosphodiesterase inhibitor; reduces preload + afterload, increases contractility
- ⚠️ Long-term inotrope use increases mortality; reserved for bridge to transplant/device
Hypertensive Pulmonary Edema
Most patients have diastolic dysfunction and LV hypertrophy — afterload reduction is more important than diuresis. Vasodilators (IV nitrates, nicardipine, clevidipine) are mainstays. — Tintinalli's Emergency Medicine
Treatment in CKD/ESRD
- Hemodialysis is the definitive treatment for volume overload pulmonary edema in ESRD
- Initiate urgently; other measures are temporizing
- CPAP/BiPAP: effective adjunct
- Furosemide: only helpful if residual renal function present
- Peritoneal dialysis: too slow for acute pulmonary edema — Rosen's Emergency Medicine / Tintinalli's
ARDS / Noncardiogenic Management
- Treat underlying cause (sepsis, pneumonia, aspiration)
- Lung-protective ventilation: Tidal volume 6 mL/kg IBW, plateau pressure <30 cmH₂O, individualized PEEP
- Adjuncts for refractory hypoxemia: inhaled nitric oxide, inhaled prostacyclin, prone positioning
- Fluid management: conservative fluid strategy to reduce ongoing edema formation
- Avoid hyperoxia (FiO₂ ≤0.5 if achievable) — Morgan & Mikhail's Clinical Anesthesiology
Safety Factor Summary (Guyton)
| State | Approximate max tolerated PCWP |
|---|---|
| Acute (normal lymphatics) | ~28 mmHg |
| Chronic (dilated lymphatics) | 40–45 mmHg |
| Plasma colloid osmotic pressure | ~25–28 mmHg |
| Normal PCWP | ~7 mmHg |
Key Differentiating Points: Cardiogenic vs. ARDS
| Feature | Cardiogenic | ARDS |
|---|---|---|
| PCWP | >18 mmHg | ≤18 mmHg |
| PaO₂:FiO₂ | Variable | <300 (ALI), <200 (ARDS) |
| CXR distribution | Perihilar, dependent | Diffuse, bilateral |
| BNP | Markedly elevated | Normal/mildly elevated |
| Protein in edema fluid | Low (transudate) | High (exudate) |
| Response to diuretics | Rapid | Minimal |
Sources:
- Guyton and Hall Textbook of Medical Physiology (Pulmonary Edema Safety Factor)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Pathology, Classification)
- Murray & Nadel's Textbook of Respiratory Medicine (Treatment, Vasodilators, Diuretics)
- Morgan & Mikhail's Clinical Anesthesiology (ARDS, Noncardiogenic)
- Tintinalli's Emergency Medicine (Hypertensive Pulmonary Edema)
- Rosen's Emergency Medicine (CKD/ESRD management)
This is a shared conversation. Sign in to Orris to start your own chat.